
Abstract
Abstract
Purpose:
To investigate the value of laparoscopic radical hysterectomy (LRH) in the treatment of early stage cervical cancer by comparing intraoperative and postoperative outcomes with abdominal radical hysterectomy (ARH).
Materials and Methods:
We searched the Medline, Web of Knowledge, Cochrane Library, and Chinese National Knowledge Infrastructure, through February 2, 2016 with keywords of “laparoscopic OR laparoscopy” AND “radical hysterectomy OR early cervical cancer OR stage IB, stage IB1, stage IB2, stage IIA, stage IIA1, stage IIA2, stage IIA cervical cancer” to identify all relevant studies that compared LRH with ARH in treating early cervical cancer. Two reviewers evaluated the quality of literature independently. Standardized tables were used to extract data (study or participant details and results) from the texts, tables, figures, or any other attachments of eligible publications. Weighted mean differences (MDs) and odds ratios (ORs) were pooled with the random effects model. Then we conducted meta-analysis using the RevMan5.3 software.
Results:
A total of 615 studies were initially identified. After screening, 23 studies, including 4205 patients were recruited. LRH was associated with lower estimated blood loss (mL) (MD = −178.41, 95% confidence interval [CI] = −214.89 to −141.94, P < .00001), longer operation time (minutes) (MD = 43.68, 95% CI = 29.42–57.95, P < .00001), fewer retrieved lymph nodes (MD = −3.44, 95% CI = −5.96 to −0.92, P = .007), shorter hospital stay (day) (MD = −3.17, 95% CI = −4.06 to −2.29, P < .00001), quicker return to normal bowel activity (day) (MD = −0.7, 95% CI = −0.96 to −0.45, P < .00001), and shorter duration of bladder catheterization (day) (MD = −1.69, 95% CI = −2.83 to −0.55, P < .004) than ARH. LRH also demonstrated lower odds of transfusion (OR = 0.47, 95% CI = 0.30–0.73, P = .0007), and ileus (OR = 0.34, 95% CI = 0.12–0.91, P = .03) than ARH.
Conclusion:
LRH outweighs ARH in treating early stage cervical cancer in most essential aspects, which should arouse sufficient attention.
Introduction
D
The progressing technique and effectiveness of minimally invasive surgery in the late 1980s encouraged surgeons to explore its application to complicated oncologic surgery, thus complementing the traditional laparotomy approach to RH. 3 Initially, the laparoscopic approach was only a supplementary means of vaginal RH and was restricted to pelvic lymph node dissection. 4 Gradually, the application of laparoscopic procedures to oncologic surgery excelled with its superiorities in effectiveness, safety, short hospital stay, and less estimated blood loss (EBL). 5 With the improvement of instruments and technique, laparoscopic surgery has demonstrated at least an equivalent effect to traditional hysterectomy in dealing with benign gynecological conditions. 6 In treating endometrial cancer, the laparoscopic approach has reached similar clinical outcomes to laparotomy without lowering survival rate.3,7 Although laparoscopic surgery has the above advantages, its longer operative time (OT) compared with laparotomy postponed the adoption of the laparoscopic approach for malignancies. 7 Currently, laparoscopic radical hysterectomy (LRH) and abdominal radical hysterectomy (ARH) are both available in the clinical setting along with controversial arguments. This systematic review and meta-analysis aim to compare intraoperative and postoperative events between LRH and ARH approaches in treating early stage cervical cancer.
Materials and Methods
Systematic search strategy
We conducted a comprehensive search of the electronic databases, including the Medline, Web of Knowledge (WOK), Cochrane Library and Chinese National Knowledge Infrastructure (CNKI), through February 2, 2016. We used the terms, laparoscopic OR laparoscopy AND radical hysterectomy OR early cervical cancer OR stage IB, stage IB1, stage IB2, stage IIA, stage IIA1, stage IIA2, and stage IIA cervical cancer, to identify all relevant studies that compared LRH with abdominal approaches in treating early cervical cancer. The detailed search strategy for Medline with Medical Subject Heading search terms and free text correlated with this topic can be found in Appendix 1. The search was restricted to “comparative research” using online filtering options. All available studies were considered regardless of their language status. Experts were consulted, and references from relevant articles were scanned. Two independent reviewers performed all aspects, including establishing the search strategy, screening the titles and abstracts of all articles according to inclusion criteria, and then reviewing the full text articles in detail, as indicated. The third reviewer examined and arbitrated any disagreements.
Identification of articles and data extractions
Studies meeting all the following terms were eligible for inclusion: (1) the primary population of interest was women diagnosed with cervical cancer (IA1 to IIA) and treated with RH with or without lymphadenectomy; (2) prospective and retrospective studies comparing laparoscopic surgery with abdominal approaches; (3) measurements involved were intraoperative and postoperative outcomes, which may be the following, but does not necessarily include them all: intraoperative outcomes included EBL (mL) as approximately measured by irrigation–suction fluid difference, blood transfusion, OT (minutes), number of lymph nodes retrieved, and intraoperative complications; postoperative outcomes included length of hospital stay (day), febrile morbidity, deep venous thrombosis/pulmonary embolism (DVT/PE), return to normal bowel activity (day), ileus, lymphocele or lymphedema, duration of bladder catheterization (day), urinary tract infection (UTI), ureteral/vesical/vaginal fistulas, recurrences, concurrent chemoradiotherapy (CCRT), and length of follow-up (month); and (4) for repeated reports of the same sample population, only the most recently published one was included.
The exclusion criteria were: (1) studies evaluating radical trachelectomy for fertility preservation, radical vaginal hysterectomy, abdominal assisted vaginal hysterectomy, recurrent cervical cancer cases, or single-armed studies; (2) publications lacking specific data associated with intra- or postoperative outcomes, which were essential for the analysis; and (3) earlier versions of repeated reports of the same sample population. The sample size was not an exclusion criterion.
Standardized tables were used to extract the required data from all eligible publications, including study details (first author's name, publication year, country, and type of study), participant details (number of patients in respective groups, patient characteristics, histopathology, and surgical intervention), and results (intra- and postoperative events). Data came from texts, tables, figures, or any other attachments. All analyses were based on previously published studies, thus no ethical approval and patient consent were required.
The Newcastle–Ottawa Scale (NOS) was used to assess the quality of the included studies independently by 2 reviewers. 8 The 2 investigators extracted data until agreements were reached through discussion.
Data synthesis and data analysis
The differences in EBL (mL), OT (minutes), length of hospital stay (day), return to normal bowel activity (day), duration of bladder catheterization (day), length of follow-up (month), and number of total or pelvic-only lymph nodes retrieved were analyzed using mean, standard deviation, and sample size for each group. The effect size was expressed as a weighted mean difference (MD) with 95% confidence interval (CI) and two-sided P values. Hozo's formula was used to convert data expressed as a median and range. 9 Dichotomous data were presented as odds ratios (ORs) with 95% CIs. The Mantel–Haenszel estimates were calculated and pooled under a random effects model. Heterogeneity was assessed by examining the clinical characteristics of the included studies as well as by formal statistical testing with χ2 and I2. The Egger test was used to assess the possibility of publication bias by Stata/MP 13.0 (StataCorp, College Station, TX). The meta-analysis was performed with RevMan5.3 according to the PRISMA guidelines. 10
Characteristics of included studies
The systematic search identified 615 relevant references and the study selection flowchart was depicted in Appendix Figure A1. After screening titles and abstracts, we excluded 511 articles, including those evaluating different procedures or disease stages. The 104 remaining articles were retrieved in full text for formal review. After independent review, 81 studies failing to offer specific data of intra- or postoperative outcomes were excluded. We examined recent reviews and comments, and no additional relevant studies were included.
Table 1 displayed the characteristics of the 23 included studies with 4205 participants meeting our predefined inclusion criteria.11–33 Patient characteristics, such as number of participants in each study, were collected. Histological types and interventions were also gathered.
AC, adenocarcinoma; ARH, abdominal radical hysterectomy; ASC, adenosquamous carcinoma; LA, lymphadenectomy; LN, lymph nodes; LRH, laparoscopic radical hysterectomy; RCT, randomized controlled trial; RH, radical hysterectomy; SCC, squamous cell carcinoma.
Among the included studies, only one was the randomized controlled trial while all the others were retrospective or prospective cohort design. Five studies were conducted in the United States,14–16,19,30 five in Italy,13,18,29,32,33 four studies in Korea,20–22,31 two in Turkey,23,24 one in Norway, 17 and six studies in China.11,12,25–28 In all, 4205 women were included in the pooled analysis; 1250 women were treated by LRH and 2955 by ARH. The studies were conducted and published between 2003 and 2016. All women were treated with RH with or without lymphadenectomy; RH could be type II and III under the Piver classification 34 or type B1/C1 according to Querleu and Morrow classification. 35 The assessment of the risks of bias is shown in Table 2. According to the Newcastle-Ottawa Scale (NOS), high quality choices are identified with a star—a maximum of one star for each item within the “Selection” and “Outcome” categories, a maximum of two stars for the “Comparability” category.
Results
Figures 1 and 2, respectively, showed the forest plots of intraoperative and postoperative events between LRH and ARH.
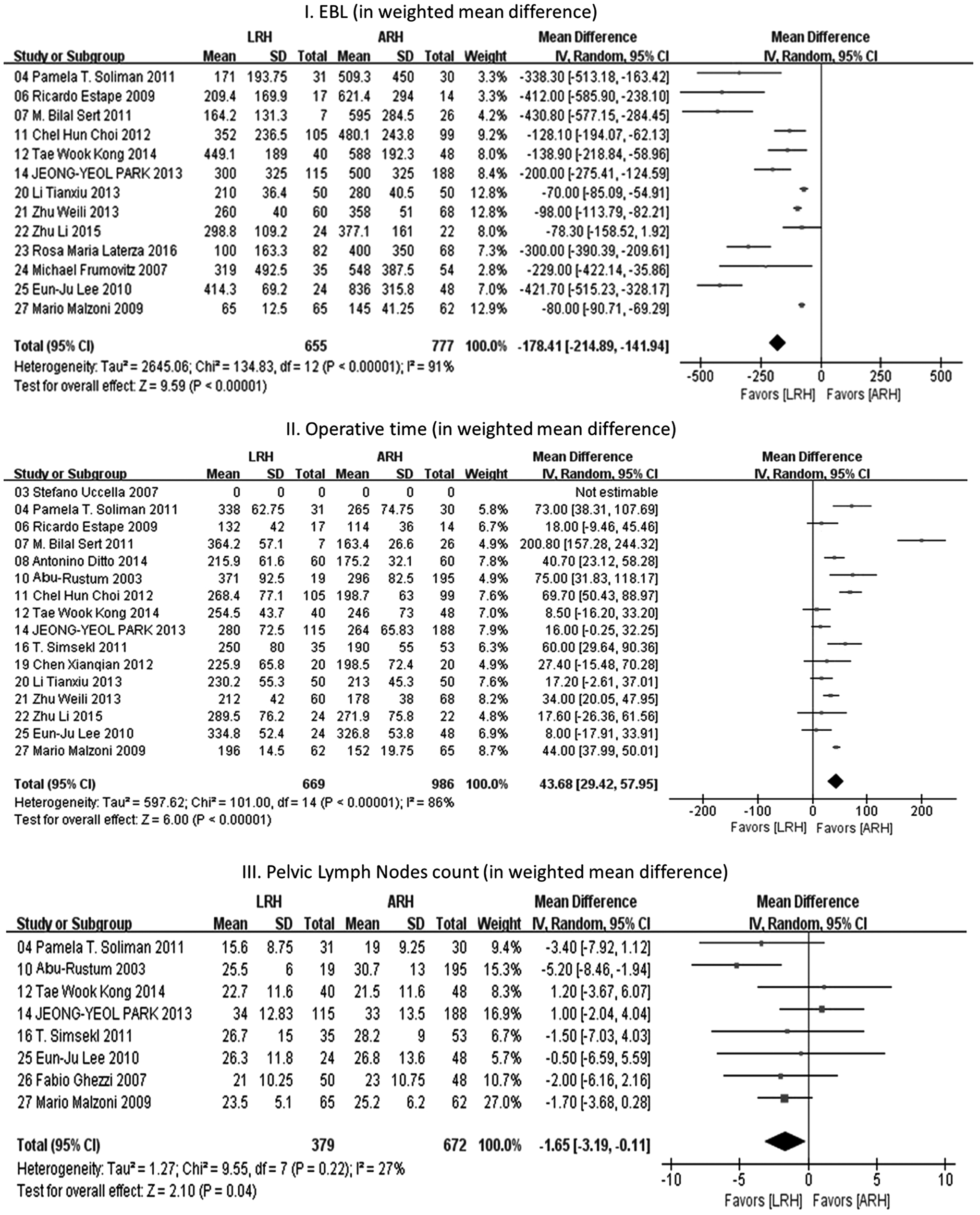
Forest plots of effect estimates of intraoperative outcomes (EBL, OT, pelvic lymph nodes count, intraoperative complications, and blood transfusion) between LRH and ARH. ARH, abdominal radical hysterectomy; EBL, estimated blood loss; LRH, laparoscopic radical hysterectomy; OT, operative time.

Forest plots of effect estimates of postoperative outcomes (hospital stay, complications, and so on) between LRH and ARH. ARH, abdominal radical hysterectomy; LRH, laparoscopic radical hysterectomy.
In comparison to ARH, LRH was associated with significantly shorter hospital stay (day) (MD = −3.17, 95% CI = −4.06 to −2.29), quicker return to normal bowel activity (day) (MD = −0.70, 95% CI = −0.96 to −0.45), shorter duration of bladder catheterization (day) (MD = −1.69, 95% CI = −2.83 to −0.55), lower EBL (mL) (MD = −178.41, 95% CI = −214.89 to −141.94), and transfusion rate (122/772 versus 493/2469, OR = 0.47, 95% CI = 0.30–0.73), but longer OT (minutes) (MD = 43.68, 95% CI = 29.42–57.95). Among the intraoperative complications, only the difference of intestinal injury between LRH and ARH was of statistical significance (6/543 versus 7/2029, OR = 3.96, 95% CI = 1.33–11.78). Moreover, LRH was linked to fewer lymph nodes retrieved (MD = −3.44, 95% CI = −5.96 to −0.92) and shorter follow-up (month) (MD = −20.37, 95% CI = −33.02 to −7.72), which can be supplementary indications.
Although LRH was associated with fewer ileus, smaller number of pelvic lymph nodes retrieved, and more frequent ureteral/vesical/vaginal fistulas than ARH, the OR or MD was of borderline significance (4/526 versus 22/1980, OR = 0.34, 95% CI = 0.12–0.91; MD = −1.65, 95% CI = −3.19 to −0.11 and 10/246 versus 2/346, OR = 3.67, 95% CI = 1.08–12.47, respectively). There was no significant difference in either the number of positive lymph nodes (91/494 versus 151/643, OR = 0.85, 95% CI = 0.62–1.17) or the incidence of overall intraoperative complications (23/560 versus 69/1976, OR = 1.14, 95% CI = 0.68–1.93) between LRH and ARH. Individually, both LRH and ARH were comparable in terms of the pooled odds of vascular injury (5/438 versus 2/1930, OR = 4.05, 95% CI = 0.85–19.24), bladder injury (15/591 versus 42/2091, OR = 1.40, 95% CI = 0.73–2.67), and ureteral injury (9/543 versus 37/2029, OR = 1.09, 95% CI = 0.40–2.99). The following postoperative parameters also demonstrated equivalence between LRH and ARH (Fig. 2). No significant differences were found in the prevalence of febrile morbidity (14/272 versus 26/366, OR = 0.65, 95% CI = 0.32–1.29) and DVT/PE (6/405 versus 17/1908, OR = 1.31, 95% CI = 0.48–3.57). Lymphocele or lymphedema and UTI did not differ between both pooled cohorts either (12/213 versus 14/241, OR = 1.46, 95% CI = 0.49–4.36; 6/262 versus 18/367, OR = 0.58, 95% CI = 0.22–1.57). Although recurrence and CCRT were less recognized in the LRH cohort, the differences were not statistically significant (42/504 versus 69/577, OR = 0.74, 95% CI = 0.49–1.13; 85/311 versus 118/417, OR = 1.07, 95% CI = 0.75–1.53) (Table 3).
ARH, abdominal radical hysterectomy; CCRT, concurrent chemoradiotherapy; CI, confidence interval; DVT/PE, deep venous thrombosis/pulmonary embolism; LRH, laparoscopic radical hysterectomy; OR, odds ratio; UTI, urinary tract infection.
Heterogeneities were substantial in the analyses of length of stay, return to normal bowel activity, follow-up, EBL, transfusion, OT, and total number of lymph nodes retrieved, whereas there was no significant heterogeneity in other analyses.
Discussion
As far as we know, we performed a robust systematic review and meta-analysis for the first time comparing LRH to ARH in treating early stage cervical cancer. We aimed to integrate multiple evidences and make a comprehensive analysis to figure out the respective advantages of LRH and its alternative approaches to RH in treating early stage cervical cancer, which can be helpful in patient counseling and decision making for equipment procurement.
The results demonstrated that LRH was associated with shorter hospital stay and duration of bladder catheterization, quicker return to normal bowel activity, and lower EBL or transfusion rate, all of which showed the superiority of LRH to ARH. Nevertheless, LRH was also linked with longer OT, possibly because of laparoscopy's lacking depth perception and limited range of motion. The steep learning curve was another potential reason. Besides, the application of LRH had little influence on the incidence of intraoperative complications, including vascular injury, bladder injury, and ureteral injury.
As for other postoperative complications, although LRH was associated with fewer ileus and more ureteral/vesical/vaginal fistulas than ARH, the ORs were of borderline significance. Therefore, we should be prudent in acknowledging the fact that LRH was remarkably superior to ARH in reducing the rate of ileus or inferior to ARH for increasing ureteral/vesical/vaginal fistulas. There was no difference in the number of positive lymph nodes either. The prevalence of fever, DVT/PE, lymphocele or lymphedema, and UTI did not differ between both pooled cohorts. Although recurrence and CCRT were less recognized in the LRH cohort, the differences were not statistically significant.
Our meta-analysis suggested that LRH was effective, safe, and embraced superiorities in most essential short-term and long-term surgical outcomes over the abdominal approach. For some terminal parameters, such as 5-year survival rate or mortality, more data were needed to enrich our analysis.
Our review was based on systematic literature search and strict inclusion criteria and included assessments of the methodological quality and risks of bias of the studies that met the predefined inclusion criteria using the NOS approach and the PRISMA guidelines. In the present work, patterns and sources of inconsistency among different study results were quantified and analyzed. The precision and accuracy of estimates can be improved as more data are used.
However, our review also had its limitations, which mainly involved the quality and quantity of the available evidence on this issue. First, the sources of publications searched from selected electronic databases were limited, and we failed to retrieve unpublished studies, thus potentially introducing inevitable publication bias. Second, included studies are mainly nonrandomized and retrospective with significant heterogeneity for some measures, which lowered the confidence in the estimates. Third, even though our search strategy disregarded language limitations, we failed to find all qualified studies in other languages, which may produce language bias. Fourth, compared with ARH, LRH is a relatively newer technique and therefore most of LRH cases are being performed in recent years, whereas ARH is more mature and more frequently being performed in earlier time. Among all the studies included in this meta-analysis, some of them reviewed patients undergoing LRH or ARH at the same period, whereas some other studies recruited a historical cohort of patients treated with ARH as the control group. For the former type, women who currently undergo ARH (instead of LRH) are likely to represent more challenging cases with larger uteri and so on, which inevitably contributed to the selection bias. While for the latter type, as the control group patients (i.e., the ARH group patients) were treated earlier than the LRH group, some parameters between the two groups would in some sense certainly be different from each other, such as the follow-up time, a parameter associated with patients' health consciousness, which has been growing as time goes on. As a result, time bias came up. Fifth, age, family history, and other covariates that may influence the incidence of the disease were also not considered. Moreover, we did not subdivide the RH into type II and III (Piver classification) in our analysis. In fact, these two types of RH bear somewhat different results especially in terms of early bladder dysfunctions. Last but not least, the cost is an important consideration when we decide on surgical approaches. However, due to lack of valid data, we failed to address this aspect. Current evidence suggests that LRH is superior to ARH with lower EBL, shorter hospital stay and duration of bladder catheterization, quicker return to normal bowel activity, and less frequent blood transfusion and ileus. LRH and ARH appear equivalent with regard to the other intra- and postoperative outcomes. Additional studies are necessary to evaluate the total cost of care and longer-term outcomes, including survival rate and mortality.
Footnotes
Acknowledgments
The authors are grateful to Prof. Jian-Hua Mao (Lawrence Berkeley National Laboratory, USA) for providing important guidance related to statistical methodology. Discussion with Prof. Xiao Han (Nanjing Medical University) and Prof. Yong-Qing Wang (Peking University Third Hospital, China) also improved the quality of this article greatly. Their gratitude is also extended to Prof. Yi-Ming Zhao (Peking University, China) for his expertise.
Ethical Approval
This article does not contain any studies with human participants or animals performed by any of the authors. (All analyses are based on previously published studies, thus no ethical approval and patient informed consent are required.)
Disclosure Statement
No competing financial interests exist.