
Abstract
Abstract
Background:
An optimal alimentary tract reconstruction technique after laparoscopic total gastrectomy (LTG) remains controversial. The authors developed a new simple technique for intracorporeal esophagojejunal anastomosis that employs a conventional purse-string suture instrument (PSI) and circular stapler.
Methods:
From May 2014 to April 2016, 41 consecutive patients with gastric cancer underwent LTG in the author's institution. Intracorporeal esophagojejunal anastomosis using the following method was attempted for all patients. After total gastrectomy was completed laparoscopically, a small vertical incision (about 40 mm) was created at the left midclavicular line and retracted by a wound retractor. An anvil of a 25 mm circular stapler was introduced into the abdominal cavity. Then a previously prepared surgical glove, which was cut open at the thumb and the little finger through which the two hand shafts of the PSI were passed separately and sealed by ties, was attached to the wound retractor to maintain airtightness, and the PSI was introduced into the abdominal cavity. The following procedure was similar to conventional open surgery except that it was performed under laparoscopic vision.
Results:
Intracorporeal esophagojejunal anastomosis was performed successfully for all 41 patients. No case required extension of the initial incision for difficulties during anastomosis. The mean operation time was 245 minutes, and the mean time for the purse-string suture and anvil placement was 15 minutes. Tumor-free margins were achieved in all 41 patients. There were no anastomosis-related complications or other major surgical complications.
Conclusions:
With the described method, intracorporeal esophagojejunal anastomosis can be performed easily and safely.
Introduction
L
In conventional open total gastrectomy, the standard reconstruction method uses a purse-string suture instrument (PSI) and circular stapler for esophagoenteral anastomosis. However, conventional PSIs and circular staplers were not developed for intracorporeal anastomosis, and thus have been unavailable during LTG. Some surgeons have used an extracorporeal approach through a minilaparotomy for esophagojejunostomy, which is similar to conventional open surgery.4,5 However, in this technique, it is sometimes difficult to complete the anastomosis because of the narrow and deep operating fields, especially for patients who are obese or have a large anteroposterior diameter, and extension of the incision for laparotomy may be required. Intracorporeal anastomosis under laparoscopic vision appears to be a better choice; however, the technical problem is how to place and fix the anvil head at the esophageal stump laparoscopically. Some alternative methods to overcome this technical problem have been reported. However, an optimal procedure for esophagojejunostomy is yet to be established.
A conventional circular stapler may be used for intracorporeal anastomosis by the glove method under maintenance of pneumoperitoneum, and this procedure inspired us to devise a new simple method of purse-string suture placement using conventional PSI. Herein, we describe the details of the procedure and the short-term outcomes of the initial series.
Patients and Methods
Patients
From May 2014 to April 2016, a total of 41 consecutive patients (28 men and 13 women) with gastric cancer underwent LTG using conventional PSI for intracorporeal circular stapled esophagojejunostomy in our institution. These patients had a median age of 61.7 years (range 35–82 years) and a median body mass index of 28.5 kg/m2 (range 18.3–33.4 kg/m2). Inclusion criteria were as follows: histologically confirmed gastric adenocarcinoma located in the upper third of the stomach with or without invasion to the intraabdominal esophagus of <30 mm, and without adjacent organs or distant metastasis. Both early and advanced gastric cancers were included in this study.
Informed consent was obtained from each patient before surgery in all cases. The Institutional Review Board of Qingdao University approved this retrospective study.
Surgical techniques
Before the operation, the instruments were first prepared. Two surgical gloves were needed. One was for the circular stapler, prepared in the usual way, and the other was cut open at the thumb and the little finger, through which the two hand shafts of the PSI were passed separately and sealed by ties (Fig. 1a–c), appearing as if trousers were put on the PSI.

Surgical glove prepared for the PSI and attached to the wound retractor
Under general anesthesia, the patient was placed in the split-leg supine position. The surgeon stood on the right side of the patient, with the first assistant on the left side and the laparoscope operator between the patient legs. A 10-mm camera port was introduced below the umbilicus, and the pneumoperitoneum was established. Four additional ports were created in the upper abdomen, as shown in Figure 2.
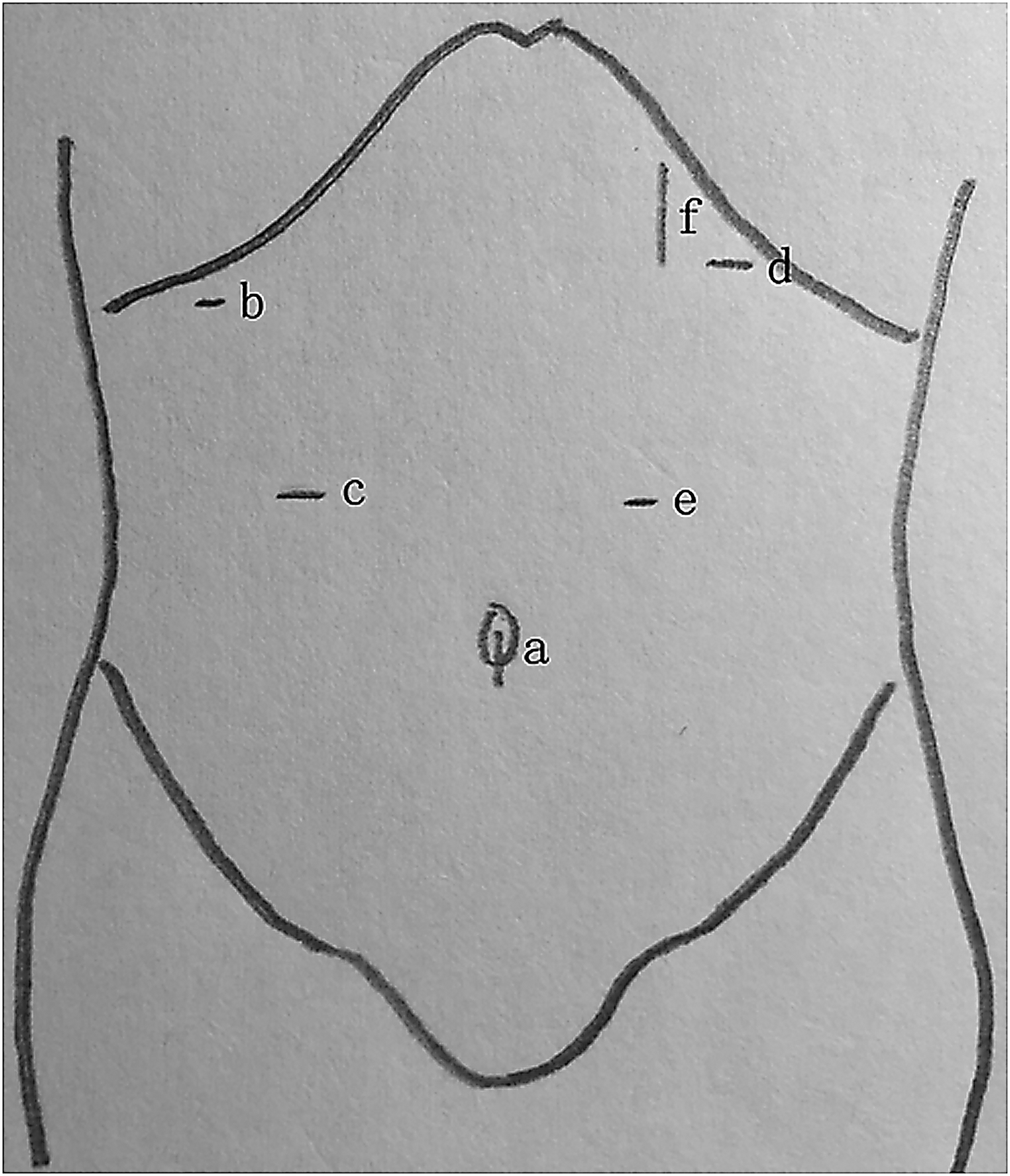
Trocar placement. a, 10-mm umbilical port for the scope; b and e, for 5-mm ports; c and d, for 12-mm ports; f, for 40-mm minilaparotomy after a laparoscopic total gastrectomy.
To ensure exposure around the abdominal esophagus, the left lobe of the liver was retracted by a method similar to that described by Sakaguchi et al. 6 After radical lymphadenectomy and full mobilization of the stomach, the abdominal esophagus was exposed completely and transected perpendicularly with a 45-mm linear stapler (ETS Flex45; Ethicon Endo-Surgery, Cincinnati, OH) on the oral side of the esophagogastric junction. Then, a vertical incision about 40 mm, depending on the diameter of the mass, was created at the left midclavicular line and was retracted and protected by a wound retractor before the stomach was extracted, and an anvil of a 25-mm circular stapler (ECS; Ethicon Endo-Surgery) was introduced into the abdominal cavity by minilaparotomy. The location of the incision is crucial in this technique because the PSI will be attached to the esophagus stump by this small incision. An incision just below the costal margin is essential. In contrast, as the jaws of the PSI contain an obtuse angle, an incision around the left midclavicular line provides the optimal angle for attaching the PSI to the esophagus stump.
The previously prepared surgical glove with PSI was attached to the wound retractor to maintain the pneumoperitoneum, and the PSI was introduced into the abdominal cavity (Fig. 1d). The esophagus stump was gently retracted by two bowel forceps, and attachment of the PSI was achieved with ease under laparoscopic vision (Fig. 3a). The conventional purse-string suture with two straight needles was then introduced into the abdominal cavity and inserted through the entrance hole of the PSI from left to right laparoscopically (Fig. 3b). Next, the esophagus stump was transected with laparoscopic scissors distal to the PSI clamping line before the PSI was removed, the proximal resection margin was obtained, and frozen biopsy was performed (Fig. 3c). After we confirmed a negative resection margin, the following esophagojejunal anastomosis was performed. The esophageal lumen was opened gently toward the right and left by bowel forceps, and the anvil head was introduced using an endoscopic anvil grasper from its rim similar to fastening a button. Once the anvil was in place, the purse-string suture was tied first with a surgeon knot, and additional knots were made to secure the anvil (Fig. 3d). In all cases, a monofilament pretied loop (Endoloop; Ethicon Endo-Surgery) was applied to reinforce the ligation.
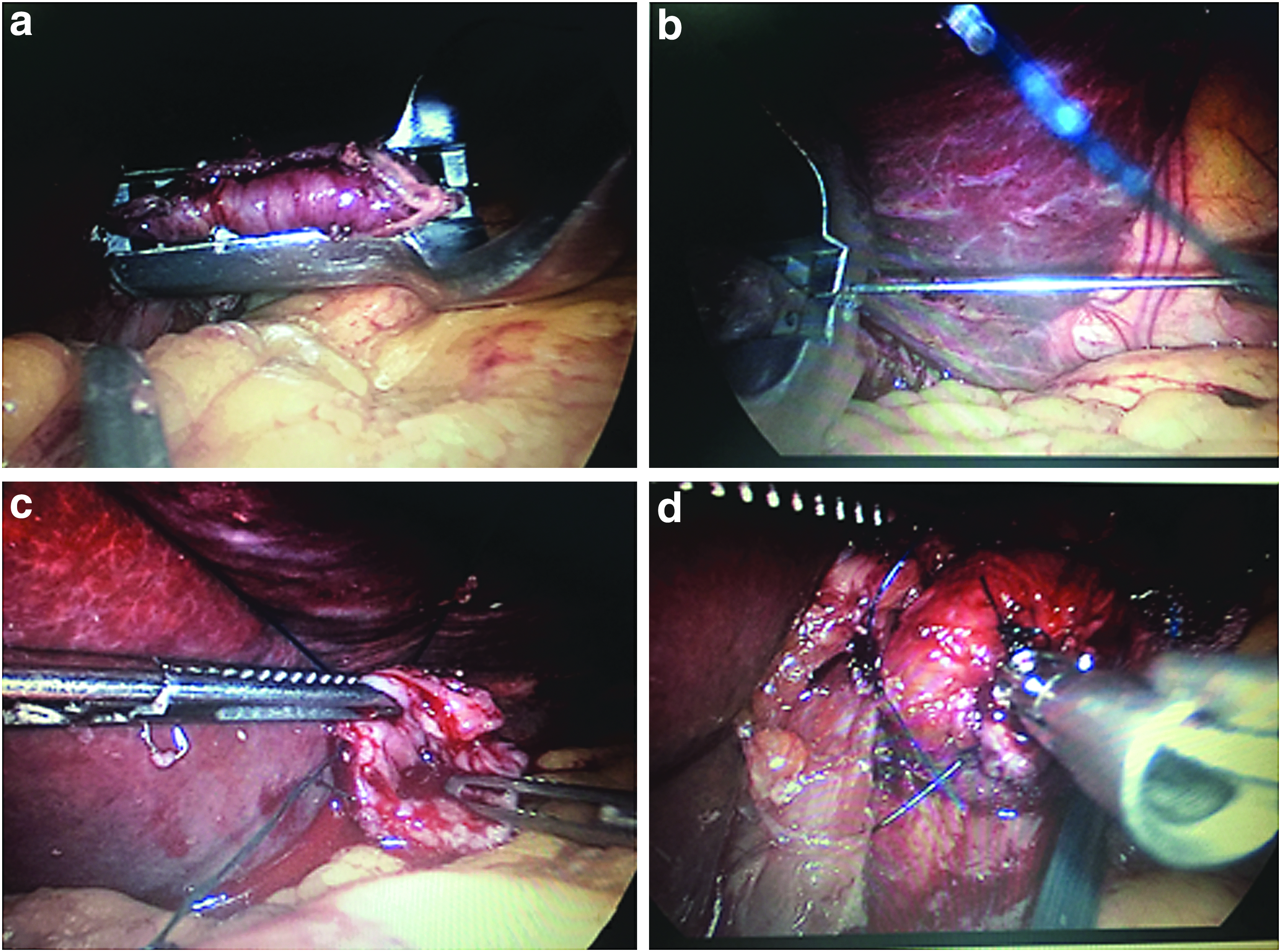
Purse-string suture placement and anvil fixation
Reconstruction was performed by the Roux-en-Y method. The jejunojejunal anastomosis was performed intracorporeally, and the distal limb of the jejunum was brought up anteriorly to the colon. The previously prepared surgical glove with circular stapler was attached to the wound retractor to maintain pneumoperitoneum after the body of the circular stapler was inserted into the distal limb of the jejunum, which was tied by an elastic tape to prevent slippage of the jejunum from the circular stapler. Pneumoperitoneum was reestablished, and the tip of the circular stapler was introduced into the abdominal cavity and combined with the anvil head under laparoscopic vision. The circular stapler was withdrawn after firing. Finally, the jejunal stump was closed laparoscopically with a 45 mm endoscopic linear stapler (ETS45; Ethicon, Endo-Surgery).
Results
All the patients successfully underwent the aforementioned operation. No case required conversion to open surgery or extension of the initial incision for difficulties during anastomosis. The pathological stages were stage I in 10 (24.4%) patients, stage II in 27 (65.9%) patients, and stage III in 4 (9.7%) patients. The mean operation time was 245 minutes (range 210–320 minutes) and the mean time for the purse-string suture and anvil placement was 15 minutes (range 10–25 minutes). The average estimated blood loss was 85 mL (range 50–110 mL). Tumor-free margins were achieved in all 41 patients. The mean postoperation hospital stay of patients was 5.2 days (range 4–7 days). The surgical results are summarized in Table 1.
Means (range).
LTG, laparoscopic total gastrectomy.
One patient experienced pneumothorax intraoperatively. High airway pressure and reduced respiration in the left lung were detected by the anesthetist before the esophagoenteral anastomosis was established. A 10-mm defect on the left pleura was discovered, and intracorporeal hand sutures were performed. The patient was discharged 5 days later with an uneventful postoperative course. Another patient had intraperitoneal bleeding on postoperative day 2 and required only conservative management. No other surgical complications such as postoperative anastomotic leakage, stenosis, or duodenal stump leakage were observed during the median follow-up period of 17 months (range 6–28 months).
Discussion
One of the most important issues regarding gastrointestinal surgery is the reconstruction technique, especially when the anastomosis site is located near the two ends of the alimentary tract, such as esophagojejunostomy after total gastrectomy and colorectal anastomosis after low anterior resection. Both of the anastomoses are technically demanding because of the physical constraints of a narrow and deep operating field, regardless of that in open or in laparoscopic surgery. Unlike the laparoscopic colorectal anastomosis, in which the double stapling technique has been the standard method, an optimal intracorporeal esophagojejunostomy technique remains controversial. Many anastomosis techniques for intracorporeal esophagojejunostomy have been developed (summarized here in Table 2) and can be categorized into those employing linear staplers and those using circular staplers. In addition, laparoscopic hand-sewn esophagojejunal anastomosis has been reported, 13 but is not discussed in this article because it is really a difficult and time-consuming process and is thus difficult to popularize.
PSI, purse-string suture instrument.
Esophagojejunostomy with linear stapling devices was first reported by Walther et al. in open surgery and was utilized laparoscopically by Uyama et al.7,14 Since then, many studies regarding this novel technique have been reported with good outcomes, including functional end-to-end anastomosis, the overlap method, and other modified techniques.12,15–17 This technique has several advantages. First, it abolishes the need for a purse-string suture and the insertion of an anvil into the lower esophagus, both of which are time-consuming and technically challenging procedures in laparoscopic surgery, especially in the case of a narrow esophagus. Furthermore, it creates a significantly wider anastomosis, which reduces the risk of the development of anastomotic stenosis. However, this technique has the additional limitation of requiring sufficient esophageal length to secure the distance for anastomosis and necessitates bringing more of the esophagus down into the mediastinum, which may carry a potential risk of damaging the blood supply of the distal esophagus and result in anastomosis leakage and subsequent mediastinitis. In particular, when the esophagus has been invaded by the tumor and more proximal esophagus needs to be transected, manipulation using an endoscopic linear stapler becomes increasingly difficult. Therefore, although Uyama and colleagues recommended the overlap method for gastric cancer with invasion into the introabdominal esophagus of <20 mm, 12 some groups have suggested that esophagojejunal linear-stapled anastomosis should not be applied to patients with tumors that have invaded the esophagus.18,19
The creation of esophagojejunostomy using a circular stapler is the most frequently used technique in open surgery. The obvious advantage of using a circular stapler laparoscopically is that surgeons are already familiar with the devices and know the detailed technical tips on how to use them. Another merit of this technique is that it can be applied in cases with esophageal invasion of the tumor, as far as 30 mm from the esophageal gastric junction.
Many different types of anastomosis techniques using circular stapling devices for intracorporeal esophagojejunostomy have been reported and can be divided into those using double (or hemidouble) stapling techniques and those using single stapling techniques.9,11,20,21 The former employs one linear stapler and one circular stapler to achieve the esophagojejunal anastomosis, which omits the time-consuming purse-string suture. An anvil insertion can be accomplished by using the “oral-to-abdomen” method or the “abdomen-to-oral” method. 22 OrVil (Corviden, Mansfield, MA), a newly developed transoral pretitled circular anvil, which is positioned by the oral-to-abdomen method, has been used in the reconstruction of the digestive tract involving the esophagus with favorable efficacy. 10 As for the abdomen-to-oral method, the anvil is inserted through a small hole, which is made on the anterior wall of the esophagus at the distal area from a planned transection line, and transection of the esophagus is performed using a linear stapler, while the hole is approximated and the anvil is fixed at the esophageal edge. 21 The possibility of the intraabdominal or intraluminal spread of cancer cells would be a concern in this technique, especially in cases with tumors near the esophagogastric junction.
The double stapling technique is the standard procedure for reconstruction of the sigmoid colon and the rectum despite the fact that in colorectal surgery, the double stapling technique has a much higher rate of stenosis than the single stapling technique, even when a stapler of the same size is used.23,24 However, situations are different with esophagojejunostomy, in which postoperative anastomotic stenosis becomes a particular problem as the lumen of the esophagus is much smaller than that of the rectum. Similar to that in colorectal surgery, anastomosis stenosis and leakage in LTG tend to occur more frequently with the double or hemidouble stapling technique than with the single stapling technique. Overlap of stapler lines may have some role in anastomosis stenosis because of the possibility that local ischemia at the site where the staple lines meet may result in the development of anastomotic stenosis because of fibrosis. 25 Therefore, the single stapling technique should be the preferred method in the circular stapled esophagojejunostomy to minimize postoperative complications.
It is necessary to place a purse-string suture for the single stapling technique; however, that is still thought to be a difficult procedure under laparoscopic vision. Kinoshita et al. have reported using a hand-sewn purse-string suturing technique in a manner similar to that used in open surgery. 11 This procedure is technically demanding and difficult to perform even by surgeons familiar with intracorporeal suturing and knot-tying techniques. A new device, Endo-PSI, which was designed especially for purse-string suturing in LTG, was reported by Usui et al. with good outcomes. 9 Unfortunately, this device is not widely available.
Our technique presented in this report is very simple, just a small modification of the glove method described in previous reports; however, it provides another new option to perform esophagojejunostomy intracorporeally, which possesses all the merits of other intracorporeal reconstruction techniques, such as small incisions and excellent surgical view. The mean time for the purse-string suture and anvil placement was 15 minutes in our series, which was comparable with the times reported by other groups.15,26,27 A good quality purse-string suture, which should be well distributed and smooth around the anvil rod after ligation, can be steadily achieved using this technique. Furthermore, the conventional PSI being widely used during traditional operations is familiar to surgeons and available in almost every institution; therefore, this technique has the advantage that it is easy to popularize and is especially useful in countries with limited access to other special or expensive devices such as Endo-PSI and OrVil.
For those cases with tumor invading the lower esophagus, it is always a challenge to reconstruct after the removal of tumor, no matter what kind of technique is applied, because of the narrow working space. We have also tried this technique in such cases and found that it was feasible in gastric cancer with invasion into the introabdominal esophagus of <30 mm, although it was more difficult and a little more time consuming. One of the technical problems of such a procedure using PSI device is driving of a straight long needle in the narrow working space. And, it is even more difficult in the lower mediastinal space for the esophagus-invading tumor. Here are two helpful tips to complete this procedure. First, trying to mobilize and drawing the lower esophagus out of the mediastinum. Second, at the appearance of its tip at the other side of the PSI device, use a needle driver to curl up the straight needle and make it gradually pass through the holes of the PSI device.
The weaknesses of this study are the retrospective nature of this review, the lack of a control group, and the small number of patients, which prevent us from drawing categorical conclusions. Further studies including a larger number of patients and studies that compare with other techniques measuring short-term and long-term surgical outcomes are warranted to evaluate the safety and feasibility of this technique.
Footnotes
Disclosure Statement
No competing financial interests exist.