
Abstract
Abstract
In recent years, a number of endoluminal procedures such as endoscopic resection and thermal ablation have emerged as less invasive treatment options for early esophageal cancer. These therapies have demonstrated excellent oncologic outcomes for dysplasia as well as intramucosal cancers. However, few studies have directly compared long-term outcomes of endoscopic therapy versus traditional esophagectomy. Current esophagectomy techniques now deliver consistently good outcomes in the hands of experienced surgeons at high volume centers, and this option should be considered an important treatment consideration for early esophageal cancer. Under current recommendations, esophagectomy should be considered for tumors invading the submucosa, tumors with high-risk pathologic features, bulky tumors, multinodular tumors, tumors within a long segment of Barrett's esophagus, and tumors adjacent to a hiatal hernia. Likewise, individual patient factors and comorbidities must also be considered when determining the best treatment for a patient with early esophageal cancer. The risk of missing metastatic disease or recurrence that is associated with endoscopic treatment must be weighed against the surgical risks of esophagectomy. With these considerations in mind, the aim of this article is to review the current guidelines and literature that explore the role of esophagectomy for early esophageal malignancy in the era of endoscopic therapies.
Introduction
E
Staging and Guidelines
At the present time, esophageal cancer is staged using the T (tumor), N (node), and M (metastatic disease) staging classification system as described by the American Joint Committee on Cancer (AJCC) 7th Edition (2010). 2 Early esophageal cancer is defined as any node-negative tumor that does not extend beyond the submucosal layer of the esophageal wall. This correlates with a stage of T1 or less. Early tumors can be further broken down into high-grade dysplasia (Tis), intramucosal cancer (T1a), and submucosal cancer (T1b). 2 The Japanese society for esophageal disease classification 3 further subclassifies tumors based on the depth of invasion into the lamina propria (T1a-lp), muscularis mucosa (T1a-mm), and submucosa (T1b-sm1-3). 3 These classifications are represented in Figure 1 as part of the larger classification system.

Current representation of the subclassification of early esophageal lesions based on depth of invasion into the esophageal wall. HGD, high-grade dysplasia; IMC, intramucosal cancer; SMC, submucosal cancer; Tis, does not invade the lamina propria; T1a-lp, invades the lamina propria; T1a-mm, invades the muscularis mucosa; T1b-sm1, invades the upper third of the submucosal layer; T1b-sm2, invades the middle third of the submucosal layer; T1b-sm3, invades the lower third of the submucosal layer; T2, invades the muscularis propria; T3, invades the adventitia; T4, invades surrounding structures.
The current National Comprehensive Cancer Network (NCCN) guidelines (Version 3, 2015) 4 recommend endoscopic resection (ER) for medically fit patients with HGD (Tis) and intramucosal (T1a) cancer without nodal disease. However, the guidelines begin to lose granularity when tumors are classified as superficial submucosal tumors (T1b-sm1), but they do state that endoscopic therapies are a consideration for these malignancies. 4 If we accept these NCCN recommendations as a baseline for treating these early tumors, then there are a number of additional tumor characteristics that preclude ER and warrant consideration for esophagectomy. These characteristics include tumor size greater than 2 cm, presence of lymphovascular invasion, and poorly differentiated pathology. 4 The NCCN guidelines also acknowledge that esophagectomy remains an acceptable treatment for HGD and intramucosal lesions. 4 Even with this guidance, determining the optimal treatment for early esophageal cancer is often more problematic and demands a contemporary consideration of the current literature.
Outcomes for Surgical and Endoscopic Management of Early-Stage Esophageal Cancer
Although esophagectomy remains an acceptable treatment for early esophageal cancer, it is still associated with significant complication rates and carries the highest mortality among elective gastrointestinal surgical interventions. 5 Improvements in technique and patient care have had a favorable impact on surgical outcomes in recent years, and a number of studies have shown that esophagectomies performed at high volume centers have significantly improved outcomes.6,7 Furthermore, advances in minimally invasive techniques have demonstrated improvement in perioperative and postoperative outcomes in a wide number of areas such as pulmonary complications, length of hospital stay, and postoperative quality of life.8–12
Unfortunately, there are only a few published studies that directly compare long-term outcomes of esophagectomy to those of endoscopic treatments. A recent meta-analysis did identify seven retrospective studies comparing outcomes between endoscopic therapies and esophagectomy.13–20 This analysis included studies that only compared treatments for HGD or intramucosal cancers. The authors found no differences between surgical and endoscopic therapy with respect to cancer remission rates, overall survival, or cancer-related mortality. 13 Not surprisingly, endoscopic treatment was associated with a higher recurrence risk, but fewer major adverse events. 13 A summary of the major outcomes from this pooled analysis is shown in Table 1.
Endoscopic therapy was associated with fewer major adverse events (relative risk 0.38, 95% confidence interval: 0.20–0.73, P = .004). 13
Endoscopic therapy was associated with higher neoplasia recurrence risk (relative risk 9.5, 95% confidence interval: 3.26–27.75, P < .0001). 13
To date, no study has directly compared quality-of-life indices after esophagectomy with those after endoscopic therapy. It is not difficult to appreciate that quality of life is more adversely impacted by a major operation, but one potential advantage to surgical resection is that esophagectomy requires much less frequent follow-up screening endoscopy. Follow-up regimens for ER may require between two to six endoscopies in the first year and then yearly afterward, even in the absence of new lesions.5,21 Patients often require several ablative treatments to eradicate residual dysplasia and metaplasia and as many as 50% will develop a symptomatic stricture that requires endoscopic dilation.5,22 Although prospective data are lacking, ER appears to have similar long-term survival outcomes with lower complication rates compared to esophagectomy. Combined modality treatment of ER with radiofrequency ablation has also demonstrated excellent oncologic metrics. 5 Even with improvements in surgical outcomes, endoscopic therapy is preferred for HGD and intramucosal lesions in medically fit patients due to the less invasive nature of ER.
Discussion
With the adoption of routine surveillance for Barrett's esophagus, as many as a third of all esophageal cancers are diagnosed as early-stage malignancies. 23 This has facilitated an expanded role for endoscopic techniques in providing definitive treatments. At this time, endoscopic therapies not only play an important role in treatment but also in the staging of early esophageal cancers.5,24 A recent retrospective review of 107 early esophageal cancer patients treated with esophagectomy found that endoscopic ultrasound (EUS) understaged tumor depth in 32% (19/59) of pathology-confirmed T1a tumors and 49% (17/35) of T1b tumors. 25 Due to the inaccuracies of EUS, a more expanded use of ER as a staging modality is gaining popularity with many clinicians. Consequently, staging ER can now be used to guide individualized treatment or as a definitive therapy if an R0 resection is obtained on the index procedure. Positive radial margins following staging ER can be managed with repeat ER, while a positive deep margin should usually be treated surgically. 5
Due to the aggressive nature of this malignancy, any evidence of submucosal invasion should be treated with esophagectomy. 5 It is well recognized that there is a definite increased risk of lymph node metastasis once the tumor invades into the submucosal plane, and this observation forms the basis for the current surgical recommendations. 26 The risk of lymph node metastasis for intramucosal lesions can be as high as 8%, but once tumor reaches the submucosa, the risk is much greater.26,27 In the largest analysis to date, a European group pooled outcomes from 7645 esophagectomies and found lymph node metastasis in 27%, 38%, and 54% for submucosal tumors staged at sm1 through sm3, respectively. 27 Interestingly, as a whole, submucosal squamous cell tumors demonstrated a more aggressive behavior with 45% nodal metastasis compared to 26% of adenocarcinomas. 27 Due to this observation, some clinicians have gone so far as to argue that the aggressive nature of squamous cell cancer mandates that even intramucosal tumors (T1a-mm) should be treated with esophagectomy as opposed to endoscopic therapy. 23 Other factors that predict lymph node spread include lymphovascular or neural invasion, poor differentiation, and the presence of multifocal HGD. 26 Tumors displaying these pathologic findings should be considered for esophagectomy regardless of T-stage. 26 Finally, when a malignancy is contained within a long segment of Barrett's esophagus, consideration should be given to esophagectomy. Long-segment metaplasia exists as a potential source of a metachronous malignancy and significantly complicates postprocedural surveillance. 28
In addition to microscopic features, gross tumor characteristics, individual patient anatomy, and functional status must also be taken into account when determining the best possible treatment. The NCCN guidelines set a size limit of 2 cm for endoscopic therapy. 4 This size determination is largely based on the finding that tumors greater than 2 cm are more likely to require piecemeal resection. Absolute size aside, it is more important to consider if the tumor can be resected en bloc. 29 A recent large systematic review examined outcomes of over 4000 patients from 80 studies undergoing treatment for early esophageal cancer and found that piecemeal ER was an independent predictor of local recurrence. 29 Additional anatomic considerations that may cause difficulty with en bloc resection are multinodularity, ulceration, hiatal hernia, and prior fundoplication. 26
Finally, when treating early esophageal cancer with esophagectomy, it is important to tailor the surgical technique in a manner that will minimize operative complications. At our institution, we prefer to perform a minimally invasive transhiatal esophagectomy for early esophageal cancer. This approach has shown consistent improvements in both short-term and long-term outcomes.8–12 In addition, the benefits of an extensive mediastinal lymphadenectomy are unproven for early cancers, and this also favors the transhiatal approach. This procedure does not require single-lung ventilation, patient repositioning, thoracoscopy, or an intrathoracic anastomosis.11,30 The laparoscopic transhiatal inversion technique utilized in our practice is a modification of the open inversion stripping technique originally described by Akiyama in 1994. 30 For tumors of the GE junction, we prefer an antegrade inversion technique, as opposed to a retrograde technique (Fig. 2). Inverting the esophagus in an antegrade manner does not require division of the stomach along the lesser curvature, and this leaves the tumor margin intact. 30 In addition, an antegrade inversion does not require a large gastrotomy as with the retrograde technique. This minimizes exposure of the peritoneum to contamination from gastrointestinal flora, as well as potential exposure to malignant cells. 30 For patients who are not candidates for endoscopic treatment, esophagectomy can be a tolerable and safe option when performed by experienced hands. In our experience, laparoscopic transhiatal esophagectomy can be performed with low morbidity and a perioperative mortality rate <1%. 31
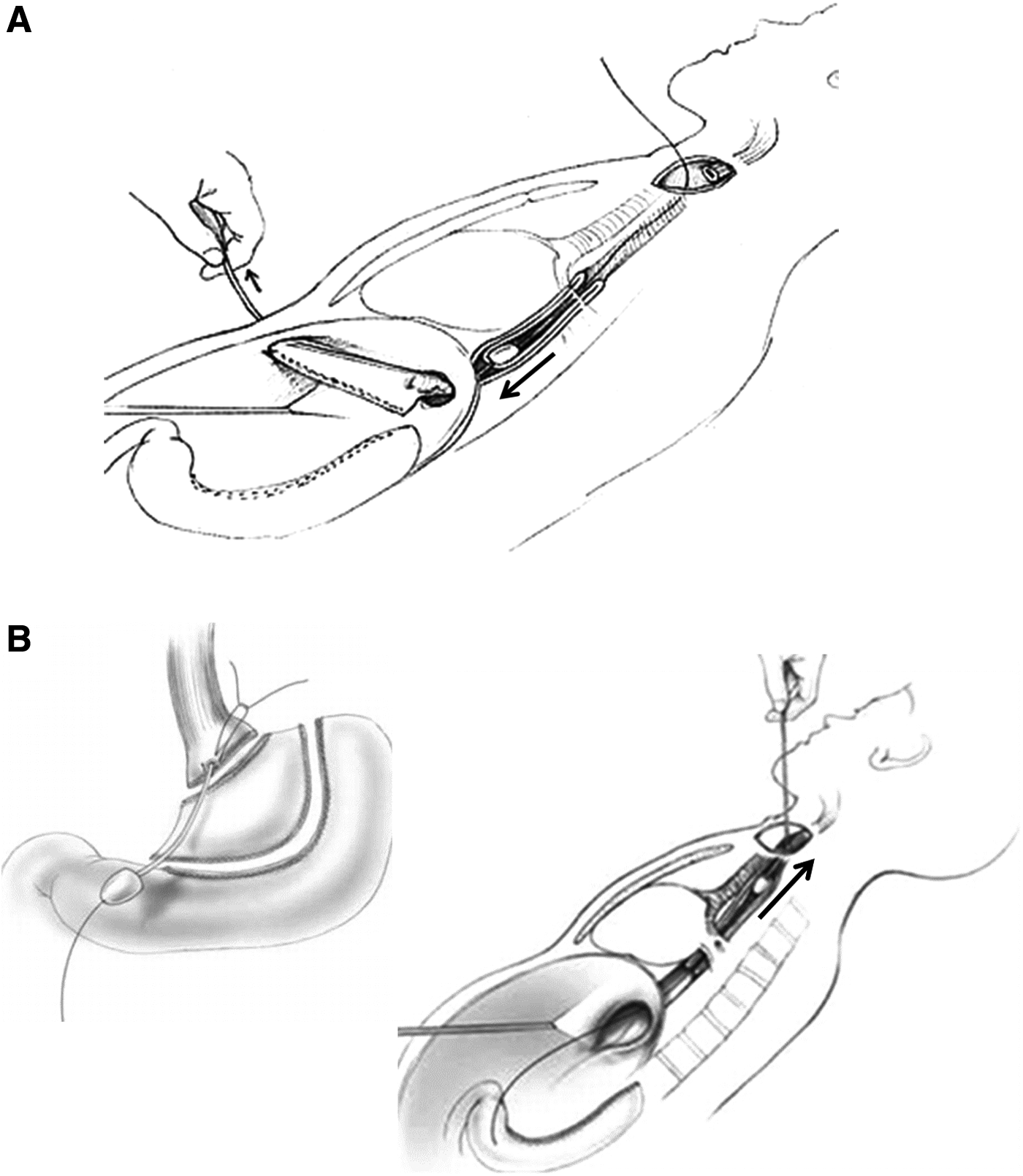
For an antegrade inversion esophagectomy
Conclusions
The emergence of endoscopic treatments provides clinicians with less invasive options for esophageal cancers, yet there are many circumstances where esophagectomy remains an important consideration. A summary of our treatment pathway for early esophageal cancer is outlined in Figure 3. We recommend that patients with intramucosal tumors (T1a) and HGD be first considered for ER, in line with the NCCN guidelines. Following ER, if a radial margin is positive, the patient can be treated with repeat ER or ablations. If the deep margin is positive on initial ER, the patient should be referred for esophagectomy. If tumor pathology demonstrates lymphovascular invasion or poorly differentiated pathology, regardless of T-stage, the patient should also be treated with esophagectomy. Likewise, tumors larger than 2 cm, those located within a long segment of Barrett's esophagus, a hiatal hernia, a fundoplication, or other anatomic variation making endoscopic en bloc resection difficult, should also be referred for surgery. Patients treated with ER must be able to comply with regular follow-up surveillance due to the high recurrence risk and stricture rates that often require reintervention. For early esophageal cancer, we favor a minimally invasive transhiatal technique due to the decreased pulmonary morbidity compared to a transthoracic approach. Finally, both esophagectomy and endoscopic treatments should be performed in high-volume centers to maximize patient outcomes.
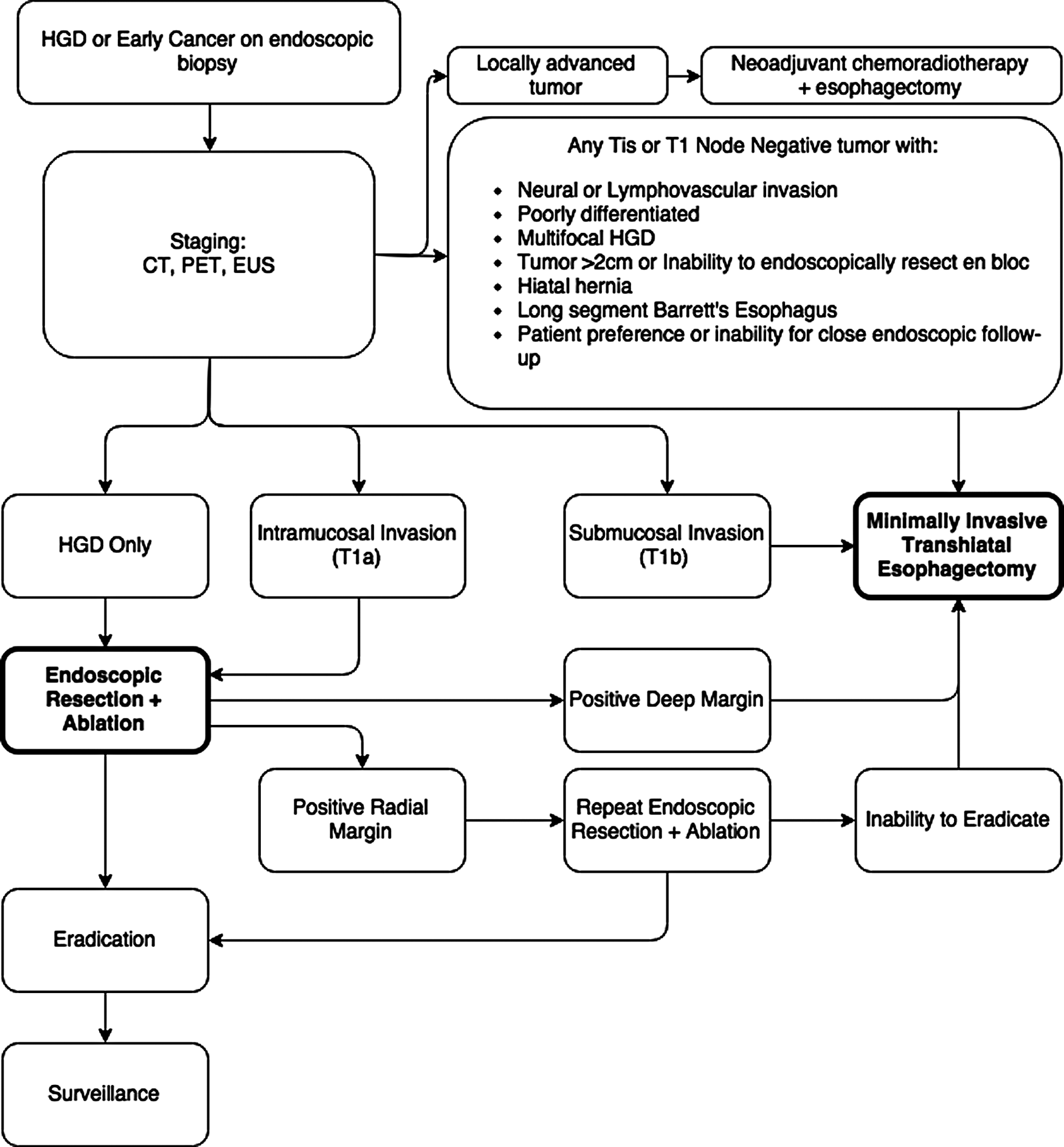
Our current institutional treatment pathway for determining the best management of early esophageal cancer and high-grade dysplasia.
Footnotes
Disclosure Statement
No competing financial interests exist.