
Abstract
Abstract
Background:
Intravenous injection of indocyanine green (ICG) is used to illuminate extrahepatic biliary anatomy. Fluorescence of biliary structures may lower surgical complications that can arise due to inadvertent injury to the common bile duct. We describe a method of injecting ICG directly into the gallbladder to define the cystic duct and common bile duct anatomy.
Materials and Methods:
A standard laparoscopic cholecystectomy was performed using a laparoscope with near-infrared imaging capability. Before dissection, the gallbladder was punctured with a cholangiogram catheter or a pigtail catheter to aspirate the bile within the gallbladder. The aspirated bile is mixed with ICG solution, which is reinjected into the gallbladder to fluoresce the gallbladder, cystic duct, and common bile duct structures.
Results:
Eleven patients underwent direct gallbladder ICG injection for fluorescence cholangiography during cholecystectomy. Direct gallbladder ICG injection clearly defined the extrahepatic biliary anatomy, including the cystic duct–common bile duct junction, by fluorescence. In addition, the dissection plane between the gallbladder and the liver is highlighted with the gallbladder ICG fluorescence.
Conclusions:
Direct gallbladder ICG injection provides immediate visualization of extrahepatic biliary structures and clarifies the dissection plane between the gallbladder and the liver bed.
Introduction
L
Indocyanine green (ICG) fluorescence, visualized with near-infrared (NIR) imaging, can improve visualization and provide detailed anatomical mapping of the biliary structures. Intravenous (IV) injection of ICG has become a useful adjunct for confirming anatomy in adult laparoscopic cholecystectomy.10–15 The current technique involves preoperative IV injection of ICG, which is excreted into the bile, causing biliary fluorescence when viewed with NIR light. However, there are two significant drawbacks to this technique: (1) lag time between injection and peak fluorescence can make the ideal timing of IV injection problematic and (2) the background fluorescence of the liver can interfere with optimal viewing of the extrahepatic biliary structures. 16 We describe a new technique of direct ICG injection into the gallbladder, which provides immediate illumination of relevant biliary system during laparoscopic cholecystectomy. The intent of this technique is to minimize bile duct injury and optimize visualization without compromising surgical efficiency.
Materials and Methods
Surgery and equipment
Institutional review board approval was obtained for the purpose of the study (#16003). All patients underwent laparoscopic cholecystectomy with traditional four-port technique: 12 mm umbilical port and three 5 mm ports in the right upper quadrant. All procedures were performed using a laparoscopic tower and 30-degree 5 mm laparoscope with NIR imaging capability (Stryker Corporation, Kalamazoo, MI).
ICG preparation and injection
Before the procedure, a 0.25 mg/mL ICG solution (IC-GREEN; Akorn, Inc., Lake Forest, IL) is prepared on the surgical back table. To make this solution, a 25 mg vial of ICG powder is dissolved in 10 mL sterile water to create a 2.5 mg/mL solution; then 1 mL of this solution is further diluted in 9 mL sterile water to create the 0.25 mg/mL solution.
Once the fundus is grasped and retracted, a needle-tipped Kumar cholangiogram catheter (Nashville Surgical Instruments, Springfield, TN) is introduced through the 12 mm umbilical port, adjacent to the camera. The Kumar catheter, guided by a grasping or dissecting instrument, is used to puncture the infundibulum of the gallbladder. Nine milliliters of bile is aspirated from the gallbladder into a syringe and mixed with 1 mL of the 0.25 mg/mL ICG solution, creating a 0.025 mg/mL ICG-bile solution. This solution is then reinjected into the gallbladder (Fig. 1). The premixed ICG-bile solution glows immediately upon injection with no lag time, quickly filling the gallbladder and spreading through the cystic duct into the extrahepatic bile ducts. The catheter is removed and the puncture site pinched closed with a Maryland grasper. Dissection is then performed under either ambient light or NIR mode. The surgical view of the gallbladder dissection is toggled back and forth between the two viewing modes.

Diluted ICG-bile solution is injected into the gallbladder infundibulum, which immediately fluoresces. ICG, indocyanine green.
Alternatively, the dilute ICG-bile solution can be injected into the gallbladder fundus through a pigtail catheter, which can be placed using the Seldinger technique. A pleural/pneumopericardial drainage set, which contains a needle, plastic dilator, wire, and 8Fr pigtail drainage catheter (Cook, Inc., Bloomington, IN), is used. With the gallbladder lifted cephalad with a grasper, a needle is inserted through the skin into the fundus of the gallbladder. A guidewire is then passed into the gallbladder. The subcutaneous muscular tract is then dilated with a dilator. The pigtail catheter is then passed over the wire into the gallbladder. The passage of the pigtail catheter through the gallbladder wall can be assisted by grasping the catheter with a Maryland grasper and applying force as it is pushed into the gallbladder. Once the catheter is within the gallbladder, the wire is removed. The pigtail catheter can be left in place during the cholecystectomy to prevent leakage of bile into the surgical field, which could limit the efficacy of this technique by generating background fluorescence and decreasing the quality of the NIR image.
Results
Eight patients underwent elective laparoscopic cholecystectomy for biliary colic, one patient for biliary dyskinesia, and two patients had urgent procedures for acute cholecystitis. The average age of the patients was 16 years. Seven patients were female and four were male. One of the patients with acute cholecystitis had a total occlusion of the cystic duct with a stone. Due to the obstruction, the entire length of the cystic duct could not be visualized with the ICG fluorescence. For this patient, the gallstone located within the cystic duct was slightly milked toward the gallbladder with a Maryland dissector to allow the bile and dye to drain. A metal clip was applied at the original position of the milked gallstone. For the remaining patients, the entire length of the cystic duct could be visualized as well as the junction of the cystic duct and common bile duct (Fig. 2). There were no postoperative complications.
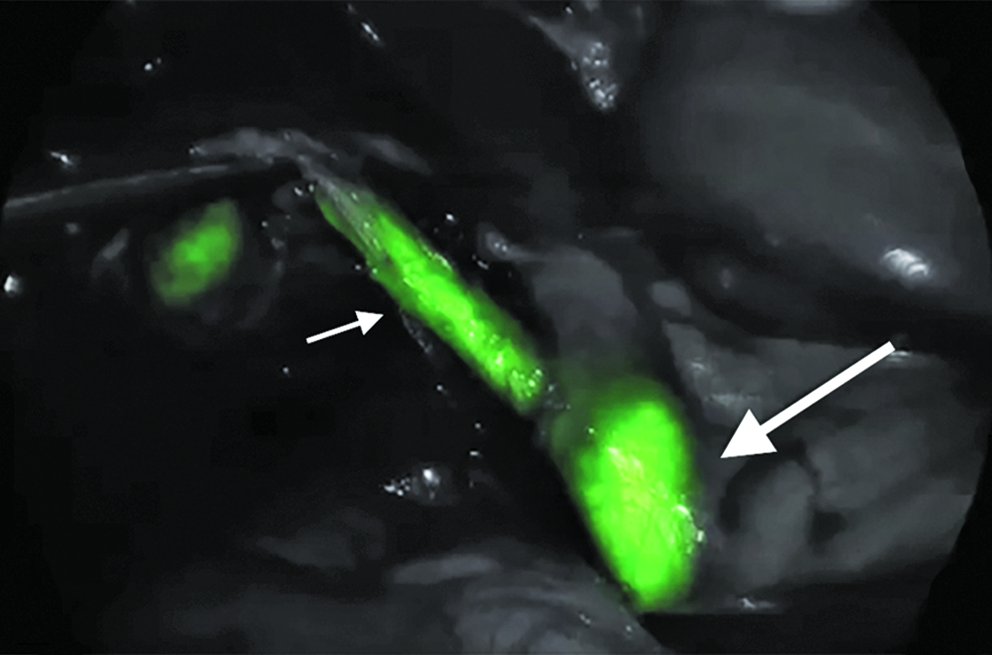
ICG fluorescence of the cystic duct (small arrow), leading into the common bile duct (large arrow), is shown. ICG, indocyanine green.
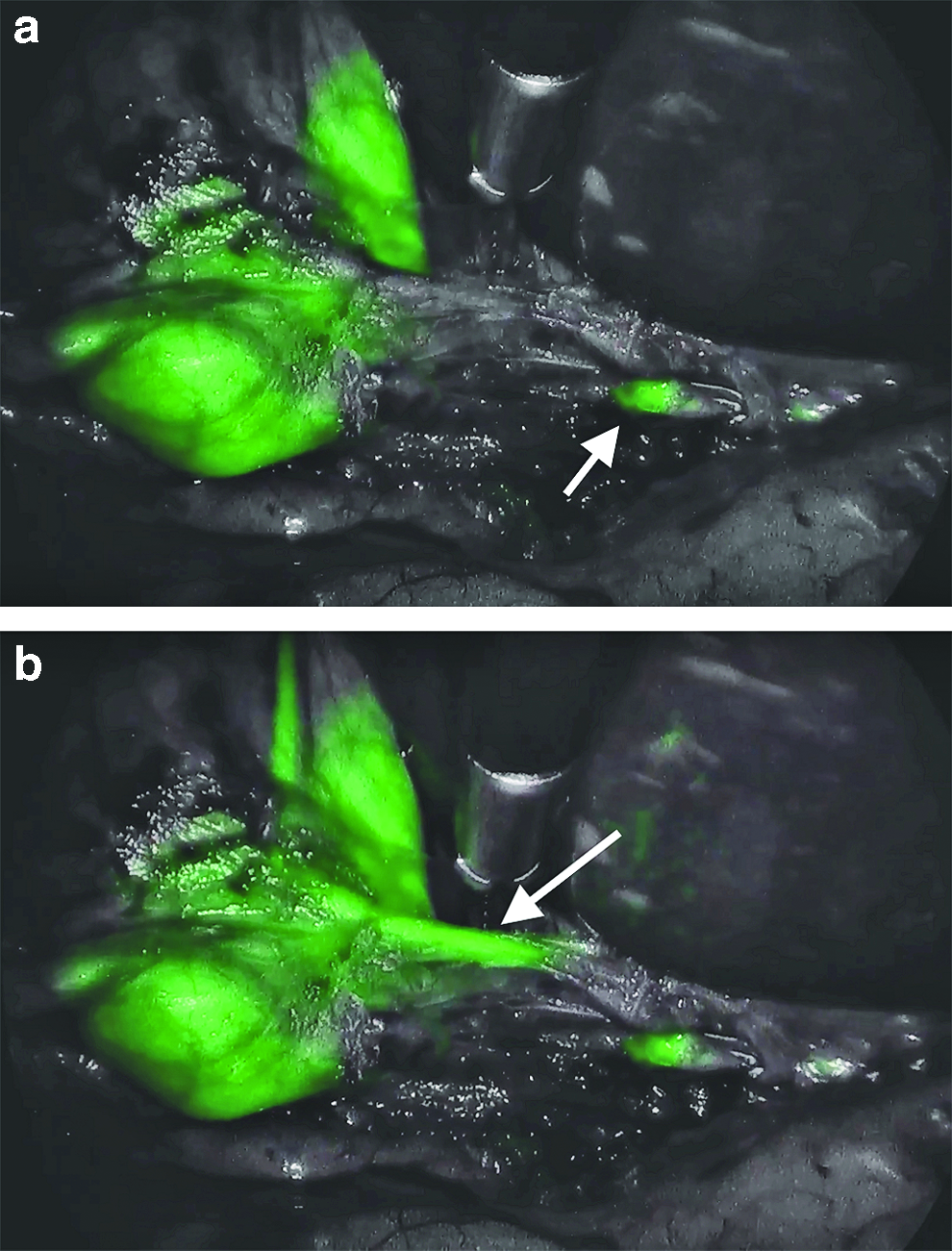
Dissection of the gallbladder from the liver bed using cautery was done under NIR mode. The fluorescence of the gallbladder aided in differentiating the boundary layer between the gallbladder and the liver (Fig. 3).

The fluorescent gallbladder, in contrast to the dark liver, accentuates the plane of dissection of the gallbladder fossa.
Discussion
ICG was originally developed for use in photography by Kodak Research Laboratories in 1955 and subsequently approved for clinical use in 1956. The dye is nontoxic and nonionizing, and it has no known metabolites. When injected intravascularly, it rapidly binds to plasma proteins, keeping the molecule within the vasculature until it is quickly and entirely extracted by the liver and excreted into the bile.17,18 Of note, ICG is manufactured with a small amount of iodine premixed to aid in water dissolution. Although adverse reactions to ICG given intravenously are very rare, at ∼0.003%,15,19 patients should be asked about iodine allergy before use, and premedication should be considered in patients with a previous iodine reaction, since iodine can be absorbed through the biliary tract membrane.
The confinement of ICG to the vasculature, as well as its high optical absorbance at wavelengths wherein most human tissues are translucent (∼800 nm), makes the dye particularly useful for angiography and the assessment of tissue perfusion. Its many medical applications include ophthalmic angiography, intraoperative neurosurgical and coronary angiography, reconstructive microsurgery, prediction of wound healing after amputation, and lymphatic mapping. 17 Moreover, because of the dye's complete excretion into the bile, ICG is also the ideal dye for visualization of the extrahepatic biliary tree. 20 However, timing of IV administration can be difficult to optimize, as background signal from the liver can impede visualization if ICG is injected too close to time of dissection. 16 If an additional injection is required, the surgeon must wait for bile excretion, which can add time to the procedure.
We describe a novel use of ICG injected directly into the gallbladder to visualize biliary anatomy. Although previously performed in a porcine model, 21 to our knowledge, this has never before been performed in humans. The direct injection into the extrahepatic biliary system eliminates the delay associated with IV injection, allowing for immediate fluorescence. Moreover, the liver and blood vessels are excluded, highlighting only the extrahepatic biliary system, and thereby improving visual contrast. This technique of fluorescent cholangiography, therefore, serves a similar purpose to traditional intraoperative contrast X-ray cholangiography. However, it provides several advantages: it avoids the use of radiation, allows for real-time visualization during dissection, and can be performed entirely by the surgeon without additional staff. Although special equipment is required, this equipment is easily integrated into a traditional laparoscopy tower. One important caveat is that fluorescent cholangiography has not been shown to effectively identify common bile duct stones. 15 Therefore, it should not replace traditional contrast X-ray cholangiography in cases with concern for common bile duct obstruction.
The concentration of ICG in solution affects its fluorescence. At high concentrations, quenching (decrease in fluorescence due to light absorption) occurs, due to aggregation of the dye molecules.20,22 When ICG is injected intravascularly, it rapidly binds to plasma proteins, which separate the molecules, decreasing the quenching effect. 23 When using ICG to visualize blood vessels, extraction by the liver also maintains brightness, because, although the dye is cleared, the dequenching effect from dilution keeps fluorescence intensity relatively stable. 24 Because our technique confines the ICG to the biliary system, to avoid the quenching effect, a dilute solution of ICG should be used when injecting directly into the gallbladder. Studies suggest an ICG solution of ∼0.025 mg/mL is ideal for biliary imaging.25,26 We describe our three-step dilution procedure above. While mistakes in the dilution process would not be harmful to the patient, more or less concentrated ICG solutions would not fluoresce as brightly, and NIR visualization may be suboptimal.
During dissection of triangle of Calot, standard light and NIR light modes are toggled back and forth to take advantage of both modes of visualization. Fluorescence of the cystic duct and common bile duct gives an extra level of comfort to the surgeon dissecting the critical view of safety, especially in the face of inflammation or aberrant anatomy. The cystic artery is not illuminated with our method of direct gallbladder injection, but the contrast between it and the fluorescent gallbladder is useful to define the path of the artery along the gallbladder wall (Fig. 4). If further definition of the cystic artery is desired after the cystic duct has been isolated, a fluorescent view of the cystic artery can be obtained with an IV bolus dose (2.5 mg) of ICG, administered by the anesthesiologist. The triangle of Calot must be carefully monitored with the NIR camera, as the cystic artery will transiently fluoresce ∼15 seconds after IV injection of the ICG bolus (Fig. 5).

The path of the cystic artery (dark) can be easily visualized coursing along the surface of the fluorescent gallbladder.
Fluorescence of the cystic artery can be obtained with an intravenous (IV) bolus of ICG.
ICG fluorescence also greatly improves visualization of the plane between the gallbladder and the liver bed, as the gallbladder is dissected free. A particular advantage of this technique is the ability to quickly identify any accessory bile ducts arising from the gallbladder fossa, which can be missed with a standard light view.
Whenever a new method is introduced, the cost of the implementation becomes a consideration. Fortunately, the cost of ICG is low; one powdered vial of ICG costs $25. According to Stryker Corporation, the cost of their NIR tower system is comparable to their current high-definition non-NIR system. The NIR tower system can also be used in a regular non-NIR mode.
In conclusion, we present a modification of fluorescent cholangiography using direct gallbladder ICG injection to improve visualization during laparoscopic cholecystectomy.
Direct gallbladder injection provides two important advantages compared to intravascular injection: it provides immediate visualization of extrahepatic biliary structures upon injection and clarifies the dissection plane between the gallbladder and the liver bed. By improving visualization of biliary anatomy, we minimize bile duct injury without compromising surgical efficiency.
Footnotes
Disclosure Statement
No competing financial interests exist.