
Abstract
Abstract
Background:
Portal hypertension is necessary for the development of most clinical complications of cirrhosis. We recently reported a novel, endoscopic ultrasound (EUS)-guided technique for direct portal pressure measurements using a digital pressure wire.
Aims:
The aims of this study were to (1) evaluate safety in an animal survival model and (2) compare direct portal vein (PV) versus transhepatic access of a first-order venule.
Materials and Methods:
Yorkshire pigs, weighing 40–55 kg. Procedures were performed under general anesthesia. PV was identified using a linear array echoendoscope and accessed with a 22-G fine needle aspiration needle preloaded with a digital pressure wire. Access was confirmed by portal venography. Mean digital pressure measurements were recorded over 30 seconds, and again after accessing a first-order portal venule in a transhepatic manner. Procedure times and video logs were maintained throughout. Animals were survived for 2 weeks. Repeat portal pressure measurements were performed before euthanasia and necropsy.
Results:
EUS-guided portal pressure measurements ranged from 3 to 11 mm Hg (mean 6.1) and were performed in a mean time of 214 seconds. There was no difference in measurement between the PV and first-order venule, or between baseline and 2-week follow-up. Five of 5 animals survived without incident. On necropsy, there was no evidence of thrombus or hemorrhage.
Conclusions:
This study represents the first survival study after EUS-guided direct portal pressure measurements using a digital pressure wire. This method appears safe, straightforward, and precise. Measurements of the PV and a first-order portal venule appear equivalent, and serial measurement seems feasible.
Introduction
T
We recently developed a straightforward endoscopic ultrasound (EUS)-based technique for direct portal pressure measurements using a digital pressure wire. 6 In a nonsurvival animal model, a 22-G fine needle aspiration (FNA) needle (Fig. 1A) preloaded with a digital pressure wire (Fig. 1B) was used to puncture the portal vein (PV) under EUS guidance (Fig. 1B). This wire features a transmitter with the potential to stream pressure data wirelessly to a remote vital signs display (Fig. 1C). Mean digital pressure measurements were not found to be statistically different from HVPG measurements obtained through a conventional transjugular approach.
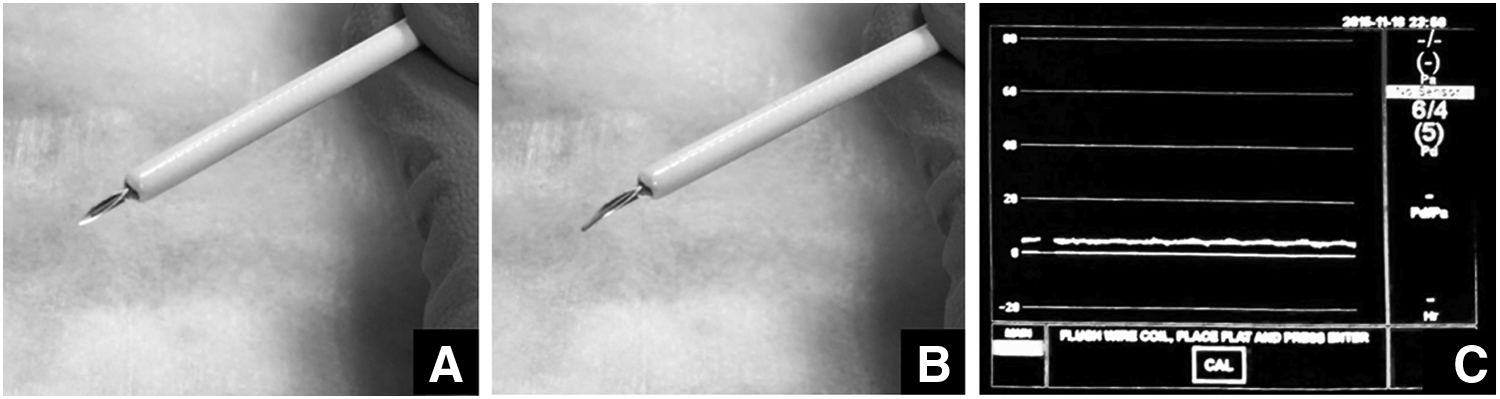
FNA needle preloaded with digital pressure wire
Our results demonstrated short-term safety, technical feasibility, and accuracy of obtaining direct portal pressure measurements compared with the gold standard approach in a nonsurvival model. This technique was reproducible and efficient. However, safety of this technique was not assessed in a survival model. Furthermore, transhepatic puncture, which may provide tamponade and prove to be safer in coagulopathic patients, was not tested.
The aims of this study were to (1) evaluate safety in an animal survival model and (2) compare direct PV access versus transhepatic access of a first-order venule. In light of our initial work demonstrating the straightforward approach for direct portal pressure measurement, we hypothesize no postprocedure bleeding, portal venous thrombi, or trauma to the liver or other intraabdominal organs. Furthermore, we anticipate similarity of pressure measurements transduced from a first-order venule through a transhepatic approach to those obtained through direct PV puncture.
Materials and Methods
Preparation of animals
Five Yorkshire pigs weighing 40–55 kg were utilized in this study at the Pine Acres Research Facility (Norton, MA) after obtaining Institutional Animal Care and Use Committee approval. All procedures were performed under general anesthesia.
Procedure: day 1
A detailed description of the endoscopic procedure used to measure direct portal pressure is described elsewhere. 6 In brief, a linear array echoendoscope (Pentax EG-387OUTK; Hitachi Preirus System, Montvale, NJ) was used to identify the PV. With a commercially available 22-G FNA needle (Medtronic/Covidien Beacon BNX System, Minneapolis, MN) preloaded with a digital pressure wire (PressureWire™ Aeris; St. Jude Medical, St. Paul, MN), the PV was punctured under Doppler imaging to ensure avoidance of other vasculature (Fig. 2A). Mean digital pressure measurements were obtained by 2 separate proceduralists. Subsequently, a first-order portal venule was identified under ultrasound and fluoroscopic guidance. This venule was accessed in a transhepatic manner, and repeat digital pressure measurements were performed (Fig. 2B). All digital pressure measurements were recorded continuously for at least 60 seconds after obtaining a stable tracing. Procedure times and video logs were maintained for subsequent review.

Passage of EUS-guided FNA needle into PV
Postprocedure
All animals were recovered and survived for 2 weeks. During this time, these animals underwent twice daily inspection to assess food intake and general appearance, and monitor for abdominal pain, shock, or bleeding. A standard diet was provided throughout.
Procedure: day 14
Before euthanasia, repeat portal pressure measurements were performed in both the PV and a first-order portal venule. After euthanasia, necropsies were performed to evaluate for thrombus or hemorrhage in both intraperitoneal and retroperitoneal spaces. Mean portal pressure measurements (±standard deviation) were calculated from the baseline, transhepatic, and pre-euthanasia approaches.
Results
Survival animal studies
All pigs tolerated general anesthesia and recovered without incident. Puncture of the PV and first-order portal venule with a 22-G FNA needle was successfully performed in all pigs. Direct pressure measurements were obtained in each of these two locations, at baseline and at 14 days. Baseline portal pressure measurements ranged from 3 to 11 mm Hg, with a mean of 6.1 mm Hg. Differences in pressure measurements between proceduralists were not statistically significant. Mean time to obtain pressures was 214 seconds (range 180–295). First-order portal venule pressure measurements performed during this initial procedure did not significantly differ from those obtained in the PV. On follow-up 2 weeks later, repeat portal and first-order portal venule measurements did not significantly differ from baseline values (Table 1). There was no intraprocedural hemodynamic instability and no procedural complications.
Postmortem analysis
On necropsy, there was no evidence of abscess, thrombus, intra-abdominal/retroperitoneal bleeding. There was no evidence of inadvertent organ damage during the puncture of the portal vasculature. The liver was harvested and revealed no evidence of trauma or abscess despite accessing a first-order portal venule in a transhepatic manner.
Discussion
The presence of portal hypertension is necessary for the clinical complications of liver disease. Portal pressures should ideally be known for optimal care of this patient population. Measurement of HVPG is currently used in practice, but it is invasive, indirect, susceptible to operator technique, and only performed in specialized centers.5,7,8 Because measurement of portal pressure is clinically important, a widely available and reproducible modality to identify portal hypertension is needed to advance the care of patients with liver disease.
We recently described an EUS-based technique for obtaining direct digital pressure measurements of the PV in a nonsurvival animal model. 6 This approach was demonstrated to be advantageous and unique for a variety of reasons, including the elimination of pressure variation from positional changes known to occur in analog systems, the delivery of real-time pressure tracings through wireless transmission, and the fact that it reflected direct portal pressure measurements, unlike HVPG measurements, which provide only a surrogate. However, the safety of this technique in a survival model and the possibility of accessing the portal venous system through a transhepatic approach were not addressed.
A few studies to date have investigated EUS-guided PV catheterization in an animal survival model. Lai et al. investigated the feasibility of EUS-guided PV catheterization in animals in both a normal and portal hypertension-induced state. 9 These animals were survived for only 4 days. Giday et al. evaluated the feasibility and safety of EUS-guided PV angiography in a porcine model with an FNA needle using carbon dioxide as a contrast agent.10,11 These animals underwent transhepatic puncture of the PV with the FNA needle and were survived for 2 weeks. There were no signs of intraperitoneal bleeding, infection, or organ damage.
This study demonstrates the safety of this technique in a survival animal model. All of the animals were survived for 2 weeks without complication. We did not observe any postprocedure bleeding, portal venous thrombi, or trauma to the liver or other intra-abdominal organs. Furthermore, there was little variation between baseline portal pressure measurements obtained by each proceduralist and between baseline values and those obtained before necropsy, both of which speak of the reproducibility of this method.
The similarity of pressure measurements transduced from a first-order venule through a transhepatic approach to those obtained through direct PV puncture also has clinical implication. These results suggest feasibility of this method in altered anatomy when direct portal access may be challenging. Furthermore, a previous study of EUS-guided PV access reported a complication of intraperitoneal bleeding and hematoma formation, 9 although this occurred in an anticoagulated model and also in the setting of prolonged needle insertion time. A transhepatic approach may provide tamponade after needle withdrawal and may prove to be safer in coagulopathic states. Further studies are required to determine the validity of this proposal.
Limitations of this study include the small sample size and inclusion of animals without underlying portal hypertension. Furthermore, although there was no evidence of bleeding during the survival period or on necropsy, additional studies are needed to determine its safety with concurrent coagulopathy.
This study demonstrates that a recently described EUS-based technique for obtaining direct digital pressure measurements of the PV is safe in an animal survival model. Ongoing animal studies and early human protocols are currently underway.
Footnotes
Acknowledgments
A.R.S. has nothing to disclose; C.C.T. is Consultant/Research Support at Olympus, Consultant at Boston Scientific, and Consultant, Royalty, Stock at Covidien; and M.R. is Consultant, Honorarium at Covidien.
Authors’ Contributions
A.R.S. performed study concept and design, acquisition of data, analysis and interpretation of data, drafting of the article, and statistical analysis; C.C.T. performed study concept and design, critical revision of the article for important intellectual content, and study supervision; and M.R. performed study concept and design, critical revision of the article for important intellectual content, and study supervision.
Disclosure Statement
No competing financial interests exist.