
Abstract
Abstract
The last 25 years have witnessed a steady increase in the use of minimally invasive esophagectomy for the treatment of esophageal cancer. However, it is unclear which the optimal minimally invasive approach is: totally minimally invasive or hybrid (laparoscopic assisted or thoracoscopic assisted)? The current evidence from nonrandomized control trials suggests that hybrid laparoscopic-assisted esophagectomy couples the benefits of laparoscopy and the advantages of thoracotomy, leading to reduced surgical trauma without jeopardizing survival compared with open esophagectomy. Compromised blood supply and tension on the anastomosis are two of the main factors that lead to anastomotic leakage. Recent studies have shown that a side-to-side mechanical intrathoracic esophagogastric anastomosis is associated with low anastomotic complications. This article discusses surgical aspects and outcomes of hybrid laparoscopic-assisted esophagectomy for esophageal cancer.
Introduction
E
The optimal approach to esophageal cancer is still under debate. While transhiatal esophagectomy is advocated for the reduced postoperative cardiopulmonary complication rates,2,3 transthoracic (Ivor Lewis) esophagectomy is considered in many centers the preferred approach since it is associated with lower esophagogastric anastomotic leak rates 4 and a more extended mediastinal lymphadenectomy. 5 Furthermore, mortality rates do not differ in patients developing cervical or intrathoracic anastomotic leak after esophageal resection performed in high volume centers.5,6
The last 25 years have witnessed a steady increase in the implementation of minimally invasive approaches to esophageal cancer. Evidence from nonrandomized controlled trials (non-RCTs) and small randomized controlled trials (RCTs) shows lower cardiopulmonary morbidity and in-hospital mortality and shorter hospital stay after laparoscopic/thoracoscopic than after open Ivor Lewis esophagectomy.7,8 More recently, a hybrid transthoracic approach (laparoscopy + right thoracotomy) has been proposed, aiming to combine the reduced risk of anastomotic leak of the transthoracic approach and the lower morbidity of laparoscopy.
The aims of this article are to describe the technical steps of a transthoracic hybrid esophagectomy and to discuss the outcomes of this approach.
Surgical Technique
Step #1: Patient positioning on the operating table and trocar placement
The patient is supine over a bean bag being inflated to prevent sliding during the operation when a steep reverse Trendelenburg position is used. After general anesthesia is induced with a double-lumen endotracheal tube, a nasogastric tube is inserted to keep the stomach decompressed. The surgeon performs most of the laparoscopic procedure standing between the patient's legs, with an assistant on the right side and another one on the left side of the operating table. Pneumoperitoneum is obtained with a pressure of 15 mmHg using a Veress needle placed 16 cm inferior to the xiphoid process, or a Hasson cannula. After insertion of the camera, the abdominal cavity is carefully inspected to rule out the presence of liver metastases, peritoneal carcinomatosis, or ascites. In the absence of metastatic disease, four 11-mm trocars and one 12-mm trocar are placed as reported in Figure 1.
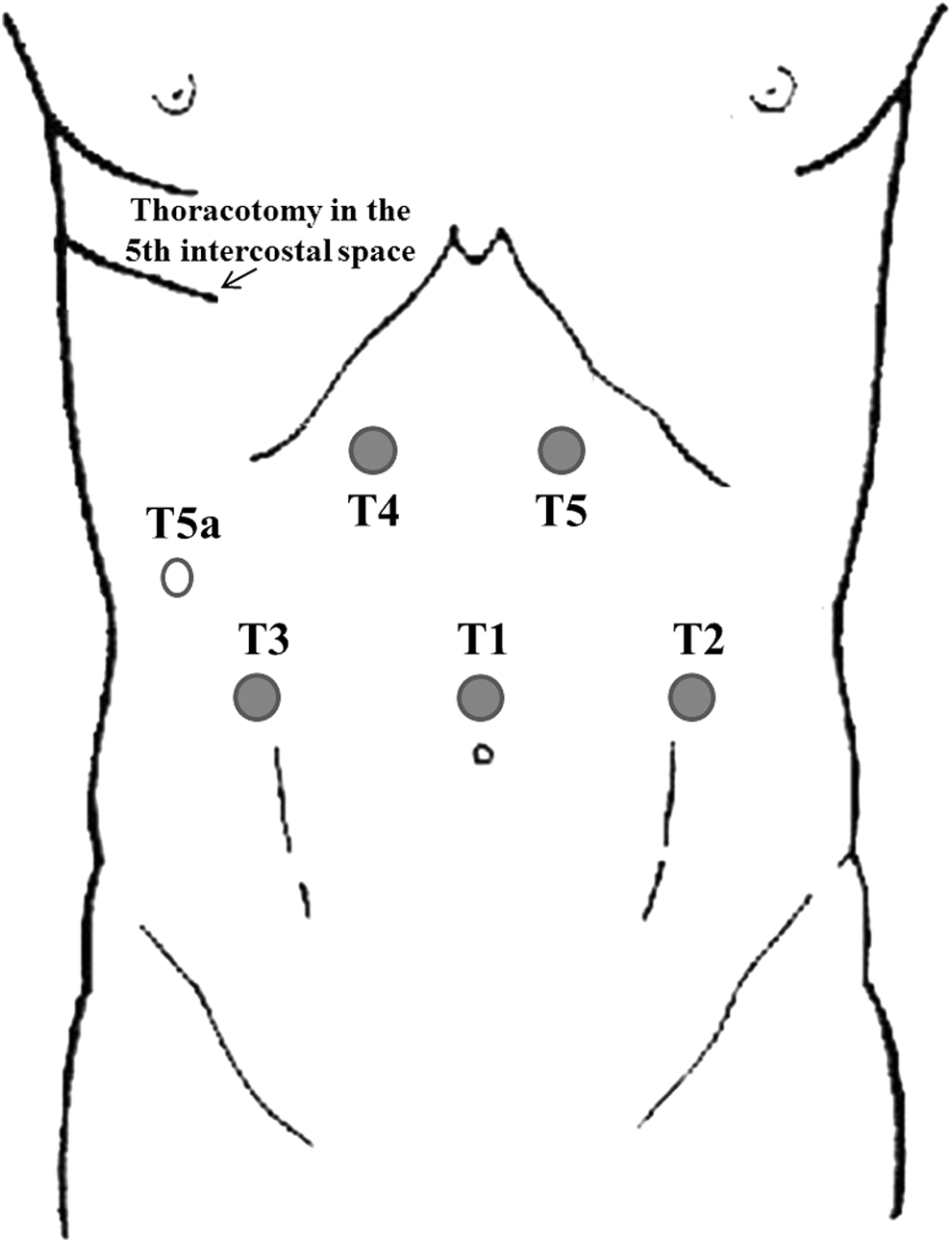
Trocar placement.
Step #2: Crural and lower mediastinal dissection
The gastrohepatic ligament is divided to identify the right pillar of the crus that is bluntly dissected from the right side of the esophagus. Then, the division of the peritoneum and phrenoesophageal membrane covering the esophagus allows to reach the left pillar of the crus, which is separated by blunt dissection from the esophagus. The posterior mediastinum is then dissected cranially for about 5 cm above the diaphragm, assessing the absence of tumor invasion of the aorta, and the lower mediastinal lymph nodes are excised.
Step #3: Short gastric vessel division
The division of the short gastric vessels is performed using an energy-based device starting at the level of the middle portion of the great curvature of the stomach and continuing cranially to reach the most proximal short gastric vessel.
Step #4: Penrose drain placement around the esophagus
A window is created under the esophagus, between the gastric fundus, the esophagus, and the left pillar of the crus, and a Penrose drain is passed around the esophagus.
Step #5: Mobilization of the stomach
Gastric mobilization begins with the dissection of both the coronary vein and left gastric artery at their base aiming to remove as many lymph nodes as possible. Both vessels are then transected using an Endo GIA stapler with a 45 mm long vascular cartridge. The opening of the gastrocolic ligament is then obtained all the way to the pylorus, preserving the right gastroepiploic artery. The gastrohepatic ligament is then completely opened preserving the right gastric artery. As a consequence, the right gastric artery and the right gastroepiploic artery are the two main vessels that supply blood to the stomach.
Step #6: Pyloroplasty
Pyloroplasty is performed by opening the pylorus longitudinally and closing it transversely with interrupted 2-0 silk sutures.
Step #7: Feeding jejunostomy
A jejunostomy is created by: (1) inserting a 10 F feeding tube in the jejunum about 40 cm distal to the ligament of Treitz; (2) placing a 3-0 silk purse string around the tube; (3) creating a 4 cm Witzel tunnel with interrupted 3-0 silk sutures; and (4) fixing the jejunum to the left side of the abdominal wall with four 3-0 silk stitches. Finally, the proper position and patency of the tube are checked by injecting 100 cc of saline.
Step #8: Abdominal wall closure
The trocar sites are closed after removing the trocars under direct vision and achieving hemostasis. Local anesthetics are injected and sterile dressings are applied.
Step #9: Mobilization and resection of the esophagus
After the laparoscopic steps of the operation are completed, the patient is positioned on the left lateral decubitus. The chest is entered through a posterolateral thoracotomy in the fifth intercostal space. Resection of a 1.5-cm long segment of the posterior portion of the sixth rib facilitates the positioning of a retractor to achieve the optimal exposure of the surgical field. After ruling out the presence of metastases, the division of the inferior pulmonary ligament and the opening of the pleura above and below the azygos vein are performed. An Endo GIA linear stapler with a vascular cartridge is used to cut the azygos vein. Then, the dissection of the esophagus is performed beginning about 3 cm above the azygos vein all the way down to the gastroesophageal junction, thus joining the mediastinal dissection previously performed by laparoscopy.
The stomach is pulled up into the chest, a window is opened along the lesser curvature between the second and third branch of the left gastric artery, and transection of the upper portion of the stomach is performed using an Endo GIA stapler with green cartridges. The stomach is not usually tubularized. The esophagus is then clamped with a Satinsky clamp to avoid separation of the mucosa from the muscular layers and transected about 3 cm above the azygos vein.
Step #10: Intrathoracic esophagogastric anastomosis
The esophagus is placed over the anterior wall of the stomach and full thickness, and 3-0 silk stay sutures are placed to keep the posterior wall of the esophagus aligned with the anterior wall of the gastric fundus. Sliding of the esophageal mucosa when the stapler is inserted is avoided by placing 3-0 silk stay sutures at the four edges of the esophageal opening that keep together the mucosa with the other layers of the esophageal wall. The anterior wall of the stomach is opened just distal to the esophageal transection line, and interrupted 3-0 silk stitches are used to fix the gastrotomy to the posterior wall of the esophagus.
After inserting the thinner branch of a 45 mm Endo GIA stapler into the stomach and the thicker branch into the esophagus, the stapler is fired, thus constructing a 4 cm long side-to-side anastomosis between the posterior wall of the esophagus and the anterior wall of the stomach. After passing the nasogastric tube under direct vision into the stomach so that the tip is above the diaphragm, closure of the anterior aspect of the anastomosis is obtained in double layer: an inner layer of running 3-0 absorbable braided suture followed by an outer layer of interrupted 3-0 silk sutures.
Step #11: Drainage and closure
Two chest tubes are routinely placed in the chest for drainage. After direct visual evaluation of the expansion of the lung, the thoracotomy is closed in layers.
Discussion
The last 25 years have witnessed increasing adoption of the minimally invasive surgical approaches for the treatment of esophageal cancer. 9 The current evidence shows better short-term outcomes after minimally invasive than open Ivor Lewis esophagectomy, 7 while long-term oncologic outcomes seem comparable. 10 However, these data should be interpreted with caution since the vast majority of the studies are retrospective. In addition, the heterogeneity of the comparative studies does not allow to define the optimal minimally invasive technique: thoracoscopy + laparoscopy (total minimally invasive), thoracoscopy + laparotomy (hybrid thoracoscopic assisted), or thoracotomy + laparoscopy (hybrid laparoscopic assisted)?
During the past 15 years, disappointing early results of totally minimally invasive esophagectomy in terms of postoperative complications likely secondary to prolonged operative time and controversial oncologic outcomes have led to increasing interests in hybrid techniques.
While only a few studies have evaluated the outcomes in patients undergoing thoracoscopic-assisted Ivor Lewis esophagectomy,11–14 several studies have focused on laparoscopic-assisted esophagectomy15–26 (Table 1). This approach combines the advantages of laparoscopy and thoracotomy. The laparoscopic procedure follows the same oncologic principles of the open surgery with no differences in lymph node harvest,25,26 but it causes a significantly lower surgical trauma; the thoracotomy allows a wide exposure of the chest, is associated with reduced risks of laryngeal nerve injuries, and the construction of the esophagogastric anastomosis appears less challenging than by thoracoscopy.
P < .05.
All cervical anastomoses.
P < .001.
HYB-E, hybrid esophagectomy; Lap., laparoscopic assisted; MPPC, major postoperative pulmonary complications; NA, not available; OP-E, open esophagectomy; PRO, prospective; RETRO, retrospective; VATS, video-assisted thoracic surgery.
Briez et al. 22 published in 2012 the results of a study comparing 140 patients undergoing hybrid transthoracic esophagectomy and 140 well-matched patients undergoing an open Ivor Lewis esophagectomy for cancer. Similar intraoperative complication rates were recorded. Major postoperative pulmonary complications occurred less frequently after hybrid esophagectomy (15.7% versus 42.9%, P < .001); overall morbidity (35.7% versus 59.3%, P < .001) and in-hospital mortality rates (1.4% versus 7.1%, P = .018) were lower after hybrid esophagectomy than open esophagectomy. A multivariate analysis showed that the hybrid approach and epidural analgesia were independent protective factors against pulmonary complications. The authors speculated that the benefits observed in the short term after hybrid esophagectomy might be due to reduction of postoperative pain and related ventilator mechanical dysfunction and by decreased metabolic and inflammatory responses to surgical trauma.
Similar results were reported by Bjelovic et al. 26 in a single institution prospective cohort study where 44 patients undergoing hybrid esophagectomy and 44 patients undergoing open esophagectomy were compared. Bonavina et al. 25 found no significant differences in respiratory complication rates in a propensity-matched comparative analysis of 93 patients having totally minimally invasive esophagectomy and 197 patients undergoing hybrid esophagectomy, confirming the protective role of laparoscopy. Very recently, Scarpa et al. 27 shed some light on the potential mechanisms by which patients undergoing hybrid esophagectomy have fewer complications than those treated by open surgery. They found in a case–control study which included 68 patients that postoperative systemic inflammatory response to surgical trauma was lower and the albumin levels were higher after hybrid esophagectomy than open surgery.
The current evidence shows that totally minimally invasive esophagectomy and hybrid esophagectomy achieve similar long-term oncologic outcomes compared with open surgery. 10 Briez et al. 22 reported similar R0 resection rates (85.7% versus 87.9%) and median number of overall (N = 22) and abdominal resected lymph node (N = 8) after hybrid or open esophagectomy. Median survival was 36 months in both groups, and no differences were observed in 2-year survival: 57.2% versus 58.3%, respectively. In addition, Bjelovic et al. 26 found that the hybrid approach does not jeopardize survival: mean number of harvested lymph nodes was higher after hybrid esophagectomy (31.9 versus 26.3, P = .010) and median overall survival was 778 and 824 days after open or hybrid survival, respectively.
The esophagogastric anastomotic leakage rates largely vary in the literature from 1% to 30%, being higher in patients undergoing transhiatal than transthoracic esophagectomy. 4 Compromised blood supply and tension on the anastomosis are thought to play a major role in causing anastomotic leakage. Historically, a leak in the chest was associated with significantly higher mortality than cervical anastomotic leak 28 ; however, the advances in early diagnosis and treatment of sepsis have led to a significant reduction in leak-related mortality after transthoracic esohagectomy. 4
Other technical factors, including minimally invasive versus open esophagectomy, anterior versus posterior route of reconstruction, and ischemic preconditioning of the gastric conduit or hand-sewn versus stapled esophagogastric anastomosis do not seem to influence the risk of anastomotic dehiscence. 29 A meta-analysis 30 of nine RCTs comparing esophagogastric hand-sewn or stapled anastomosis using a mechanical circular stapler showed that the two techniques are burdened by similar anastomotic leakage rates (8.7% versus 9.2%, respectively), while anastomotic strictures occurred more frequently after stapled anastomosis (pooled odds ratio = 1.76). However, none of these studies have assessed the outcomes of the stapled side-to-side esophagogastric anastomosis that was first proposed in 1998 by Collard et al. with the aim to decrease the risk of anastomotic complications. 31 Some non-RCTs have reported lower or comparable leakage rates and lower stricture rates with this technique than with the hand-sewn anastomosis after transhiatal 32 or transthoracic esophagectomy. 33
Conclusions
The current evidence suggests that hybrid laparoscopic-assisted Ivor Lewis esophagectomy with a side-to-side stapled esophagogastric anastomosis is a safe and effective procedure for the treatment of esophageal cancer. The results of ongoing large RCTs, such as the MIRO trial, 34 will better clarify the real impact of the hybrid approach.
Footnotes
Disclosure Statement
No competing financial interests exist.