
Abstract
Abstract
Background:
The aim of this study is to compare the feasibility and oncologic safety of Single–incision, gasless, Endoscopic trans-axillary bilateral Total thyroidectomy (SET) with open cervical total thyroidectomy in patients with papillary thyroid carcinoma (PTC).
Materials and Methods:
From March 2008 to December 2012, PTC patients underwent bilateral total thyroidectomy. Conventional, open surgery was performed on 538 patients (Group O) and endoscopic surgery was performed on 200 patients (Group E). We analyzed the patient's clinicopathologic, postoperative complications, and surgical completeness.
Results:
The mean ages of the patients were 48.9 ± 0.5 (range = 24–77) in Group O and 39.5 ± 0.8 (range = 17–73) in Group E with statistical significance (P < .001). Percentage of female patients were 74.3% in Group O and 96.0% in Group E with statistical significance (P < .001). The postoperative hospital stay in Group O was significantly longer than Group E (4.60 ± 0.05 versus 3.30 ± 0.05; P < .001). The operation time in Group E was significantly longer than Group O (93.9 ± 1.3 versus 142.6 ± 3.3; P < .001). More transient hypocalcemia was found in Group O compared to Group E with statistical significance (28.1% versus 22.4%; P < .001). There were no significant differences with respect to permanent hypocalcemia, permanent recurrent laryngeal nerve palsy, seroma, and hematoma. The mean 1 year-stimulated sTg was 0.23 ± 0.03 and 0.18 ± 0.02 in Group O and E, respectively. Tumor recurrence during short-term follow-up at neck ultrasonography (1 year) was detected in 4 patients in Group O.
Conclusion:
SET is safe and effective, not only for low-risk patients with early-detected cancer, but also for selected cases of advanced cancer.
Introduction
T
Since first report of endoscopic thyroid surgery was published in 1997, 5 approaches for endoscopic thyroidectomy have been examined. The endoscopic trans-axillary approach used by Ikeda et al. in 2000 6 has several benefits; a wide operation field with the same surgical view as open surgery, and, ready accessibility to the thyrothymic ligament, facilitating neck node dissection in the central compartment. However, this approach has several drawbacks for bilateral total thyroidectomy. The lack of view of the contralateral side of the thyroid, or the remnant tissue after thyroidectomy, makes it difficult to apply to some patients, and also difficult for less experienced surgeons to perform. Therefore, application of the endoscopic trans-axillary method has recently focused on lobectomy for papillary thyroid microcarcinoma. 7 Only a few cases have used the endoscopic trans-axillary method for bilateral total thyroidectomy. 8 However, the improvement in surgical technique makes endoscopic bilateral total thyroidectomy via axilla to be used widely.
Therefore, the goal of this study was to evaluate the feasibility and oncologic safety of Single-incision, gasless, Endoscopic trans-axillary bilateral Total thyroidectomy (SET) in patients with papillary thyroid carcinoma (PTC), and to compare the outcomes with conventional, open cervical total thyroidectomy.
Materials and Methods
Study subjects
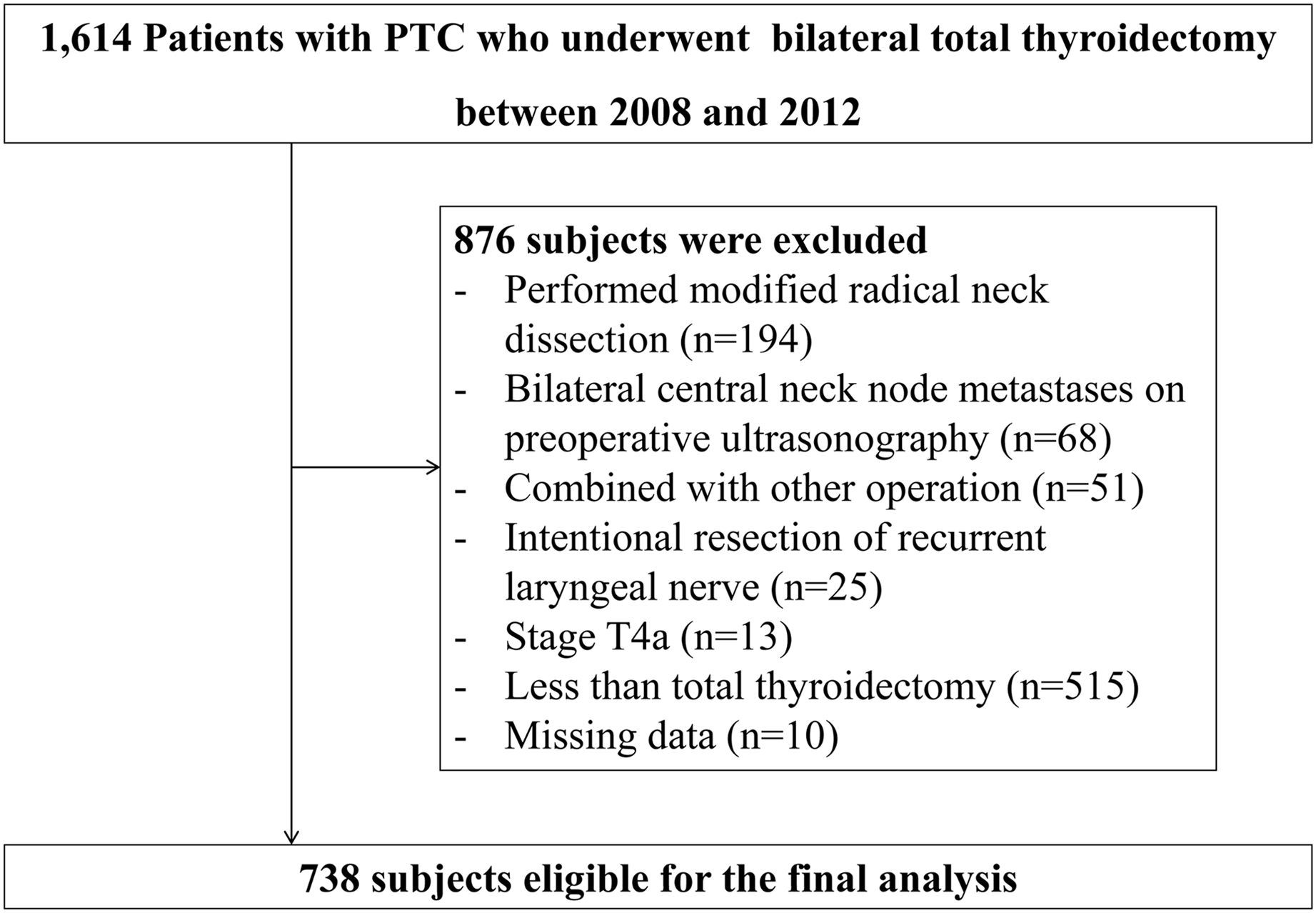
From March 2008 to December 2012, 1614 patients with PTC underwent bilateral total thyroidectomy at Department of Surgery in Kangbuk Samsung Hospital and Severance Hospital. Cases with lateral neck node metastases or distant metastasis who required modified radical neck dissection, bilateral central neck node metastases on preoperative ultrasonography (USG), combined with other operation, intentional resection of recurrent laryngeal nerve (RLN) invasion, and less than total thyroidectomy were excluded. A total of 738 subjects were included in the final analysis (Fig. 1). Open cervical surgery was performed on 538 patients (Group O). SET was performed on 200 patients (Group E). The recommendations for endoscopic surgery used by our institutions were (1) age <45 years, (2) stage T1, T2, or T3, (3) suspicious ipsilateral central neck node metastasis (stage N0 or N1a), and (4) approach desired by the patient.
Selection of study subjects.
Preoperative diagnosis of a thyroid tumor was based on fine-needle aspiration cytology and high resolution USG. Patients with thyroid cancer >1 cm with multiple lesions, bilateral lesions, extracapsular extension during surgery, clinically apparent metastatic disease to nodes (clinical N1), a history of head or neck radiation therapy, or a first-degree familiar history of thyroid cancer, underwent bilateral total thyroidectomy.
All operations were conducted by surgeons, each with at least 10 years of experience. Prophylactic ipsilateral central compartment node dissection (CCND) was done for all the cases. We defined transient hypocalcemia and transient RLN injury based on the recovery from symptoms and normalization of laboratory data within 6 months. All patients were administered levothyroxine after thyroidectomy, for hormonal replacement and thyroid stimulating hormone (TSH) suppression. Radioactive iodine (RAI) therapy was recommended for PTC patients with extrathyroid extension, multiplicity, bilaterality, and lymph nodes metastasis based on American Thyroid Association (ATA) guidelines. 9 The patients who satisfied the indications underwent RAI therapy 4–6 weeks after bilateral total thyroidectomy. A postablation whole body scan (WBS) was performed 5–7 days after the administration of 131RAI. Based on ATA guidelines and several other reports, we measured stimulated serum Tg (sTg) level 1 year after completion of thyroidectomy and RAI ablation therapy, and defined <2 ng/mL as an indicator of surgical completeness.10,11 Neck USG was performed 1 year after remnant ablation for tumor recurrences. All patients performed neck USG, except 8 patients in Group O and 10 patients in Group E, who were lost during follow-up period. We assessed postoperative pain directly based on visual analog scale (VAS) pain scores.
Operative methods
Endoscopic procedure
The patient was placed in a supine position with pillow under the neck for extension. The arm on the lesion side was raised above the head and held parallel to the midline extending from the hyoid bone and to the sternal notch. A 5–6 cm vertical skin incision was made in the lateral side of the pectoralis major muscle at the axilla (Fig. 2). A standardized endoscopic procedure by axillary approach is well described on a review article by Linos. 12 Our surgical methods are based on techniques that are described in this article. The route to the anterior neck area was dissected through the anterior surface of pectoralis major muscle, using an electric cautery under direct vision, until the sternocleidomastoid (SCM) muscle was exposed. The dissection was made from the sternal notch toward the hyoid bone, to minimize bleeding and injury of the flap. Once the clavicular and sternal heads of SCM muscle were exposed, a right angle retractor or cuda retractor (with light source attached) was placed in the space between the SCM branches (Fig. 3). The exposed strap muscle was dissected laterally, then the omohyoid muscle was pushed below the strap muscle. A Chung's retractor was inserted through the axilla to create working space.
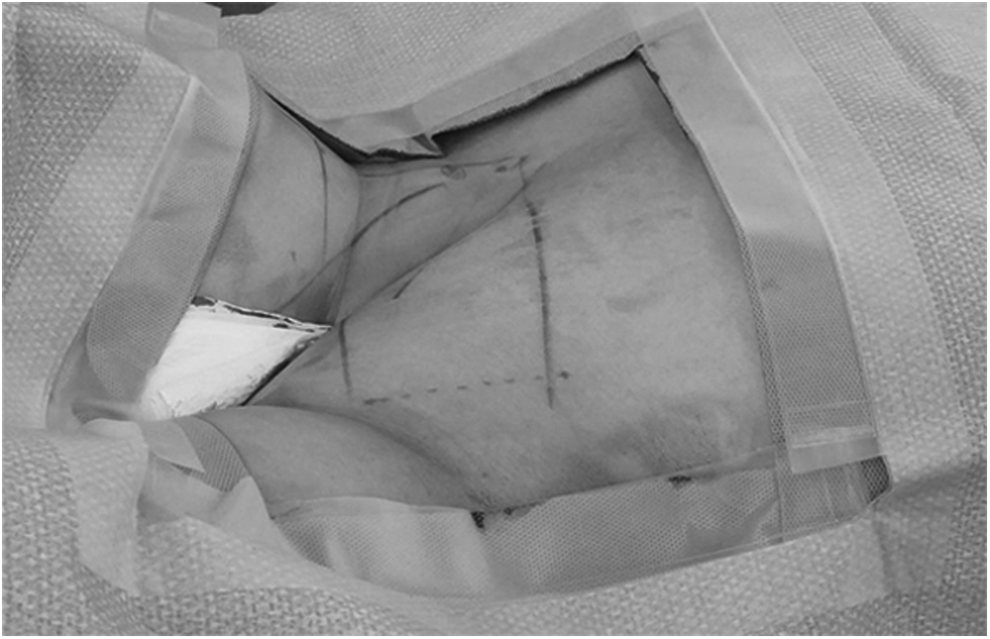
The patient in supine position with the arm on the lesion side raised. A 5–6 cm vertical skin incision was made in lateral side of pectoralis major muscle.

The incision approaches the avascular space between the SCM branches. SCM, sternocleidomastoid.
A 12 mm port was fixed 1–2 mm from the uppermost margin of the axillary incision, then a 45° rigid endoscope was inserted through the port. Under endoscopic guidance, the trachea was visualized parallel to the operation field, and the thyroid gland was exposed. The shielding blade of an ultrasonically activated scalpel (Harmonic scalpel; Johnson & Johnson, Cincinnati) was placed downward to protect the cricothyroid muscle. The upper pole of the thyroid was drawn downward, and the superior thyroid vessels were individually ligated; using the harmonic scalpel, to avoid injury to the external branch of the superior laryngeal nerve. The lower pole was dissected to the thyrothymic ligament, and then the inferior thyroid vessels were dissected. The thyroid gland was retracted medially using endoscopic grasper, and the carotid sheath was sharply dissected using an endoscopic dissector to trace the RLN. The middle thyroid vein was then ligated. The RLN adjacent to Berry's ligament, protected by covering it with gauze. The entire cervical course of the RLN was then traced, and the inferior thyroid vein, located 1 cm superior to RLN, was ligated (Fig. 4). The ipsilateral side of thyroid gland was then dissected from the trachea. When a CCND (the prelaryngeal, pretracheal, and paratracheal area of the tumor side) was required, soft tissue and lymph nodes were detached from the thyrothymic ligament area with the superior-medial retraction of the thyroid.

The dissection follows the entire cervical course of the recurrent laryngeal nerve.
Instead of making additional skin incision, the dissection continued to the contralateral side of thyroid gland. The contralateral side of thyroid gland was detached from the strap muscle, using the harmonic scalpel. The contralateral thyroid lobe was then detached from the trachea (Fig. 5), and the dissection proceeded into the avascular space between the thyroid gland and cricothyroid muscle. The upper pole of the thyroid was drawn downward, and the superior thyroid vessels were individually ligated. Medial traction was applied to the thyroid, and the dissection proceeded to the lower pole of the thyroid to locate the RLN. The thyroid was pulled upward, and detached along Berry's ligament to avoid injuring the RLN.
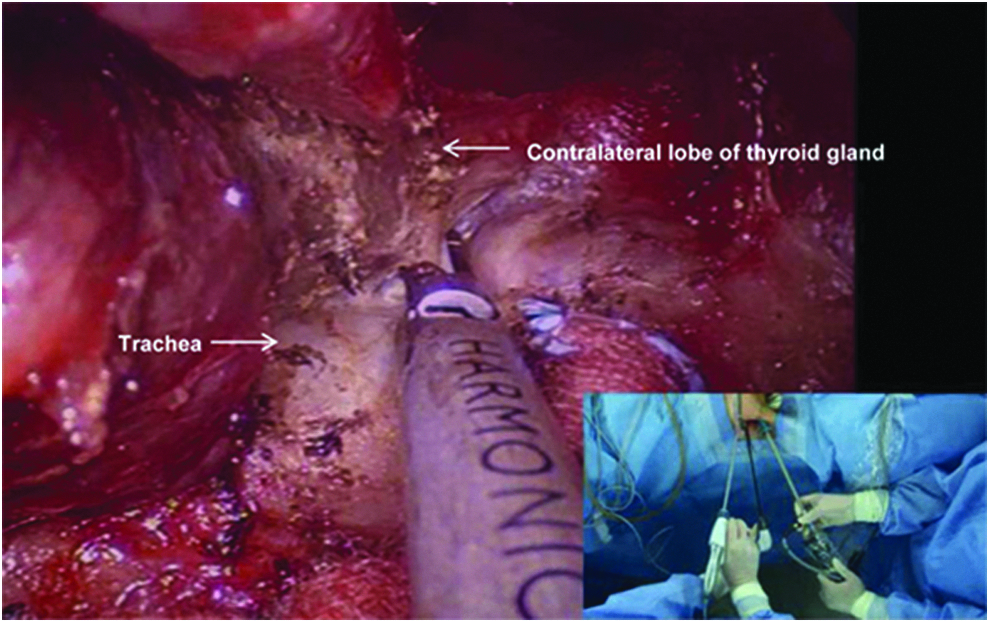
The contralateral side of thyroid gland is detached from the trachea.
To avoid bleeding and adhesion, Tisseel fibrin sealant (Dalim, Seoul, Korea) and HyFence (CHA Bio & Diostech, Seoul, Korea) were applied to the detachment sites of the thyroid gland, trachea, and SCM muscle. Fluid collected in cervical area level V was removed using a suction catheter. A closed suction drain was inserted to the detachment site of the thyroid gland and fixed at 2 cm distal from the inferior margin of the wound. The subcutaneous fascia was closed with absorbable Vicryl sutures (Vicryl 4–0; Ethicon, Johnson & Johnson, Somerville) and the subcuticular layer was closed with 5-0 Maxon sutures (Covidien Pty. Ltd., Melbourne, Australia). The skin was closed with a 3M™ steri strip (3M, St. Paul).
Open procedure
The patient was placed in a supine position with the neck extended. A 6–8 cm transverse skin incision was made two fingers above the sternal notch and a subplatysmal flap dissection was performed from the hyoid bone to the sternal notch. A vertical incision was made on the midline of the strap muscle to expose the thyroid gland. A bilateral total thyroidectomy, CCND, and wound closure were performed in the same manner as the endoscopic procedure.
Statistical analyses
Characteristics of Groups O and E were compared using the Student's t-test for continuous variables and the Pearson χ2 test, Fisher's exact test for categorical variables. Means and standard errors are shown in the tables. Multivariate regression analysis was performed for operation time, postoperative complications, and surgical completeness after adjusting for the differences in demographics, pathological and other clinical characteristics of the patients with logistic regression model. Differences between groups were considered significant at P < .05. All statistical analyses were performed using the SPSS software (SPSS version 12.0, Chicago, IL).
Results
Baseline characteristics of the study population
The clinicopathologic characteristics, postoperative complications, and surgical completeness of the two groups are shown (Tables 1 and 2). Group O consisted of 538 patients and Group E consisted of 200 patients.
Values are number of individuals (n) or mean ± SE.
Student's t-test.
Pearson's chi-square test.
SE, standard error; VAS, visual analog scale.
Values are number of individuals (n) or mean ± SE.
Student's t-test.
Pearson's chi-square test.
Fisher's exact test.
AJCC, American Joint Committee on Cancer; SE, standard error.
The mean ages of the patients were 48.9 ± 0.5 (range = 24–77) in Group O and 39.5 ± 0.8 (range = 17–73) in Group E with statistical significance (P < .001). Percentage of female patients were 74.3% in Group O and 96.0% in Group E with statistical significance (P < .001). The postoperative hospital stay in Group O was significantly longer than Group E (4.60 ± 0.05 versus 3.30 ± 0.05; P < .001). The operation time in Group E was significantly longer than Group O (93.9 ± 1.3 versus 142.6 ± 3.3; P < .001). The postoperative VAS score did not differ between the two groups. The mean tumor size in Group O was significantly smaller than Group E (0.93 ± 0.02 versus 1.03 ± 0.04; P = .025). The mean number of the retrieved lymph nodes in Group O was 7.10 ± 0.24 and 5.46 ± 0.25 in the Group E (P < .001). Percentage of extrathyroid extension were 69.5% in Group O and 55.5% in Group E with statistical significance (P < .001). When comparing with respect to multiplicity and bilaterality of the tumor, Group E had more multiplicity and bilaterality compared to Group O (27.1% versus 39.3%; P = .001) (21.4% versus 29.9%; P = .016). Three hundred two patients (56.1%) of Group O were stage III and 159 patients (79.5%) of Group E were stage I (P < .001). There were no significant differences with respect to number of cervical lymph node metastasis and pN stage between the two groups.
Postoperative complications of the study population
The postoperative complications of both groups are shown in Table 3. More transient hypocalcemia was found in Group O compared with Group E with statistical significance (28.1% versus 22.4%; P < .001). More transient RLN palsy was found in Group E compared to Group O with statistical significance (4.6% versus 15.0%; P < .001). There were no significant differences with respect to permanent hypocalcemia, permanent RLN palsy, seroma, and hematoma.
Pearson's chi-square test.
Fisher's exact test.
RLN, recurrent laryngeal nerve.
Surgical completeness of the study population
Previous studies considered postoperative serum Tg levels under TSH suppression as determinants of surgical completeness.13,14 One year-stimulated sTg was analyzed in patients who underwent 131RAI therapy. 87.4% and 83.0% of Group O and E underwent 131RAI therapy and the mean one year-stimulated sTg was 0.23 ± 0.03 and 0.18 ± 0.02, respectively without statistical significance. Tumor recurrence during short-term follow-up at neck USG (1 year) was detected in 4 patients in Group O. Abnormal 131I uptake outside the thyroid bed on the WBS was detected in 8 cases and 2 cases in Group O and E, respectively (Table 4).
Values are number of individuals (n) or mean ± SE.
Student's t-test.
Fisher's exact test.
Pearson's chi-square test.
RAI, radioactive iodine; SE, standard error; sTg, serum thyroglobulin; USG, ultrasonography; WBS, whole body scan.
Discussion
This study compares the complications and outcomes between SET and open total thyroidectomy. The advantages of endoscopic procedure include better magnification of the cervical anatomy, lower incidence of postoperative hypesthesia or paresthesia in the neck, less discomfort while swallowing, and improved cosmesis.15,16 Endoscopic procedure has been performed for benign thyroid disease and papillary thyroid microcarcinoma.17,18 However, few studies reported the application of endoscopic bilateral total thyroidectomy for PTC. Kitano et al. described indications for endoscopic thyroidectomy in thyroid carcinoma as (1) age < 45 years, (2) tumor size < 2 cm, and (3) no evidence of lymph node or local invasion. 19 The recommendations used by our group were (1) age < 45 years, (2) stage T1, T2, or T3, (3) suspicious ipsilateral central neck node metastasis (stage N0 or N1a), and (4) approach desired by the patient. In this study, we found that SET is an effective surgical method for patients with PTC compared to conventional open total thyroidectomy regarding technical safety, oncologic safety, and cosmetic results.
SET provides better cosmetic satisfaction and postoperative pain compared to open total thyroidectomy. Among the various endoscopic techniques, SET provides easier manipulation of the upper and lower poles of the thyroid and better identification of the ipsilateral RLN and parathyroid glands, than the anterior chest approach. SET also results in superior cosmetic results, as there are no scars on the neck or anterior chest. 12 The small scarring in the axilla is completely covered by the arm in its natural position. 8 The higher proportion of female patients in Group E reflects their preferences for better cosmetic outcome. Our data show that there was no difference in postoperative pain between two groups (Table 1). In the past, several authors mentioned that since there is a much larger plane of tissue dissection in SET, it results in significantly more pain during the postoperative period.20,21 However, recent studies show less or no difference in postoperative pain between trans-axillary and open thyroidectomy.22,23 Since trans-axillary approach does not require anterior neck flap dissection, it leaves minimal degree of postoperative hyperesthesia or paresthesia in the neck. 24 It also leaves little discomfort while swallowing because it prevented adhesion between the strap muscle and sub-platysma muscle flap created during conventional open thyroidectomy. 25
The oncologic safety of the endoscopic method was assessed using several factors. Based on postoperative stimulated serum Tg levels under TSH stimulation as an indicator of surgical completeness, there was no significant difference between Groups O and E 1 year after surgery, that is, there was no difference in the level of remnant thyroid tissue. There was no difference on number of recurrent cases, abnormal uptake outside the thyroid bed on the WBS between two groups (Table 4). Overall, success of the endoscopic approach reported herein corresponds well with that of Kang et al., who found no local recurrence or distant metastasis in 581 cases of gasless trans-axillary endoscopic thyroidectomy. 26
In terms of technical safety, Group E had less transient hypocalcemia compared to Group O (Table 3). However, incidence of transient hypocalcemia and transient RLN palsy in Group E were slightly higher than reported in previous studies. 26 This could be explained by our lack of experience in the early cases. One of the pitfalls of SET was that approach to the contralateral superior pole of the thyroid is difficult.6,27 However in recent cases, we overcame the issue regarding the safe dissection of the opposite lobe. First, we conducted dissection of anterior thyroid surface for the making of working space until contralateral lobe is exposed. We then used 45° endoscope, which enables us to see downward easily. There was little difficulty to identify the contralateral superior pole of thyroid. Second, since SET provides multiple pivot points while maintaining stability, we minimized the operator-induced tremor issue. In set, the scope is positioned upper most and anterior half part of space. Other endoscopic devices, such as grasper and harmonic scalpel, manipulated by the operator are located in posterior half of space. This enables the operator to work on half of spaces with multiple pivot points. Multiple pivot points make easy manipulation of endoscopic devices while maintaining steady position. At last, even though more incidence of seroma was reported in Group E, due to wider dissection of skin flap in trans-axillary approach, it will be overcome by effort to make smaller dissection of flap in the future.
Since trans-axillary endoscopic thyroidectomy is more technically demanding, the learning curve duration is known to be longer than conventional open thyroidectomy. Kwak et al. reported that the operation time decreased from the 60th case of endoscopic unilateral lobectomy and the 38th case for endoscopic total thyroidectomy. 28 Liu et al. demonstrated that proficiency with the operation reached the advanced level after 150 cases. 29 In our cases, the surgeons are performing endoscopic thyroidectomy without any difficulties due to the experience of performing more than 800 cases of endoscopic surgery for 6 years. Every case should be treated with caution to avoid surgical morbidities.
Our study has a few limitations. First, because treatment was based on preoperational observations and patient preference, the treatment strategy was not randomized. Second, the number of patients who underwent endoscopic surgery was relatively small. Larger, multicenter, randomized, prospective studies are necessary in the future. Third, cosmetic satisfaction was not compared for Groups O and E. Finally, comparison of long-term oncologic safety requires follow-up period of at least several years. Despite these limitations, our study is worthwhile in that we compared surgical techniques, postoperative complications, and oncological safety of SET thus examining the benefits of SET over open total thyroidectomy.
Our study did not include pT4a or pN1b patients on Group E. A recent study, however, extended indications by performing selective lymph node dissection and modified radical neck node dissection in endoscopic method. 30 In conclusion, SET is safe and effective, not only for low-risk patients with early-detected cancer, but also for selected cases of advanced cancer. With future advances in surgical skills and endoscopic instruments, the use of endoscopic thyroid surgery can be extended to the treatment of advanced cases such as pT4a or pN1b cancers.
Footnotes
Disclosure Statement
No competing financial interests exist.