
Abstract
Abstract
Gastroesophageal reflux disease affects almost 20% of the population in the United States. Today, proton pump inhibitors are the most frequently prescribed drugs, with an estimated cost of 10 billion dollars per year. Although these medications control heartburn in the majority of patients, other symptoms such as regurgitation and respiratory symptoms often are not controlled, particularly in patients with large hiatal hernias. In these patients a properly performed laparoscopic fundoplication controls esophageal and extraesophageal symptoms and avoids life-long medical therapy. Key elements for the success of a fundoplication are careful patient selection, a complete preoperative evaluation, and a properly executed operation.
Introduction
G
For many years, PPIs were considered safe medications. However, it is becoming clear that they are associated with serious side effects. Several studies show that long-term treatment with PPIs can be associated with Clostridium difficile infection, community-acquired pneumonia, hip fracture, vitamin B12 deficiency, and hypomagnesemia. 3 Their use is also associated with an increased risk of myocardial infarction4,5 and chronic kidney disease. 6 Recently, an association between dementia and use of PPIs has been demonstrated, particularly in elderly patients. 7 Therefore, referrals for laparoscopic fundoplication will likely increase, as gastroenterologists may be more reluctant to prescribe these medications and patients may be more reluctant to undergo a life-long treatment with medications that can cause severe health problems.
This article emphasizes some aspects of the evaluation and surgical treatment of GERD that are thought to play an important role in the success of a laparoscopic fundoplication. The management of a paraesophageal hernia is discussed in another article of this symposium.
Fundoplication for GERD: Tips for Success
Three elements are important for the performance of a successful fundoplication: (1) a comprehensive preoperative work-up, (2) correct indications for the operation, and (3) respect of the key technical elements.
Preoperative work-up
A thorough preoperative GERD work-up identifies (1) the symptoms experienced by the patient, (2) the anatomy of the gastroesophageal junction, (3) the presence of esophageal mucosal damage, (4) the function of the lower esophageal sphincter (LES) and the quality of peristalsis, and (5) the reflux profile, such as the presence of abnormal reflux and the temporal correlation between the symptoms experienced by the patient and the episodes of reflux.
In 2013, a panel of expert gastroenterologists and surgeons published an evidence and experienced-based consensus that recommended the following tests before proceeding with antireflux surgery
8
:
• Symptomatic evaluation: This step should determine the presence of typical/esophageal symptoms (heartburn, regurgitation, and dysphagia) and atypical/extraesophageal symptoms (cough, hoarseness, and enamel erosion). However, a symptomatic evaluation alone should never be considered enough to plan an operation. Many studies report that the presence of symptoms alone, even for typical symptoms such as heartburn, has a low accuracy and leads to a wrong diagnosis of GERD in 30% to 50% of patients.9–11
A good response to PPI is considered an important prognostic factor for the success of a fundoplication,
12
whereas lack of response—usually labeled as “refractory GERD”—should raise the suspicion that the symptoms are caused by a different disease such as achalasia.9,11 If patients present with symptoms suggestive of delayed gastric emptying (DGE) such as nausea, vomiting, or postprandial bloating, a gastric emptying test should be performed. Although gastric symptoms are often secondary to reflux disease, some patients may have true functional disorders because of gastroparesis, especially those with mixed connective tissue disorders or diabetes. If the gastric emptying assessment reveals severe DGE, a concomitant drainage procedure (pyloroplasty) should be considered. • Barium swallow: This radiological study defines the anatomy of the gastroesophageal junction and determines the presence, size, and type of a hiatal hernia. This information helps the surgeon plan the operation, particularly if the endoscopy is performed by another provider. • Upper endoscopy: This test determines the presence and severity of the esophageal mucosal damage. If Barrett's esophagus is identified, this pathology may dictate a different algorithm and require a more rigorous postoperative follow-up. • Esophageal manometry: This physiological test determines the quality of esophageal peristalsis, rules out achalasia, and determines the position of the LES for placement of the catheter for pH monitoring. • Ambulatory pH monitoring: This physiological study is considered the gold standard for the diagnosis of GERD as it establishes the presence of abnormal reflux and determines whether the symptoms are indeed caused by the acid reflux. • Gastric emptying studies and impedance pH should be considered in very few selected patients.
8
Overall, the presence of heartburn, a good response to PPIs, and the presence of pathological reflux as shown by pH monitoring are important predictors of a successful outcome of a fundoplication. 12
Indications for the operation
The operation is indicated in patients who experience complications of PPI therapy or in patients who don't want to take medications for the rest of their lives. In addition, the operation is indicated in patients who do not have complete control of their symptoms, particularly when regurgitation persists and it is associated with cough or episodes of aspiration pneumonia. PPIs, in fact, function by changing the pH of the gastric refluxate but reflux still occurs through an incompetent LES. 13
Caution must be exerted when there is a complete lack of response to PPI therapy, and patients are labeled as having “refractory GERD.” A complete work-up is of paramount importance to ensure that the symptoms are not caused by other esophageal disorders such as achalasia or eosinophilic esophagitis or by other gastrointestinal diseases such as irritable bowel syndrome or cholelithiasis.9–11
Treatment of GERD is challenging in morbid obese patients, particularly when central obesity is present. The pathophysiology of the disease in these patients is different as an increased gradient between the stomach and the esophagus (thoracic–abdominal pressure gradient) is usually present and plays an important role.14,15 A Roux-en-Y gastric bypass is probably the procedure of choice, as it controls both acid reflux (few parietal cells in the small gastric pouch) and bile reflux (long Roux loop). In addition, it promotes weight loss with a reduction of the pressure gradient. The management of GERD in morbid obese patients is discussed in another article of this symposium.
Technical elements
The following steps depict successful approach to a fundoplication (Table 1).
The patient is placed in a steep reverse Trendelenburg position with the legs extended on stirrups. The surgeon stands between the patient's legs. Five trocars are used for the operation (Fig. 1).

Position of trocars for laparoscopic fundoplication.
Step 1. The gastrohepatic ligament is divided to the right pillar of the crus. The pillar is then separated from the esophagus. The peritoneum and the phrenoesophageal membrane overlying the esophagus are transected. The left pillar of the crus is then separated from the esophagus.
Step 2. The short gastric vessels are divided, starting midway along the greater curvature of the stomach toward the left pillar of the crus. If a large hiatal hernia is present, it may be safer to start with this step.
Step 3. The dissection is performed superiorly into the posterior mediastinum to have a minimum of 3 cm of esophagus without tension below the diaphragm. The posterior and anterior vagus nerves are clearly identified and preserved.
Step 4. A window is created between the stomach, the left pillar of the crus, and the esophagus. A Penrose drain is placed around the esophagus, also incorporating the anterior and posterior vagus nerves.
Step 5. The right and left pillar of the crus are approximated using nonabsorbable sutures, placed posterior to the esophagus.
Step 6. A 56F to 60F bougie is passed into the stomach. The use of the bougie decreases the incidence of postoperative dysphagia. 16
Step 7. The stomach is passed behind the esophagus and a shoe-shine maneuver is performed to verify sufficient fundic mobilization and to avoid having part of the gastric fundus above the wrap. A 360° fundoplication is created by placing three stitches of nonabsorbable material at 1 cm intervals to approximate the right and left side of the fundoplication (Fig. 2). The length of the anterior portion of the fundoplication should be ∼2 cm. In patients with very severe abnormalities of peristalsis, a partial fundoplication is the procedure of choice, as it is associated with a lower incidence of postoperative dysphagia17,18 (Fig. 2).
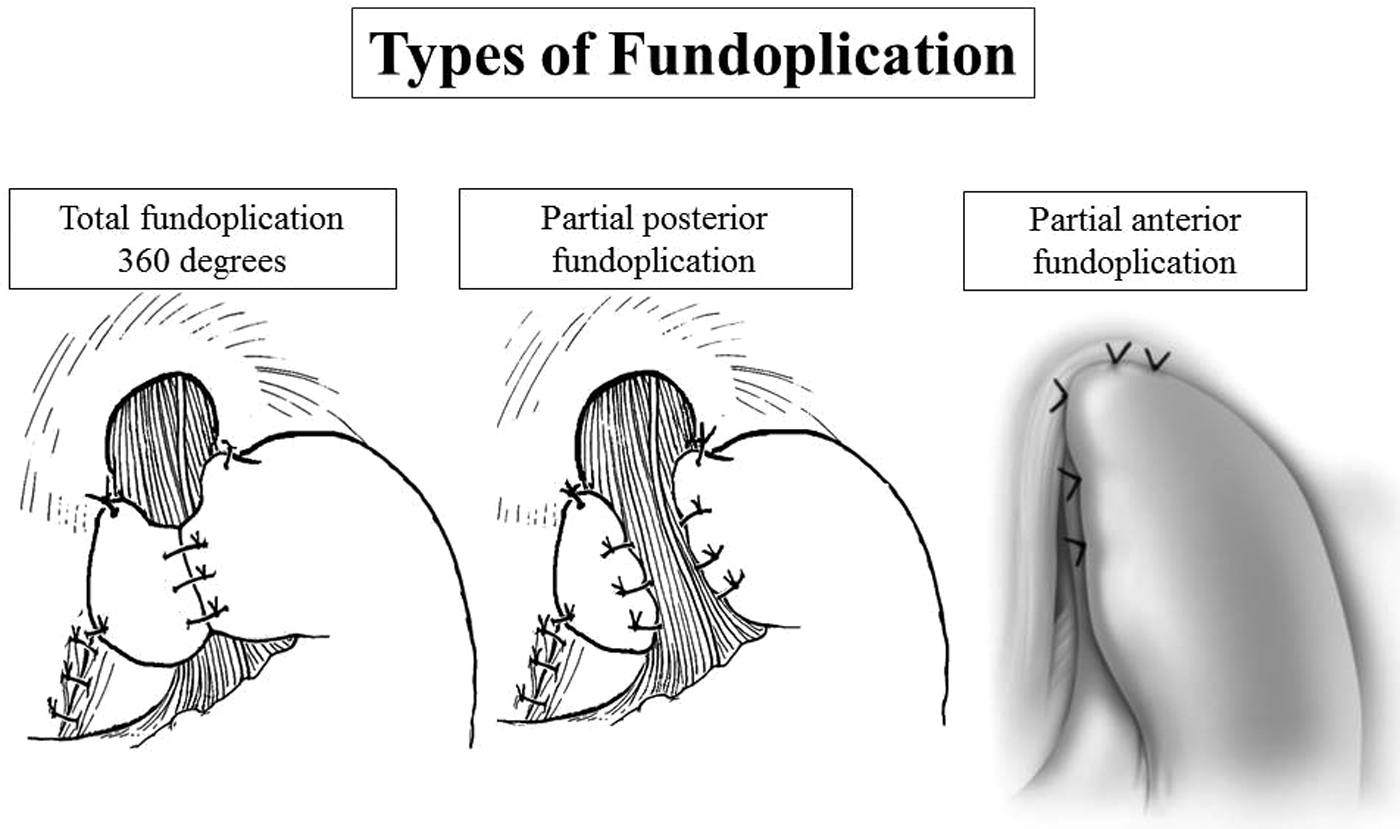
Types of fundoplications.
When these elements are respected, the operation is successful in about 90% of patients. If symptoms recur, a careful work-up must be performed to determine whether pathological reflux is indeed present and to identify the cause of the recurrence19–21 (Table 2). Horgan et al. published an excellent anatomic classification of the failures based on the preoperative work-up and operative findings. 22 As a redo operation is complex and it is usually associated with increased morbidity, a longer hospital stay, and a lower success rate, it is important to identify the patients who need a reoperation. This type of operation requires a detailed discussion about alternatives, benefits, and risks with the patient as the risks may outweigh the benefits.
Side Effects of Laparoscopic Fundoplication
Most patients experience transient gastrointestinal side effects in the postoperative period such as early satiety (96%), hyperflatulence (82%), diarrhea (26%), nausea (15%), and odynophagia (5%). 23 However, persistent bloating and dysphagia cause patient dissatisfaction despite reflux control. 24
The LOTUS trial found that 5 years postoperative bloating was present in 40% of patients after laparoscopic antireflux surgery. 25 Some authors feel that the type of fundoplication may be related to the incidence of bloating. For instance, Broeders et al. reported that the incidence of bloating was significantly higher after a Nissen fundoplication than after a Toupet fundoplication. 26 Another hypothesis is that patients with “upright” reflux have more aerophagic tendencies and, therefore, are more susceptible to develop gas-related problems postoperatively.27,28 However, the subjective definition and evaluation of postoperative gas-related symptoms remained a strong limitation of those studies. In addition, other studies have shown that all three pathological reflux patterns (upright, supine, and bipositional) respond favorably to laparoscopic fundoplication based on subjective and objective criteria.29–31
Although transient dysphagia is common in the initial weeks after fundoplication, long-term dysphagia is rare. As previously reported, the use of a bougie decreases the incidence of postoperative dysphagia. Patterson showed that the incidence of long-term severe postoperative dysphagia was 5% when a bougie was used, but was 14% when it was not used. 16 In addition, transection of the short gastric vessels allows a tension-free fundoplication, with a lower incidence of postoperative dysphagia. 32 Unfortunately, preoperative testing does not identify patients at risk for persistent dysphagia after laparoscopic antireflux surgery. The presence of dysphagia preoperatively is the best predictor of postoperative dysphagia. 33
Conclusions
Laparoscopic fundoplication is an effective and long-lasting treatment for GERD. Its success is based on a careful evaluation and patient selection, and on an operation that respects the key technical elements that have been already identified.
Footnotes
Disclosure Statement
No competing financial interests exist.