
Abstract
Abstract
Background:
A multimodal treatment has been applied for patients with rectal gastrointestinal stromal tumor (GIST) that represents 5% of the total localization. Meanwhile, transanal endoscopic microsurgery (TEM) offers a minimally invasive method for full-thickness tumor excision with negative margins and low morbidity. We report the single most extensive analysis of data from China to evaluate the feasibility and safety of the procedure combined with neoadjuvant imatinib therapy to treat patients with rectal GISTs.
Materials and Methods:
All the clinical data were obtained for patients who underwent the procedure in our hospital from February 2008 to May 2015, and the data were retrospectively analyzed.
Results:
Full-thickness excision by TEM was performed on 25 patients with rectal GIST by using primary surgical excision, 8 of whom had received perioperative chemotherapy after histopathological confirmation under the care of medical oncologists. No obvious postoperative complications were observed. The average tumor downsizing ratio was 14.5%, which apparently enabled oversized tumors to be resected by TEM. The comparative risk did not increase during or after the procedure. We did not observe recurrence or metastasis in any of the 25 patients during the median 3-year follow-up period after the procedures.
Conclusions:
The perioperative imatinib treatment effectively allowed oversized rectal GIST tumors to be resected by TEM, and the procedures did not exhibit an increased risk. Exclusively, the TEM procedure with alternative neoadjuvant imatinib therapy is a feasible and safe modality for treating patients with rectal GISTs.
Introduction
G
The population-based annual incidence of GISTs is reported to be 10 to 14.5 cases per million, and it has continuously risen in China in recent years.2,3 Among sporadic GISTs dispersed along the GI tract, rectal GISTs accounted for only 5% of the total prevalence, which is much <60% prevalence in the stomach and 30% prevalence in the small intestine.4,5 However, rectal GISTs have a worse clinical outcome and poorer prognosis than other GISTs. The clinical presentation of rectal GISTs may vary from profuse GI bleeding or severe abdominal pain to incidental endoscopic discovery. 6 Due to a lack of sufficient experience in recognizing GISTs, these tumors are not frequently diagnosed before the pathological examination, even when they are characterized by clear boundaries and high vascularity. Hirota first revealed the molecular mechanism of GISTs and showed that the mutated KIT gene and PDGFRA played important roles in tumorigenesis. 7 Furthermore, as the mainstay treatment for primary rectal GISTs, complete resection without mandatory lymph node resection has a good clinical outcome for resectable tumors, but it is accompanied by high recurrence and metastasis rates within 2 years. 8 Imatinib, a selective tyrosine kinase inhibitor targeting c-KIT or PDGFRA, has been proved to be an effective adjuvant therapy, improving survival in patients with GISTs and a high risk of recurrence.9,10 A randomized double-blind clinical trial by the American College of Surgeons Oncology Group (Z9001) showed a significantly lower recurrence rate than the placebo group. 10 Moreover, NCT00116935 revealed that 36 months of imatinib therapy improved the overall and recurrence-free survival of patients with GIST who were at a high risk of recurrence compared with those of patients undergoing 12 months of imatinib therapy. 11
The larger size and narrower surgical vision of rectal GISTs pose great challenges for general surgeons treating patients with these tumors. The clinical efficacy of transanal endoscopic microsurgery (TEM) in treating various benign tumors has been widely reported, and TEM is a safe and minimally invasive procedure that might be an alternative treatment for patients with rectal GISTs. Although strong clinical evidence is lacking due to the rarity of GISTs, TEM provides multiple advantages over conventional excision methods, such as improved visualization, exposure, access to proximal lesions in the rectum, and, most importantly, the preservation of the pseudo-membrane of benign tumors, which reduces the risk of recurrence and metastasis. 12 Furthermore, the accurate determination of margins is more easily achieved. Therefore, TEM provides surgeons with a greater degree of resection when treating patients with rectal GISTs, ensuring a better clinical outcome without severe, invasive interference. In addition, few studies have investigated the combination of the TEM procedure and neoadjuvant therapy. Because only 2 single case studies have reported the combination of the TEM procedure and neoadjuvant therapy,13,14 we now report our experience in Peking Union Medical College Hospital since 2008.
Patients and Methods
From February 2008 to February 2015, full-thickness excision using TEM was performed on 25 patients with rectal GISTs who were diagnosed with imaging modalities, such as endoscopic ultrasounds (EUS) and endoscopy, in the Department of General Surgery at Peking Union Medical College Hospital. A clinical database of these 25 patients was created, which included tumor features (distance from the anal valve, margins, and histopathology), operative details (operative method and postoperative complications), preoperative and postoperative evaluations of malignancy and recurrence, and medications (neoadjuvant and adjuvant therapy). All procedural protocols were approved and supervised by the Ethics Committee of Peking Union Medical College Hospital.
Inclusion criteria
Only patients with gross lesions with a maximal diameter <5 cm and a distance from the anal verge to the distal margin of lesions <9 cm were included; patients with lymph node involvement and distal metastasis were excluded. No other concurrent severe systemic diseases, such as cancer or severe metabolic disease, were detected. Tumor size and mitotic activity in 50 high-power fields (HPF) were considered important prognostic factors. In addition, colonoscopy and further EUS were performed for all patients. However, for patients with a risk of developing malignant GIST tumors, abdominal and pelvic computed tomography (CT) scans were performed to exclude the possibility of metastatic disease. Patients with tumor size >3 cm received neoadjuvant imatinib to treat low-grade rectal cancer.
Surgical techniques
Based on the results of routine preoperative colonoscopy and EUS, we evaluated the tumor location and size, the invasion depth, and the status of vessels and lymph nodes. All the operations were performed under general anesthesia. The position of the patient was determined based on the location of the tumor to ensure that the lesion was located at the bottom of the operating field and to obtain the best surgical field and view. A clear margin was preoperatively defined as at least 0.5 cm. Absorbable thread and silver clips were utilized to seal the defect during the operation. Tight suturing was the method of choice used to prevent severe postoperative complications (GI bleeding, anastomotic leakage, and stenosis of the rectal lumen) (Fig. 1). A tattoo or thread knot was highly recommended during the previous rectal endoscopy to facilitate the removal of the residual tumor after endoscopic polypectomy.
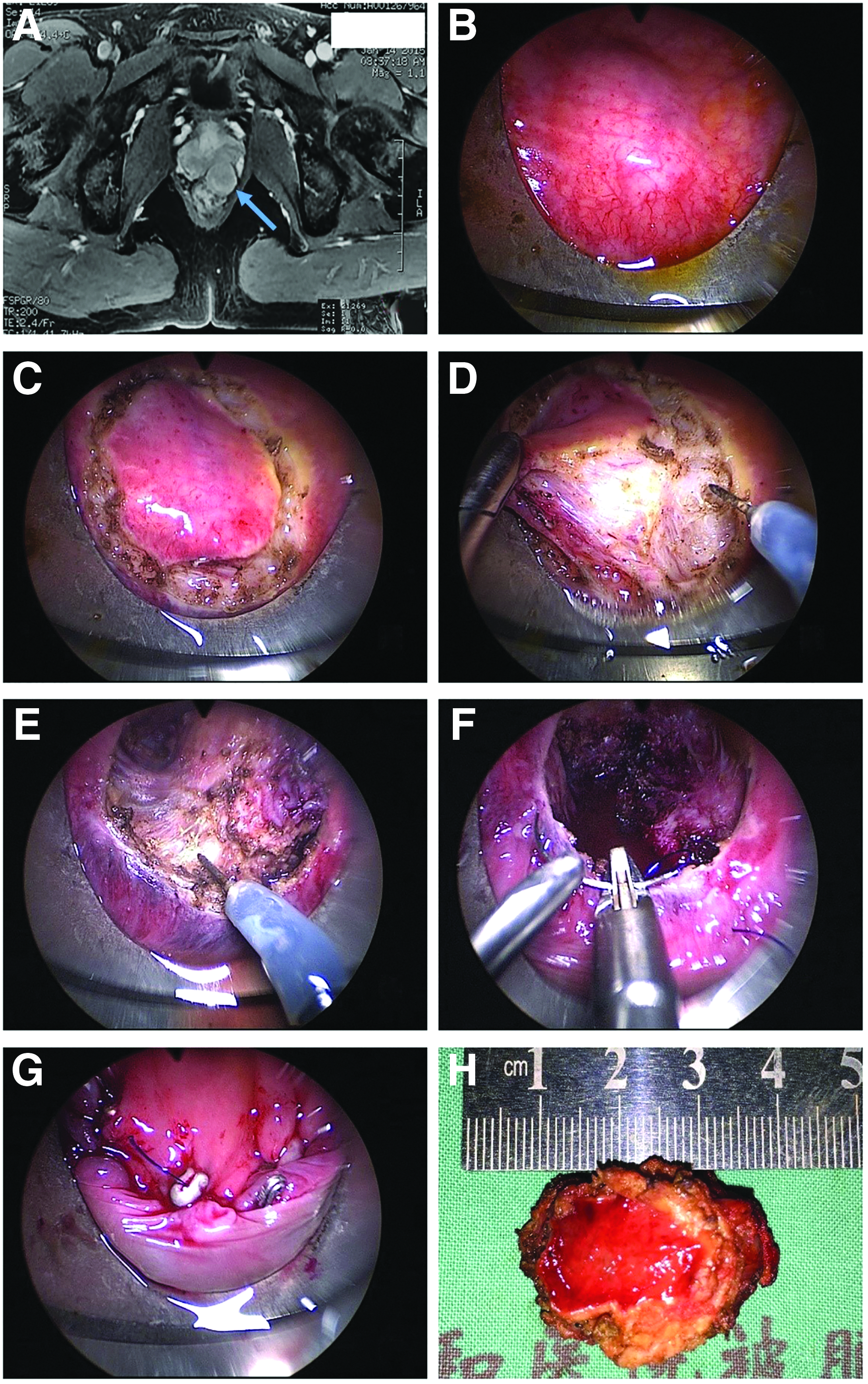
TEM procedure for rectal GIST.
Neoadjuvant therapy
Patients with a higher risk of recurrence and metastasis were medicated with 400 mg of imatinib mesylate (Gleevec) once daily under close supervision by oncologists, who evaluated and treated the corresponding adverse effects. In detail, patients with unclear adhesions between the tumor and surrounding normal tissues, a higher mitotic index (>5 HPF), and oversized tumors required the administration of a standard imatinib mesylate dosage for at least 6 months before surgery and 6 months postoperatively. Abdominal and pelvic magnetic resonance imaging (MRI) and CT were performed to evaluate the decrease in tumor size before and after the neoadjuvant imatinib therapy and to reassess the patient's risk of developing progressive diseases.
Follow-up
The guidelines of the National Comprehensive Cancer Network suggest abdominal and pelvic CT scan surveillance every 3 months for 3–5 years and annually thereafter to evaluate the postoperative clinical outcomes after complete resection. Less frequent surveillance may be acceptable for small tumors (<2 cm). Moreover, even as an anal/sphincter-preserving procedure, TEM incidentally damaged the lower anal canal and disrupted the function of the anal sphincter, causing impairments in defecation function. Patients underwent Williams grading and scoring for anal incontinence 15 and anorectal manometry 6 months after the procedure to evaluate the function of the rectum, particularly the anal sphincter. All the patients were included within our survivorship surveillance program for more than 18 months after the procedure.
Statistical analysis
Student's t test and the chi-square test were performed by using the SPSS statistical software to completely analyze and summarize the obtained data. A p-value <.05 was considered significant.
Results
Patients and demographics
Between February 2008 and February 2015, 25 patients with rectal GISTs consecutively underwent a TEM procedure, all with final pathological confirmation. No patients had undergone a previous endoscopic polypectomy. Fifteen patients were men, and 10 were women. The patients' ages ranged widely from 27 to 75 years, with a median age of 45. Among the patients, 11 were diagnosed incidentally by endoscopy performed during a medical checkup, whereas the remaining patients had variable clinical presentations ranging from mild abdominal pain to severe hematochezia. All 25 patients underwent TEM for primary tumor excision (primary excision group); 8 patients received perioperative neoadjuvant chemotherapy (imatinib 400 mg once daily) under the care of medical oncologists.
Tumor characteristics
The excised tumors ranged in size from 0.3 to 5.3 cm, with a mean size of 1.85 ± 1.15 cm. The distance from the anal verge to the lower border of the tumor ranged from 3.0 to 9.0 cm, with a mean value of 4.52 ± 1.80 cm. Thirteen tumors were located on the anterior wall of the rectum, 9 tumors were located on the posterior rectal wall, and the 3 remaining tumors were located on the lateral wall (Table 1). The histopathological examination confirmed that all the tumors were mesenchyme-derived GISTs; 100% exhibited positive staining for CD34, 96.0% were positive for CD117, 12.0% were positive for S100, and 16.0% were positive for small muscle actin (SMA). With the exception of 4 patients with a Ki-67 index between 3% and 5%, the Ki-67 index of most patients was < 1%. TNM Classification of Malignant Tumor (TNM) staging was performed and 19 patients had T1N0M0 tumors, 5 patients had T2N0M0 tumors, and 1 patient had a T3N0M0 tumor. Only 3 patients were graded stage IIIA, and the other patients were graded no higher than stage II. Therefore, with the exception of the 3 patients in the prognostic group 2, 23 patients were grouped into prognostic group 1. 16
A, anterior wall; L, lateral wall; P, posterior wall; SD, standard deviation.
Procedure
The same professional healthcare group performed all the procedures for all 25 patients over the past 7 years. The surgical duration ranged from 70 to 120 minutes, with a small quantity of blood loss, and all specimens were well circumscribed. No severe postoperative complications were observed before discharge (e.g., GI bleeding, anastomotic leakage, stenosis of the rectal lumen, peritonitis, fistula, and fecal incontinence). Most patients were placed in the supine position (for patients with tumors on the posterior wall) or in the prone position (for patients with tumors on the anterior wall), and full-thickness resection of the rectum and the surrounding mesorectum was performed by using TEM. No lymphadenectomies were performed, based on the complete preoperative diagnostic imaging assessment and the rapid histopathological evaluations performed during the procedures. No conversions to open transabdominal procedures occurred. All excisional margins (100%) of the specimens were negative, confirming the R0 resections. Most patients started walking on the first postoperative day, with per-oral intake on the second postoperative day. A liquid diet was initiated on day 3. The hospital stay ranged from 6 to 10 days, with a median of 7 days (Table 2). Compared with patients in the neoadjuvant-combined group and the solely surgically treated group, obvious distinctions were not observed in many aspects used to assess the safety, feasibility, and invasiveness of the surgery (Table 2).
NS, not significant; HPFs, high-power fields; SD, standard deviation.
Neoadjuvant chemotherapy
Eight patients received preoperative imatinib therapy for 6 months and postoperative imatinib therapy for an additional 6–12 months. Compared with the patients who were treated with surgery alone, these patients were assessed as high risk during the preoperative evaluation, as they had lesions with a diameter >3 cm or pathological results, indicating the malignant potential of the tumor, such as high mitosis rates or adhesion to surrounding tissues. According to the MRI evaluation, the mean rate at which the preoperative chemotherapy reduced the tumor size in these 8 patients ranged from 40% to 9.9%, allowing for an average partial 14.5% ± 10% decrease. This decrease in tumor size suggested that tumors should be resected by TEM rather than by transabdominal anterior resection (Fig. 2). Postoperative imatinib (400 mg daily) was administered 1 month after surgery for an additional 6–12 months before follow-up evaluations were performed.
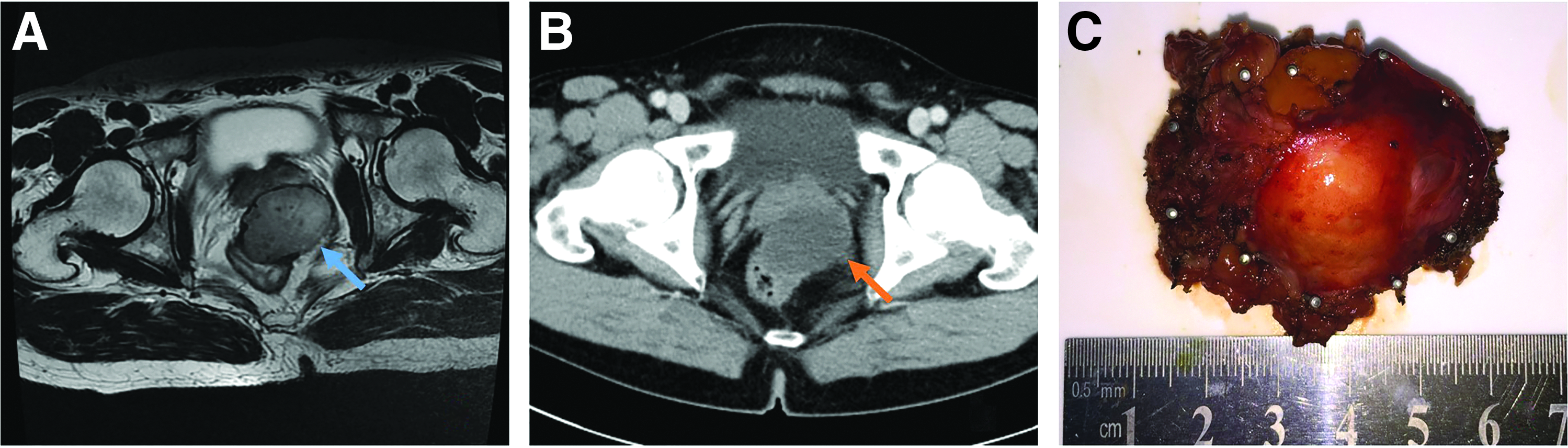
Combination of neoadjuvant imiatinib and TEM for rectal GIST. Male (50 years): Tumor in rectum was found because of difficult defecation and the biopsy pathology was GIST. The patient received imiatinib 400 mg qd for 6 months. The TEM was performed after 8 weeks of imiatinib withdrawal.
Follow-up
None of the 25 patients who underwent our follow-up protocol showed recurrence, local invasion, or malignant transformation and were symptom free according to our multipronged evaluations, including physical examinations, imaging studies, and laboratory tests. Patients were followed for a median period of 36 months (ranged 16–90 months). In addition, as mentioned earlier, 8 patients continued to self-medicate with 400 mg of imatinib per day for 6 months to 1 year as an adjuvant therapy. These patients were under the care of oncologists from the Department of Oncology in Peking Union Medical College Hospital to prevent potential bias or low compliance. Nonspecific vomiting, diarrhea, edema, flushing, fortuitous fever, and slight neutropenia were observed during the treatment and were not accompanied by severe adverse effects. The excellent overall tolerance of this prolonged chemotherapeutic treatment probably lowered the risk of disastrous events, such as recurrence and metastasis. Based on Williams grading, patients exhibited progressively improved defecation function. Most patients were rated grade B and grade A 6 months after surgery.
Discussion
Compared with GISTs in the stomach and small intestine, the prevalence of rectal GISTs is quite low (4%), and it is considered a relatively rare disease. 17 Although GISTs are sporadically reported in the rectum, several surgical methods have been reported as surgical management tools for these GIST lesions, which remain the choice of treatment. Abdominoperineal resection (Miles' operation), posterior/total exenteration, partial excision of the rectal wall, local excision, Hartmann's operation, and lower anterior resection (Dixon operation) are examples of conventional surgical methods that are used to treat patients with rectal GISTs. 18 Laparoscopic sphincter-preserving surgery after chemoreduction and modified laparoscopic intersphincteric resection are also used to treat large lower rectal GISTs.19–21 Transanal minimally invasive surgery was recently adopted as an alternative surgery for 1 patient with a very small lesion (1 cm) in 2016. 22 Surgeons traditionally choose their treatments based on the patient's history and biological traits. 23 The evolution of surgical methods for treating rectal GISTs represents the related progression in targeted treatments with less trauma and sustained clinical results. Therefore, as reported in several studies, TEM is still the mainstream method of local excision treatment for lower risk patients with rectal GISTs. Nevertheless, the lack of well-designed case series and reports make it difficult for researchers to establish a consensus.
Meanwhile, imatinib, which has previously been shown to be effective at reducing tumor volume, became the first-line therapy for advanced GISTs. 21 With the exception of tumor downsizing, neoadjuvant imatinib therapy increases the likelihood of sphincter conservation, specifically for patients with distal lesions, such as pelvic tumors.
According to several independent studies, patients who were treated with a combination of surgical management and imatinib exhibited longer disease-free survival, underscoring the advantages of this preoperative therapy.18,21,24,25 In addition, in the only case report, a patient with a rectal GIST who was treated with TEM procedures had a good prognosis, indicating the great potential of this alternative treatment. 25 However, the lack of large patient series with long-term follow-up observations after TEM and preoperative imatinib therapy encouraged us to further address this issue.
As shown by the data in the present study, the majority of patients diagnosed with T1N0M0 (19/25) who were treated with the TEM procedure generally exhibited excellent clinical outcomes. With a median follow-up period of 36 months, the disease-free survival was a reliable index, and none of the patients exhibited local recurrence or distant metastasis. Despite the relatively lower risk of developing progressive disease, longer follow-up periods might be required to observe the clinical outcomes of long-term survival.
Because patients with lower stage rectal GISTs might require follow-up periods of >5 years due to delayed local recurrence and distant metastasis, the estimated 5-year disease-free survival rate is probably insufficient to completely illustrate the overall clinical outcomes.
Technically, lymph node dissection was unnecessary due to the rarity of GISTs that had spread via the lymphatics and the lower tumor stage in our patients. 26 According to the study by Miettinen et al., 6 patients with smaller rectal GISTs between 2 and 5 cm have a low-to-moderate risk of recurrence/metastasis after resection, independent of the mitotic rate. Moreover, our tumor size cut-off value was 3 cm, based on our experience in treating lower grade colorectal carcinomas and avoiding an overly narrow surgical vision and unwarranted surgical trauma. A distance of 9 cm between the lower edge of lesions and the anal valve was also attributed to the limitations of the TEM procedure itself. In contrast to multimodal surgical treatments that have previously been performed in our hospital, the TEM procedure obviously provided many benefits to these patients, including a minimally invasive procedure, faster recovery, much less blood loss, a shorter procedure duration, and even a shorter duration of hospitalization. The duration of the procedure was 94.6 ± 11.3 minutes, which was much quicker than other procedures, which range from 100 to 150 minutes. The preservation of the pseudo-tumor membrane also remarkably reduces the risk of recurrence or potential metastasis. The longer hospitalization periods observed in the perioperative therapy group might be ascribed to the neoadjuvant medication, which reduced the rate at which the wounds healed. However, due to the diversification of surgical methods, patients' natural histories, and the tumors' biological behaviors, statistically we were not able to draw significant conclusions. A larger clinical patient series will be the focus of our future studies.
The optimal duration and inclusion criteria for chemoreduction remain controversial. Based on the Fletcher prognostic scale, the tumor size and mitotic counts are the two exclusive factors predicting prognosis. The patient's postoperative anal/sphincter function should be retained as much as possible. The chemotherapy-induced decrease in the tumor size provides a wider surgical visual field, decreases the intraoperative possibility of tumor rupture, and preserves the patient's normal defecation function to a great extent. 27 In the chemoreduction group, 6 patients had tumors larger than 3 cm, with 3 having the lesions that adhered to or shared vague boundaries with the normal surrounding organs or tissues. In addition, 3 patients had a high mitotic rate, with a Ki-67 rate >3%. Based on the surgical requirements for TEM mentioned earlier and the expectation of reducing the risk for our patients during and after the procedures, this subgroup of our patients received imatinib medication as a neoadjuvant therapy. Patients were required to take this medication for different time periods, due to the unequal probability of malignant transformation (from 6 months to 1 year).
Although we concluded that TEM had encouraging results as a treatment for patients with rectal GISTs, this study still has some limitations, including its retrospective design and the lack of a control group. We also admit that most of these patients had lower stage GISTs, and some procedures were performed at the patient's request. We were unable to perform a thorough review and comparison with other studies due to the lack of publications reporting a similar clinical series. As reported in previous detailed studies,13,14 2 patients who received 6 months of imatinib treatment and subsequent TEM required radical resection of the remnant tumor. Although the MRI showed 4.6- and 5.2-cm tumors that were contiguous with the prostate and the anal sphincters or rectovaginal septum, respectively, the lesions of our patients were smaller and more isolated. The average 14.5% reduction in tumor size after the 6-month treatment observed in our study was much <17% and 23% reductions observed in the previous case reports after 6 months, which may be explained by the higher staging and higher mitotic rate reported in previous studies, indicating a better response to imatinib mesylate. Therefore, after 6 months of treatment with imatinib mesylate, we strongly recommend that imaging tests should be reassessed to ensure that the tumors fulfill our inclusion criteria. If the tumors still do not meet our criteria, the duration of chemoreduction or other surgical procedures should be extended. Despite the lack of strong clinical evidence, we provide a flowchart summarizing our strategy as a reference (Fig. 3).
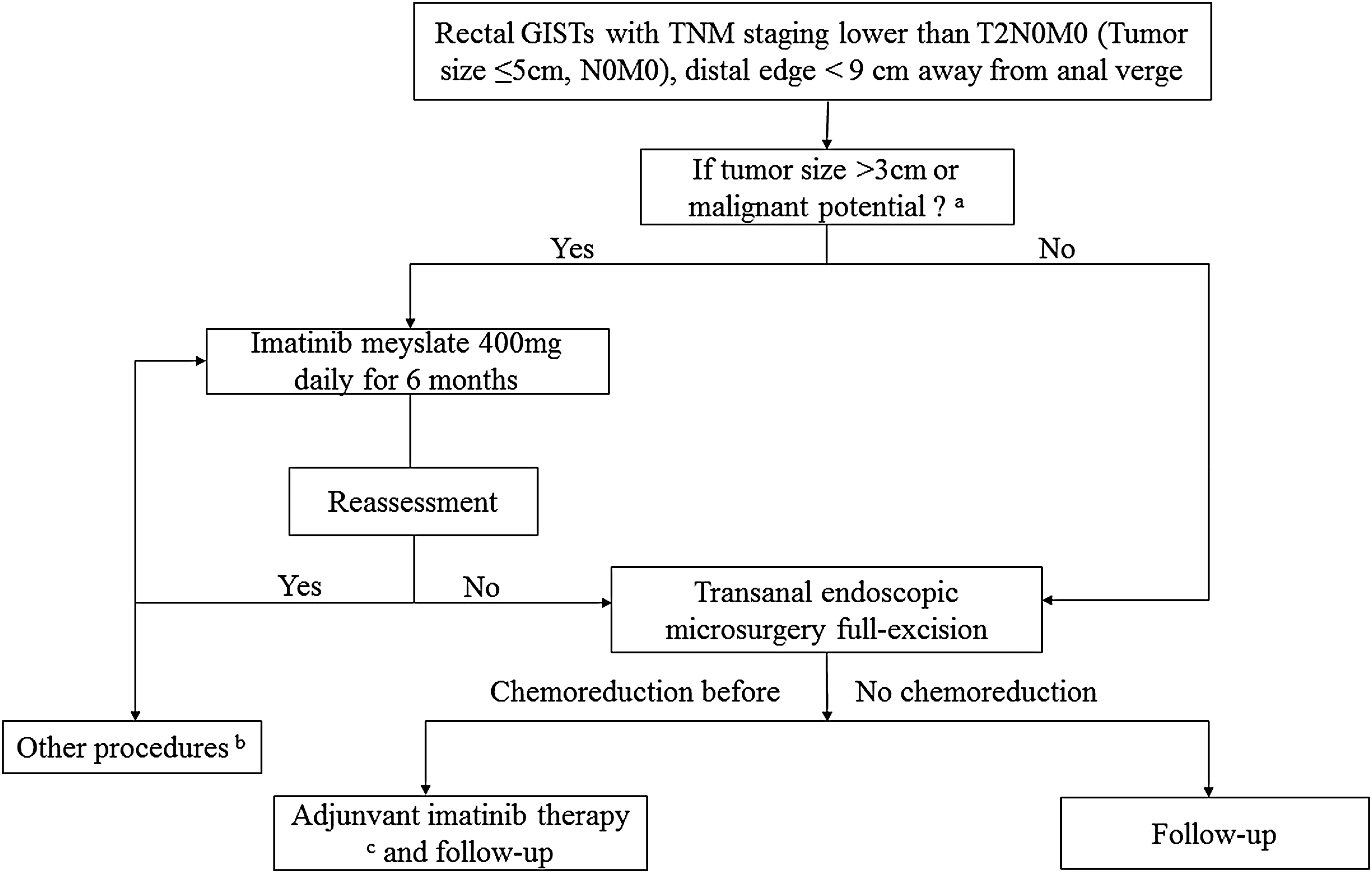
Strategy for lower grade rectal GISTs. aHigh mitotic rate or adhesion to surrounding tissues. bAbdominoperineal resection (Miles' operation), posterior/total exenteration, partial excision rectal wall, local excision, Hartmann, and lower anterior resection (Dixon operation), for example. cThe duration of adjuvant therapy should be decided grounded on the patient's periodical imaging tests results and postoperative defecation function assessment. GIST, gastrointestinal stromal tumor; TEM, transanal endoscopic microsurgery.
Because the clinical application of chemoreduction combined with TEM for patients with lower grade rectal GISTs has become widespread, more reports involving larger series will be reported in the next few years. However, to the best of our knowledge, our article is the first and largest describing the effectiveness of full-thickness excision of rectal GISTs using TEM after tumor downsizing in China. Although the evidence is inadequate, TEM alone or TEM after chemoreduction is a safe and reliable procedure for the full-thickness excision of lower stage rectal GISTs. Therefore, even with the lack of data from a large series, the comparison of the data from the two groups enabled us to propose a suggested strategy based on a defined dataset and parameters, regardless of our limitations due to the rarity of this disease.
Footnotes
Acknowledgments
We would like to express our sincere gratitude to all those who helped us work on this study. This work was mainly conducted by Doctor Han and Doctor Xu. Many people have offered us valuable help in designing and conducting this study, especially Professor Huizhong Qiu and Professor Yupei Zhao in the Department of General Surgery.
X.H.: data analysis and interpretation, drafting the article; J.X.: data acquisition and drafting the article; H.Q.: conception and design of the study; G.L.: surgeon for all operations.
Disclosure Statement
No competing financial interests exist.