
Abstract
Abstract
Introduction:
The electrothermal bipolar vessel-sealing device (BVSD) is known to supply a strong vessel-sealing power. However, only few studies have reported lymph node dissection (LND) using only BVSD during laparoscopic surgery for gastric cancer. The purpose of this study was to investigate the feasibility of LND using BVSD during reduced port laparoscopic distal gastrectomy for gastric cancer.
Methods:
From May 2015, patients in whom three- or single-port laparoscopic distal gastrectomy had been engaged for gastric cancer were enrolled in this study. We performed D1+ or D2 LND using only LigaSure™ Maryland (Medtronics, Minneapolis, MN), a recently developed BVSD. Clinical outcomes of these patients were investigated.
Results:
From May 2015 to November 2016, 20 patients were enrolled in this study. The mean operation time was 262.6 ± 36.6 (200–340) minutes. The mean time for LND was 124.7 ± 19.2 (93–171) minutes. Only one patient had a morbidity of Clavien-Dindo grade more than II. No mortality was observed in all patients. The mean number of retrieved lymph nodes was 46.8 ± 22.8 (15–105).
Conclusions:
LND using the Maryland jaw type BVSD was feasible during reduced port (single- or three-port) laparoscopic distal gastrectomy for gastric cancer. Objectively evaluating the potential advantages of BVSD in reduced port laparoscopic surgery is necessary.
Introduction
L
Currently, most surgeons prefer the ultrasonic energy device during laparoscopic surgery for patients with gastric cancer to perform a similarly feasible LND as an open procedure. A characteristic mechanism of the ultrasonic energy device, “cavitation,” also helps surgeons safely perform LND during laparoscopic gastrectomy for gastric cancer. Cavitation is the formation of vapor-filled cavities within cells because of mechanical oscillation of the instrument. 5 Expansion and contraction of these spaces result in tissue dissection. Because surgeons depend on the visual sense during laparoscopic surgery, the cavitation effect provides important clues for LND. This guidance for finding the correct dissection plane helps surgeons avoid critical complications or useless time-consuming procedures.
Meanwhile, how about the electrothermal bipolar vessel-sealing device (BVSD)? In general, BVSD supplies a stronger vessel-sealing power than ultrasonic energy device. 6 LigaSure™ vessel-sealing system (LVSS; Medtronics, Minneapolis, MN), one of the commercially developed BVSDs, can seal vessels up to 7 mm in diameter. 7 Such strong vessel sealing enables surgeons to perform clipless vessel control. However, until recently, BVSD has been regarded as inappropriate for LND in gastric cancer treatment because two critical problems exist in its application. First, it has been difficult to perform a delicate LND with the bulky tip of this device. In addition, unlike the ultrasonic energy device, BVSD does not induce the cavitation effect, and therefore, surgeons cannot expect guidance in identifying the dissection plane.
These drawbacks might be the reason for the few reports of LND using BVSD during laparoscopic surgery for gastric cancer. However, we remarked on a recently issued LVSS product, LigaSure Maryland Jaw type 37 cm laparoscopic instrument (Medtronics). This new BVSD has fine blades on its tip, although its sharpness is not equal to that of ultrasonic energy device.
Inspired by the innovative blade shape, we attempted to apply the Maryland jaw type LVSS in gastric cancer surgery, particularly in reduced port laparoscopic gastrectomy (RPLG). Many surgeons have recently reported the clinical outcomes of RPLG for gastric cancer.8–18 Our institute has also accumulated clinical experience of RPLG for patients with gastric cancer. 19 Based on our expertise, we hypothesized that the strong vessel-sealing power of BVSD can be advantageous in three- or single-port laparoscopic surgery for gastric cancer because the operator encounters all the situations (i.e., unexpected bleeding or unaided vessel ligation) alone. In addition, although the previous jaw type BVSD was not appropriate for LND, the Maryland jaw type BVSD is expected to be efficient in LND for gastric cancer. Therefore, we designed a pilot study to investigate the feasibility of LND using BVSD during reduced port surgery for gastric cancer.
Methods
Study design and participants
This was a single-arm, open-label prospective study conducted in a single institute. From May 2015, we serially enrolled patients for whom laparoscopic surgery had been scheduled for gastric adenocarcinoma. All surgical procedures were performed by one surgeon (C.M.L.), who had the experiences of ∼50 laparoscopic surgeries for gastric cancer, and had been trained in a high-volume center performing more than 700 laparoscopic gastric cancer surgeries per year.
The sample size was planned at 20, and the enrolled patients provided written informed consent for participation in all procedures associated with the study. Our protocol stated that accrual should be suspended if any of the enrolled patients develop the following problems: (1) any postoperative complication that is strongly correlated with LND using only BVSD, (2) any mortality, and (3) the number of retrieved lymph nodes is <15 (in the final pathologic report).
Approval to perform research on human subjects in this study was provided by the Institutional Review Board of Korea University Medical Center Ansan Hospital (registration number: AS16141).
Eligibility criteria
(i) Histologically proven gastric adenocarcinoma.
(ii) Age between 20 and 90 years.
(iii) Clinical stage IA (T1N0M0) based on the Seventh edition of the American Joint Committee on Cancer system 20 (The clinical stage was determined based on the findings of gastrofiberscopy and abdominal computed tomography).
(iv) Possible for R0 surgery by distal gastrectomy with D1+ or D2 lymphadenectomy.
(v) American Society of Anesthesiology (ASA) score of I, II, or III.
(vi) Eastern Cooperative Oncology Group performance status of 0 or 1.
(vii) Scheduled for laparoscopic surgery.
Specific eligibility criteria for single-port laparoscopic surgery
Single-port laparoscopic surgery was performed for patients who additionally met the following conditions:
(i) ASA score of I or II.
(ii) No previous abdominal surgery.
(iii) No history of pancreatitis or peptic ulcer.
(iv) No preoperative endoscopic treatment (i.e., endoscopic mucosal resection or endoscopic submucosal dissection).
Preoperative procedures for three-port laparoscopic surgery
In the operating room, the patient was placed on the bed with both legs abducted under general anesthesia. The bed was adjusted to create a reverse Trendelenburg position for the patient. The operator sat on the right side of the patient, whereas the scopist was positioned between the patient's legs (Fig. 1a).
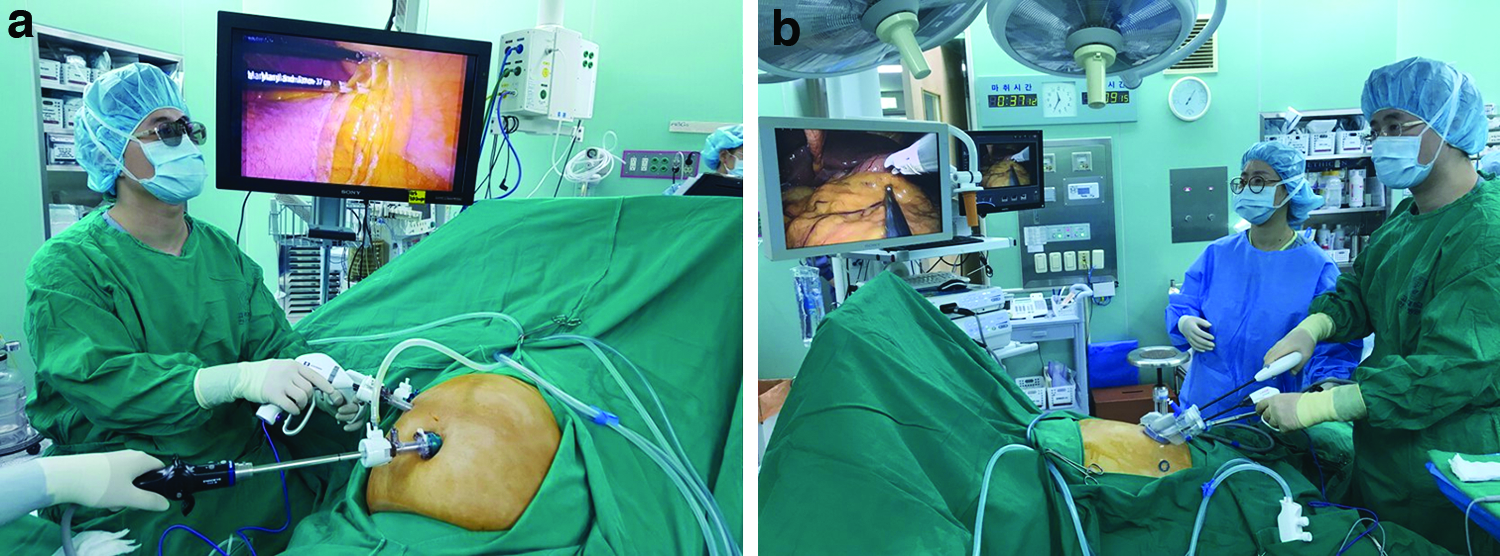
The positions of operator and scopist in reduced port laparoscopic surgery for gastric cancer.
A 12-mm channel trocar was inserted through a transumbilical incision using Hasson's method. 21 After a pneumoperitoneum was created using carbon dioxide at a pressure of 15 mmHg, a flexible scope was inserted through this umbilical port. Under the guidance of flexible scope, one 5-mm channel trocar was established on the right subcostal margin and another 12-mm channel trocar on the right midclavicular line.
Preoperative procedures for single-port laparoscopic surgery
In the operating room, the patient was placed on the bed with both legs abducted under general anesthesia. The bed was adjusted to create a reverse Trendelenburg position for the patient. The operator stood between the patient's legs. The scopist was positioned on the left side of the patient (Fig. 1b).
A commercial four-lumen single-port trocar (Gloveport®; Nelis, Bucheon, Korea) was inserted through a transumbilical incision using Hasson's method. 21 The Gloveport trocar system consists of a self-retractor that covers a 25-mm incision and four channels (one 12-mm channel and three 5-mm channels). A flexible scope was inserted through a channel of this umbilical port after a pneumoperitoneum was created using carbon dioxide at a pressure of 15 mmHg. After flexible scope insertion, two instruments were inserted through the other channels of single-port trocar.
Common surgical procedures
The falciform ligament and the left lobe of the liver were raised toward the cephalad direction by combined suture retraction. 22
Lymphadenectomy for curative distal gastrectomy was accomplished based on the criteria of the Japanese Gastric Cancer Treatment Guidelines 2010 (ver. 3). 23 We performed D1+ or D2 lymphadenectomy using only LigaSure Maryland Jaw 37 cm Laparoscopic Instrument (Medtronics).
After completion of lymphadenectomy, Billroth I or II anastomosis was performed for recovery of gastrointestinal continuity. In cases of Billroth II anastomosis, Braun anastomosis was also performed to reduce bile reflux to the remnant stomach. All the anastomoses were performed with laparoscopic linear staplers (ECHELON FLEX™ Powered ENDOPATH® Stapler; Ethicon Endo-Surgery, Inc., Cincinnati, OH).
Data collection
Demographic data, including age, sex, body mass index (BMI), and ASA score, were collected from all enrolled patients. In addition, clinical outcomes, including the operation time, LND time, conversion to open or conventional laparoscopic surgery, reconstruction method, postoperative hospital stay, time to the first semiblend diet, and postoperative complications, were also investigated. LND time was defined as the time between the first incision of omentectomy and last dissection of lymph node station No.1. Postoperative complications were classified based on the Clavien-Dindo classification of surgical complications. 24
We also investigated pathologic results, including tumor depth, and number of retrieved and metastatic lymph nodes.
Comparison of clinicopathologic outcomes to internal controls
Internal control was defined as a patient who underwent RPLG for early gastric cancer, but not enrolled in the current trial. LND was performed with Harmonic® Scalpel (Ethicon Endo-Surgery, Inc., Cincinnati, OH) for the internal control. As supplement analysis, the clinicopathologic outcomes were compared between the study participants and internal controls.
Results
Actual enrollment started in May 2015. The accrual was terminated in November 2016 when the target number of patients had been enrolled. Therefore, a total of 20 patients were enrolled in this study from May 2015 to November 2016.
Patient demographics
Patient demographics are shown in Table 1. The mean age of enrolled patients was 58.8 ± 12.3 (40–81), and the mean BMI was 23.1 ± 3.6 (17.1–29.7) kg/m2.
BMI, body mass index; ASA score, score graded by the American Society of Anesthesiologists physical status classification; SPDG, single-port laparoscopic distal gastrectomy; TPDG, three-port laparoscopic distal gastrectomy; ESD, endoscopic submucosal dissection.
Clinicopathologic outcomes
Of the 20 patients enrolled in this study, 11 (55.0%) and 9 (45.0%) underwent single- and three-port laparoscopic surgeries, respectively. All enrolled patients were not involved in conversion to open surgery or conventional multiport laparoscopic surgery, but a patient underwent conversion to total gastrectomy to acquire an adequate resection margin (Table 2). D1+ or D2 LND was completed in every patient who underwent three- (Fig. 2) or single-port laparoscopic distal gastrectomy (Fig. 3).

Lymph node dissection in three-port laparoscopic distal gastrectomy.

Lymph node dissection in single-port laparoscopic distal gastrectomy.
This patient underwent the conversion to total gastrectomy to acquire the adequate proximal resection margin.
LND, lymph node dissection; SBD, semiblend diet; C-D grade, grade by the Clavien-Dindo classification of surgical complications; RLN, number of retrieved lymph nodes; MLN, number of metastatic lymph nodes; SPDG, single-port laparoscopic distal gastrectomy; BII, Billroth II anastomosis; TPDG, three-port laparoscopic distal gastrectomy; BI, Billroth I anastomosis; TPTG, three-port laparoscopic total gastrectomy; EJ, esophagojejunostomy.
The mean operation time was 262.6 ± 36.6 (200–340) minutes, and the mean LND time was 124.7 ± 19.2 (93–171) minutes. The mean hospital stay was 15.2 ± 10.2 (8–44) days, and the mean time to the first semiblend diet was 6.4 ± 12 (4–9) days.
There were three morbidity cases. Of these, only one case corresponded to the Clavien-Dindo grade greater than II (Table 2). One was postoperatively relapsed pneumonia (Clavien-Dindo grade II) that had already affected the patient in the preoperative period, and another was intra-abdominal fluid collection (Clavien-Dindo grade IIIa). The other was postoperative ileus (Clavien-Dindo grade II) in a patient who had undergone intra-abdominal surgery twice. All these patients recovered by conservative treatment, and their clinical courses did not reach mortality.
The mean number of retrieved lymph nodes was 46.8 ± 22.8 (15–105) based on the final pathologic reports of enrolled patients. As shown in Table 3, the mean number of retrieved lymph nodes did not differ between study participants and internal controls (P = .291).
LND, lymph node dissection; C-D grade, grade by the Clavien-Dindo classification of surgical complications.
Discussion
The feasibility of LND has been an important concern regarding RPLG for gastric cancer. 25 This issue is strongly associated with the maintenance of the surgical plane. In three- or single-port laparoscopic surgery, the operator cannot be aided by any assistant who performs countertraction or removes hindrances in the surgical field. Therefore, it is difficult to restore the spatial orientation in the laparoscopic view when blood or opaque fluid covers the surgical field. In other words, even minimal bleeding may affect LND quality and may lead to a critical accident. This is a possible reason for only few surgeons adopting single-port laparoscopic gastrectomy, especially since it is more challenging to control unexpected bleeding with straight instruments inserted through only one trocar.
For these reasons, BVSD has received attention from some surgeons who have attempted RPLG for gastric cancer. This instrument enables the operator to secure hemostasis during RPLG, since the strong vessel-sealing power of BVSD facilitates clipless vessel control in the unaided condition. Although BVSD does not always control the injury of vessels, its strong vessel-sealing potential contributes to maintaining a clean surgical view during RPLG. This feature has also attracted surgeons who prefer conventional laparoscopic surgery for gastric cancer, since a clean surgical view is a basic precondition for consistent LND quality. Actually, in a considerable number of institutes, BVSD has been also added as a routine device for conventional laparoscopic gastrectomy.
Nevertheless, most surgeons prefer the ultrasonic energy device in LND for gastric cancer, although BVSD is often used as an additional device. The blades of the ultrasonic energy device are thinner and sharper than those of the BVSD. Surgeons can create spaces between tissues using the tip of the ultrasonic instrument; less dependence on the dissecting instrument shorten the operation time. In addition, the fast activation time of the ultrasonic energy device is another reason why the operation time can be shortened.
Moreover, “cavitation,” a unique mechanism of the ultrasonic energy device, makes it easy to perform laparoscopic surgery for gastric cancer. 5 Once the tissue is dissected by the cavitation effect, surgeons can obtain the important visual information regarding the tissue structures. These clues are deeply related to creating a surgical dissection plane during laparoscopic surgery.
All these advantages of the ultrasonic instrument become more prominent in RPLG for gastric cancer. During RPLG, the operator's dependence on the cavitation effect may be stronger than during conventional laparoscopic surgery because there is no countertraction or manipulation to help the operator surgeon maintain the spatial orientation. Such a tendency is more obvious in single-port laparoscopic gastrectomy, as the laparoscopic view is considerably different from multiport laparoscopic surgery.
A recently issued BVSD, LigaSure Maryland Jaw 37 cm Laparoscopic Instrument, has shown some potential to change the paradigm described above. This Maryland jaw type LVSS has a fine and curved tip resembling the jaw of the Maryland dissector, which can be applied in tissue dissection. Some surgeons have attempted tissue dissection with this product. Thus, considering the previous experiences with RPLG for gastric cancer, we hypothesized that Maryland jaw type LVSS could be advantageous in LND. A representative rationale for this hypothesis was correlated with the known characteristics of BVSD. As already mentioned, the strong vessel-sealing power of BVSD is advantageous in RPLG. In addition, Maryland jaw type LVSS was produced to be applicable in tissue dissection. Therefore, we applied the Maryland jaw type LVSS in 20 cases of RPLG for gastric cancer. No previous study has examined the clinical effectiveness of BVSD during RPLG, although Kim et al. 26 compared the clinical outcomes between BVSD and the ultrasonic device during conventional laparoscopic gastrectomy. To our knowledge, this is the first prospective study to evaluate the safety and feasibility of applying BVSD in RPLG for gastric cancer.
In this study, although three postoperative complications were noted, we could not find any correlation between these morbidities and the LND procedure. In addition, the mean number of retrieved lymph nodes did not differ from that of internal controls in which the ultrasonic energy device was used for LND (Table 3).
Moreover, we also found several advantages of LND using BVSD during our study. In the next phase of the study, the following features can be considered.
First, as we hypothesized at the initiation of this study, BVSD contributes to keeping the surgical field clean during LND. In fact, there is no evidence that BVSD is more effective than ultrasonic device in LND, since each energy device has its advantages and disadvantages. Although the ultrasonic device provides limited vessel sealing, vascular clipping makes a secure control of vessel that cannot be sealed by energy device. However, it may be technically demanding to apply clips on vessels during RPLG. In particular, during single-port laparoscopic surgery, vascular clipping is obscured by instrument collision, as well as unaided condition. Therefore, most surgeons depend on energy device rather than vascular clipping during RPLG. Despite efforts to preserve the surgical field during RPLG, such a tendency carries the risk of vessel-sealing failure. In our trial, LND using BVSD minimized the frequency of vessel-sealing failure because it provided a more stable vessel sealing than the ultrasonic device. Moreover, although vessel-sealing failure occurred, we could control bleeding or oozing without adding any port. Consecutively, during 20 RPLGs for gastric cancer, we feasibly performed LND without any disorientation of the surgical plane.
Another benefit is related to the activation mechanism of BVSD. Because the ultrasonic device generates energy by vibrating its active blade, 5 droplets of tissue fluid often stain the lens of laparoscope. Although an air suction system can be connected to the assistant's working port to reduce this phenomenon, such a system does not work in RPLG. The droplets block the operator's view, as the air flows toward the operator's working port. This situation considerably disturbs the operator during laparoscopic surgery, since the continuity of the surgical process is disconnected when the scopist cleans the stained lens of laparoscope. However, unlike the ultrasonic device, BVSD does not cause turbulent flow of droplets, and therefore, the laparoscope is less stained. Kim et al. 26 also suggested that BVSD provided a clear laparoscopic view. This feature may also save time in single-port laparoscopic surgery where it is bothersome to rearrange the scope and instruments in the laparoscopic view.
Despite the aforementioned potential advantages, RPLG using only BVSD is associated with several limitations. Most of all, although we suggest that LND using BVSD provides some advantages in RPLG for gastric cancer, there is a precondition to our contemplation: overcoming the learning curve for conventional laparoscopic gastrectomy. Otherwise, it is dangerous to perform LND during three- or single-port laparoscopic surgery because expertise in laparoscopic anatomy is essential in making a dissection plane without assistance. Particularly, in single-port laparoscopic gastrectomy, it is challenging for a novice surgeon to perform omentectomy using only BVSD, because laparoscopic view is somewhat different from that in multiport laparoscopic surgery. In such circumstances, finding a correct dissection plane without “cavitation” effect depends on the operator's proficiency.
Furthermore, the most unfavorable feature of BVSD in LND for gastric cancer was lateral thermal damage. To achieve sufficient LND, surgeons often activate the energy device in a close vicinity to a major vessel. For instance, the clearance of lymph node No. 8a involves the activation of the energy device near the common hepatic artery, which should be preserved during LND. Such situations are a concern, but are inevitable. This is why most surgeons do not prefer BVSD in LND, since the strong vessel-sealing power of BVSD might cause lateral thermal damage on the surrounding structures. 7 To solve this concern, we devised a new technique to reduce lateral thermal damage. Generally, there is a preset activation time in BVSD, and therefore, the system makes an alarming sound to inform the operator of the end of activation. Our new technique involved stopping the activation before this sound is heard. Although the end of activation means enough activation to seal vessels up to 7 mm in diameter, 7 such strong energy can damage a surrounding structure to be conserved. According to Sutton et al., the temperature generated at the tip of energy devices varies with the activation time. 27 Therefore, we attempted partial activation to prevent unnecessary lateral thermal damage due to BVSD. This technique was named the “short-time activation technique,” which may also shorten LND time by reducing the activation time of BVSD.
In conclusion, a novice surgeon, who had just overcome the learning curve of laparoscopic gastrectomy, 28 feasibly performed 20 RPLGs for gastric cancer by applying a Maryland jaw type BVSD in LND. Although it is still necessary to make more evident data regarding this issue, our attempt may be a solution for the challenging features of three- or single-port laparoscopic surgery. Therefore, in the next phase of our study, we will objectively evaluate the potential advantages of BVSD in RPLG for gastric cancer.
Footnotes
Disclosure Statement
No competing financial interests exist.