
Abstract
Abstract
Background:
Conventional laparoscopic surgeries of direct inguinal hernia include two methods, transabdominal preperitoneal hernioplasty (TAPP) and totally extraperitoneal hernioplasty. Both methods are performed using synthetic mesh without suturing the hernia defect and require extensive mesh coverage for not only Hesselbach's triangle but also indirect ring. For minimally invasive operation, suture of direct hernia defect was devised and performed. The purpose of this study is to evaluate the efficacy of defect wall suture of laparoscopic herniorrhaphy for direct inguinal hernia patients.
Methods:
We evaluated 210 direct inguinal hernia patients who received TAPP in Damsoyu Hospital, Seoul, Republic of Korea from September 2012 to December 2015. The patients were categorized into two groups according to TAPP techniques; cTAPP group had conventional TAPP without defect wall suture, and rTAPP group had defect wall suture TAPP. There were 99 patients in a cTAPP group and 111 patients in rTAPP group.
Results:
Operation time and postoperative hospital stay showed no difference between two groups. The postoperative pain score within the first week was significantly lower in rTAPP group than in cTAPP group (P < .001). The mean timing of a return to normal activities for rTAPP group was 3.8 days, which was shorter than 4.6 days of cTAPP group (P < .001). There was no difference in complication and recurrence rates between two groups.
Conclusions:
Defect wall suture for direct inguinal hernia had shorter operation time, faster recovery time, reduced pain, and an acceptable rate of recurrence and complication. This TAPP surgery with hernia defect wall suture that requires smaller dissection area is an effective method for treating direct inguinal hernia.
Introduction
I
Even though laparoscopic herniorrhaphy has been widely accepted with its various advantages, it is associated with a major challenge since it requires wide peritoneal dissection for the mesh accommodation without wall closing. We noted a few complications (2 bulging phenomenon and one chronic pain), which developed during the conventional TAPP (using mesh only without repairing the defect) herniorrhaphy at our institution. To modify and minimize the dissection area, we modified the conventional TAPP (using mesh only without repairing the defect, cTAPP) by adopting defect wall suture repair method that can reduce dissection area necessary for mesh placement. The defect wall suture performed along a linear line may reduce pain by dispersing tension to a wider area around the closure.
In this study, to evaluate the efficacy and outcomes of laparoscopic herniorrhaphy with defect wall suture along with the use of synthetic mesh in the management of direct inguinal hernia, we analyzed the surgical outcomes of our new technique and conventional TAPP.
Materials and Methods
From September 2012 to December 2015, 4500 inguinal hernia patients were treated at a single institution (Fig. 1). All operations were performed by a highly experienced surgeon (Lee SR, over 1500 laparoscopic operation per year). Clinical variables, including demographic characteristics, operative findings, and outcomes, were collected from medical records for adult 210 patients diagnosed with direct inguinal hernia and underwent TAPP. Indirect hernias and supravesical hernias were excluded. In the beginning of the study, patients chose one of the two operation methods after full explanation from the doctor before surgery. All direct hernia treatments performed after this study are rTAPP. The conventional TAPP (cTAPP) was performed on 99 patients, and TAPP with defect wall repair (rTAPP) was performed on 111 patients.
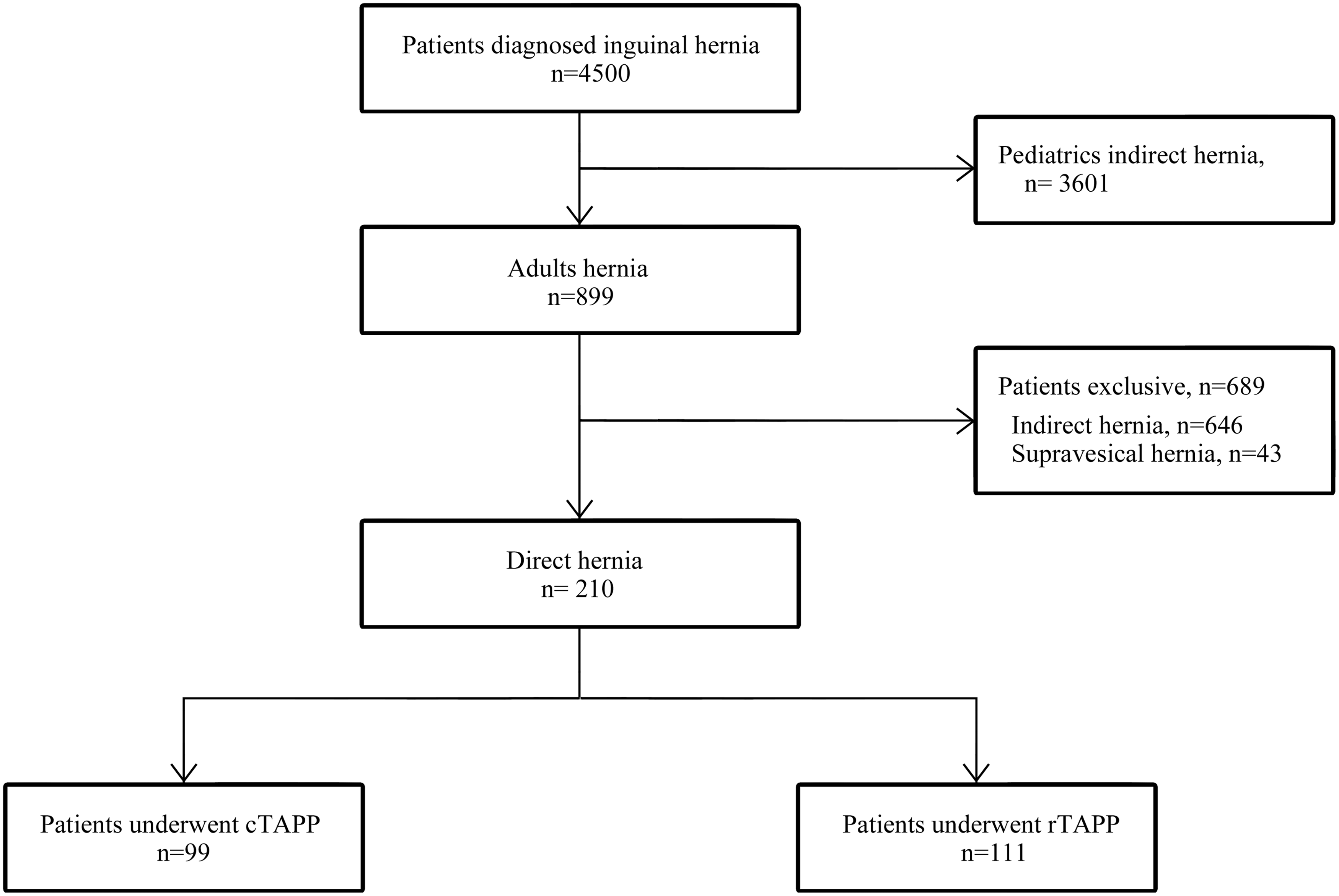
Patient enrollment distribution.
Laparoscopic herniorrhaphy technique
All patients underwent laparoscopic herniorrhaphy, using either of the two protocols: cTAPP or rTAPP. Both methods used three-port laparoscopic operation. The procedures were performed under general anesthesia in supine position. For laparoscopic system, a 5.0 mm camera and 5.0 mm instruments were used. A transumbilical 5.0 mm incision (by No.15 scalpel) was used for creation of pneumoperitoneum via a 5.0 mm trocar. CO2 pneumoperitoneum was maintained at 8–12 mmHg. Two other 5.0 mm instruments were inserted through separate 5.0 mm stab incisions in the lateral abdomen without trocars.
In cTAPP, a wide peritoneal area, including indirect area, was dissected, and lax transversalis was ligated with an endoloop. Mesh was placed in the peritoneal space without suture fixation, and then the peritoneum was closed with a continuous absorbable suture (vicryl 3–0). In rTAPP, the direct hernia defect was closed using suture with a nonabsorbable multifilament (silk 1–0). We inserted the suture needle directly through the lower abdominal area. The suture technical details are as follows (Supplementary Video S1, Suture technique details; Supplementary Data are available online at www.liebertpub.com/lap) initially we tied at the bottom of defect wall and sutured in the upward direction to the top of the defect wall, and then sutured continuously in the opposite direction until we came back down and tied at the initial knot. The knot was tied intracorporeally. The size of mesh was 10 × 13 and 6 × 7 cm2 in cTAPP and rTAPP, respectively (Fig. 2).

Comparison of rTAPP and cTAPP.
Protocols and follow-up
Diet was permitted after 1-hour observation. The protocol at our institution was that after monitoring the patients' conditions, if they are comfortable at daily activities (such as walking and eating), they were permitted to be discharged. Routinely, pain control was made with one intravenous injection (Diclofenac) after the operation. Another injection was administered only if a patient complains of pain and aches. Postherniorrhaphy pain was evaluated using the visual analog scale. Upon discharge, they were prescribed with NSAIDs medications (Diclofenac) for 3 days. Telephone interviews were performed to check postoperative status such as pain, wound state, possible symptoms of hematoma, and seroma on day 2. The outpatient follow-up routine included the physical examination after 7 days and 1 month and annual telephone follow-ups for subsequent years. Outpatient follow-up (OPD f/u) includes routine questions, and information was obtained from retrospective chart review. Patients who failed to come for OPD f/u had telephone interviews. The telephone follow-ups for the patients in this study lasted until December 2016. The range of follow-up period varied from 12 to 51 months.
Statistical methods
All statistical analyses were performed using SPSS software, version 23.0 for Windows (SPSS, Inc., Chicago, Illinois). Continuous variables were presented by mean and standard deviation. Categorical variables were presented by frequency and percentage. The Shapiro–Wilk's test was used to test for the normality of the continuous variables. As not all continuous variables were normally distributed, our choice of statistical test of continuous variables became the Mann–Whitney U test. For categorical variables, the Fisher's exact test or χ2 test was used. A P-value threshold of .05 was chosen; any univariate P-value below or equal to .05 was considered statistically significant.
Results
Patient demographics
There was no conversion to open surgery. Both groups had high proportion of males (87.9% versus. 95.5%) (Table 1). There was no significant difference in age or body mass index. Both groups had more right unilateral hernia (62.6% and 46.9%), yet, bilateral hernias were observed in both groups as well (11.1% versus 13.5%). Omentum was the most common herniated organ in both groups (98.0% versus 99.1). One incarceration was observed in each group. The duration of follow-up was similar between cTAPP group and rTAPP group. The average follow-up periods in both groups were longer than 29 months.
Categorical variables were tested by χ2 test or Fisher's exact test. Continuous variables were tested by independent samples t-test.
BMI, body mass index; TAPP, transabdominal preperitoneal hernioplasty.
Postoperative outcomes
The mean operation time of unilateral hernia was shorter in rTAPP group, but it was not significantly different from cTAPP method (P = .052) (Table 2). The mean postoperative hospital stay was longer for the cTAPP group (13.1 hours) compared with the rTAPP group (10.7 hours), but there was no statistical significance (P = .067). There was no significant difference in complication rate in both groups: 3 seroma, 1 hematoma, and 1 chronic pain in cTAPP group and 1 hematoma in rTAPP group (P = .102). In our study, 3% of patients (3/99) in the cTAPP group had seroma compared with 0% in the rTAPP group. After the syringe aspiration, all the seroma subsided. Bulging phenomenon (2%, 2/99) was only observed in cTAPP group. Postherniorrhaphy pain score was lower in rTAPP group during the first week (P < .001), and there was no difference between two groups after 1 month. There was no difference in administration of IV analgesic between two groups. The mean timing of a return to normal activities for rTAPP group was 3.84 days, which was shorter than 4.64 days of cTAPP group (P < .001). There was one recurrence in the cTAPP group due to mesh migration to hernia hole after 10 months and none in the rTAPP group so far.
Categorical variables were tested by χ2 test or Fisher's exact test. Continuous variables were tested by independent samples t-test.
TAPP, transabdominal preperitoneal hernioplasty; VAS, visual analog scale.
Discussion
Treatment of direct inguinal hernia is carried out with tension-free mesh technique to widely cover the hernia defect in open and laparoscopic surgery. The mesh repair is currently mandatory for adult direct hernia patients.4,5,7 Minimum of 10 × 15 cm2 mesh (Grade A) is recommended for secure covering with mesh, and using a smaller mesh is considered as one of the risk factors for recurrence (Level 2A).4,5 The biggest advantage of TAPP is the ability to observe the anatomical structures of hernia definitely through the laparoscopic view. This makes it possible to accurately classify a hernia into indirect hernia, direct hernia, supravesical hernia, and pantaloons hernia. The recurrence rate has been reported as 0%–6% and the complications, including hematoma, seroma, and pain. 8 Current protocols of TAPP surgeries for direct inguinal hernia include dissecting both the direct and indirect areas and covering up with mesh (Fig. 2A). However, current guideline does not provide any information on direct hernia defect wall repair in both TAPP and totally extraperitoneal hernioplasty surgeries.4,5 Hence, we developed an operation technique that sutures the hernia defect directly before applying the mesh.
The concept of this rTAPP technique was originally developed to avoid extensive dissection and to reduce the size of the mesh. The defect was sharply dissected to separate preperitoneal fat from lax transversalis fascia. The lax transversalis fascia is fixed to the suture line to reduce the occurrence of postoperative seroma. Although there is no report about the defect wall closure in direct hernia TAPP repair, there are a few reports about mesh placement with defect wall closure in ventral hernia with lower incidence rates of recurrence and seroma compared with mesh placement without defect wall closure.6,9
Seroma is a common postoperative early minor complication in endoscopic preperitoneal hernia repair, but that may delay postoperative recovery course with pain and subsequent management, and therefore, hospital stay and time to return to normal activities could be affected by seroma. Many authors have reported the rate of seroma at about 5%, and various techniques have been applied to reduce seroma development.10,11 The incidence of seromas in direct hernias can be significantly reduced when the lax transversalis fascia is inverted. 10 In case of voluminous direct hernias, the extended transversalis fascia should be inverted. In the cTAPP group, the lax transversalis was ligated with an endoloop. In the rTAPP group, the lax transversalis fascia is sutured together in defect repair (Fig. 3G). Fixation of lax transverse fascia by suturing is thought to decrease seroma occurrences, but statistical insignificance (P = .103).

Surgical procedures of rTAPP.
Despite of the suture repair, rTAPP patients had lower pain score because of smaller dissected area with suturing techniques. Suture could be thought to cause more severe tension, however, it can change the defect's shape from a circle into a line without difficulty. The diameter of the direct hernia becomes within 3 cm, which did not increase the tension. If the repair made some degree of tension that might induce pain, the pain score should have increased and affected recurrence rates. However, in our study, rTAPP group had less pain compared with cTAPP group by evaluating pain scores, and no recurrence has been detected so far. With direct suturing technique, smaller area needs to be dissected and smaller mesh could be used as well. This seems to be the reason why patients experienced less pain.
Admission time was longer for the cTAPP group since most of them were discharged a day or two after the operation, while most of the rTAPP group patients went home on the day of surgery, although there was no statistical difference (P = .067). The two groups had differences in the dissection area as well as the size of mesh. All other operation procedures were identical for both groups. This minimal difference in the recovery time seems to be directly related to the surgical technique they underwent.
Many recurrences of inguinal hernia repair using mesh are reported to occur within 2 years of operation. 12 In our study, there was one recurrence in cTAPP group after 10 months, but there was no recurrence reported for rTAPP group. Our results suggest that using a smaller mesh at least did not increase the risk of recurrence, and also the complications arising from using a large-sized mesh were mitigated.
This suturing technique acquires laparoscopic suturing training, and in-depth knowledge of the anatomical structures of the inguinal hernia to pass the learning curve. We have performed 3000 and more laparoscopic herniorrhaphies before this study, and these experiences with continuous research helped us devise an optimal laparoscopic herniorrhaphy, that is, rTAPP method. As mentioned earlier, most authors indicate that the mesh should overlap the hernia defect by at least 3 cm in all directions, and there is a significant trend toward reduced recurrence rates with increased size of mesh. Indeed, use of a small mesh almost doubles the risk for recurrence. 13 Other literatures also reported that the mesh size affects the recurrence rate in TAPP surgeries.14,15 Among patients who received cTAPP with 13 × 10 cm2 size anatomical mesh, there was one case of recurrence within 2 years, and two cases of pseudorecurrence (i.e., mesh eventration) during the follow-ups several months later. This symptom was reported after ventral hernia repair without defect closure.16,17 After suturing the hernia defect using our rTAPP method, the suture line remains at ±2 cm. Due to the suture, there is significantly lower risk of migration, so we used an ∼6 × 7 cm2 round-shaped mesh (Fig. 2B). Most indirect inguinal hernia occurs when processus vaginalis or canal of Nuck is open. The reason for covering the indirect area with mesh for the direct inguinal hernia patients is not to prevent indirect hernia but to simply overlap a large area around the defect. With defect wall repair, we can overlap the defect area by over 3 cm in all directions, without dissecting the indirect area (Fig. 3J). There are many important anatomical features in the indirect area, including spermatic cord, gonadal vessel, “Triangle of Pain,” and “Triangle of Doom,” so reducing necessary dissecting area can also lower the risk of injury.
It should be noted that this is a retrospective study, and this study was conducted at a single center. The follow-up period was not long, and so, longer term follow-up would be required to obtain the recurrence rate. To obtain the long-term recurrence results, we plan to keep monitoring patients. Statistical significance on pain score or time to return to normal activities might not mean a lot, but at least statistics revealed that patients with rTAPP had better results than patients with cTAPP. Although it was a relatively short-term observation, our comparative results on complications in the two groups yielded meaningful results.
In conclusion, in the laparoscopic direct inguinal hernia treatment, hernia defect wall closure technique with continuous running suture can reduce the dissection area and minimize the risk of injury of important organs in the indirect area. With advantages such as lower pain, faster recovery, acceptable complication, and recurrence rates, rTAPP technique is worthy of optimal minimally invasive surgery in treating adult inguinal hernia patients.
Footnotes
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.