
Abstract
Abstract
Background:
Hybrid liver resection is considered a modality of minimally invasive surgery; however, there are doubts regarding loss of benefits of laparoscopy due to the use of an auxiliary incision. We compared perioperative results of patients undergoing hybrid × open and hybrid × pure laparoscopic resections.
Methods:
Consecutive patients undergoing liver resection between June 2008 and January 2016 were studied. Study groups were compared after propensity score matching (PSM).
Results:
Six hundred forty-four resections were included in the comparative analysis: 470 open, 120 pure laparoscopic, and 54 hybrids. After PSM, 54 patients were included in each group. Hybrid × open: hybrid technique had shorter operative time (319.5 ± 108.6 × 376.2 ± 155.8 minutes, P = .033), shorter hospital stay (6.0 ± 2.7 × 8.1 ± 5.6 days, P = .001), and lower morbidity (18.5% × 40.7%, P = .003). Hybrid × pure laparoscopic: hybrid group had lower conversion rate (0% × 13%, P = .013). There was no difference regarding estimated blood loss, transfusion rate, hospital stay, complications, or mortality.
Conclusions:
Hybrid resection has better perioperative results than the open approach and is similar to pure laparoscopy. The hybrid technique should be considered a minimally invasive approach.
Introduction
L
In 2008, the first international consensus on LLR standardized technical aspects and nomenclature related to the three preferred methods of performing minimally invasive liver surgery, dividing them into pure laparoscopic liver resections (PLLR), hand-assisted liver resections (HALR), and hybrid liver (laparoscopy-assisted) resections. 3 Initial experience with LLR occurred with the pure laparoscopic approach, which is the preferred method in most centers.1,4,5 The best candidates for PLLR are patients with lesions in anterolateral liver segments (2, 3, 4b, 5, and 6), also known as “laparoscopic segments.”1,3,6 Currently, minor resections in these segments and left lateral sectionectomy are considered the gold standard practice in specialized centers.6,7
Despite the increasing experience in PLLR, there are some limitations to its diffusion, such as elevated costs, high surgical skills requirement, and long learning curve.2,8 Laparoscopy implies in a bidimensional caudal view, limitation of movements and difficult access to posterior and superior liver segments.9,10 Therefore, posterosuperior or central resections (segments 1, 4a, 7, and 8), multiple bilateral resections, and major hepatectomies (≥3 segments) are still a challenge, even in specialized centers.11–13
The hybrid technique emerged to overcome some of the limitations faced by the PLLR and, therefore, increases the indications and safety of LLR.3,14 It restores tactile sensation, being useful for identifying small lesions and for hemostatic parenchymal or hilar compression during liver transection. 15
Hybrid resections are initiated in a totally laparoscopic manner or even hand assisted. Full liver mobilization is accomplished, followed by a planned minilaparotomy for a conventional approach to vascular pedicles (if necessary) and parenchymal transection. 3 The similarity to open surgery may reduce the learning curve,12,15,16 and it may serve as a “training platform” for carrying out more complex PLLR.6,17 Moreover, the laparoscopy-assisted approach can be used for any type of hepatectomy, including complex resections and operations in which safety is crucial, such as resections in the posterosuperior segments and major hepatectomies, especially in living donor liver harvesting.7,10,11,18
The consensual classification of the hybrid technique as a modality of LLR seemed arbitrary at a time when there were no scientific data to support such classification. Even so, the hybrid technique is considered a modality of LLR, in the paucity of data demonstrating the benefits of hybrid resections compared with OLR.15,16,19 Similarly, a few studies have compared the results of the hybrid technique with other LLR techniques.20,21
The question that must be answered is whether the hybrid technique is as safe as OLR and, second, whether it improves patients' outcomes.
The aim of this study was to compare the perioperative results of patients undergoing hybrid resection with the results of patients undergoing OLR (primary endpoint). In addition, we compared the results of patients undergoing hybrid resection with the results of those undergoing PLLR (secondary endpoint).
Materials and Methods
From a prospective database, consecutive patients ≥18 years old who were submitted to liver resection between June 2008 and January 2016 were evaluated. The Institutional Research Ethics Committee approved this protocol. This study was conducted by following Strengthening the Reporting of Observational studies in Epidemiology (STROBE) recommendations. 22
Patients who were submitted to two-stage hepatectomy, and patients with hilar cholangiocarcinoma were excluded. We also excluded patients undergoing HALR and patients with incomplete data. After exclusion criteria, the remaining patients included in comparative analyses were matched by using a propensity score matching (PSM) to overcome selection bias.
Liver resections were defined according to Brisbane 2000 terminology. Minor hepatectomy was defined as resection of <2 segments, and major hepatectomy was defined as resection ≥3 segments. Laparoscopic resections of lesions located in posterosuperior segments of the liver were called “difficult resections.” 6
Postoperative morbidity was defined as any event occurring during the first 90 postoperative days and was stratified according to the Dindo-Clavien classification. 23 Postoperative biliary fistula was defined by following the criteria proposed by the International Study Group of Liver Surgery. 24 Postoperative mortality was defined as death within 90 days after liver resection.
All patients underwent pre-operative clinical evaluation with laboratory tests and image evaluation (ultrasonography, computer tomography, and magnetic resonance as needed). Patients were classified according to the American Society of Anesthesiologists (ASA) physical status score. The indication of the surgical procedure was carried out after discussion in a weekly multidisciplinary meeting.
The following preoperative characteristics were studied: age, gender, body mass index (BMI), previous medical history, ASA classification, preoperative diagnosis, size and location of the lesions, previous abdominal surgeries, presence of chronic liver disease, and portal hypertension. Regarding intra- and postoperative data: Type of procedure, operative time, estimated blood loss, transfusion requirement, conversion rate, length of intensive care unit (ICU) stay and length of hospital stay, postoperative complications, and mortality were evaluated.
Surgical procedures
OLR was defined as those performed through incisions as follows: J-shape incision, “Chevron” or “Mercedes” incision. In PLLR, the entire procedure was performed by laparoscopy and an incision was performed only for specimen retrieval. Hybrid resections were defined as procedures through which liver mobilization (with or without dissection of vascular pedicles or hepatic veins) was performed through a totally laparoscopic or hand-assisted approach, followed by elective minilaparotomy (8–15 cm) for pedicle and/or hepatic veins dissection and parenchymal transection (Fig. 1). Non-planned auxiliary incision for intraoperative complications (i.e., bleeding) or extension beyond 15 cm was considered conversion to open surgery.
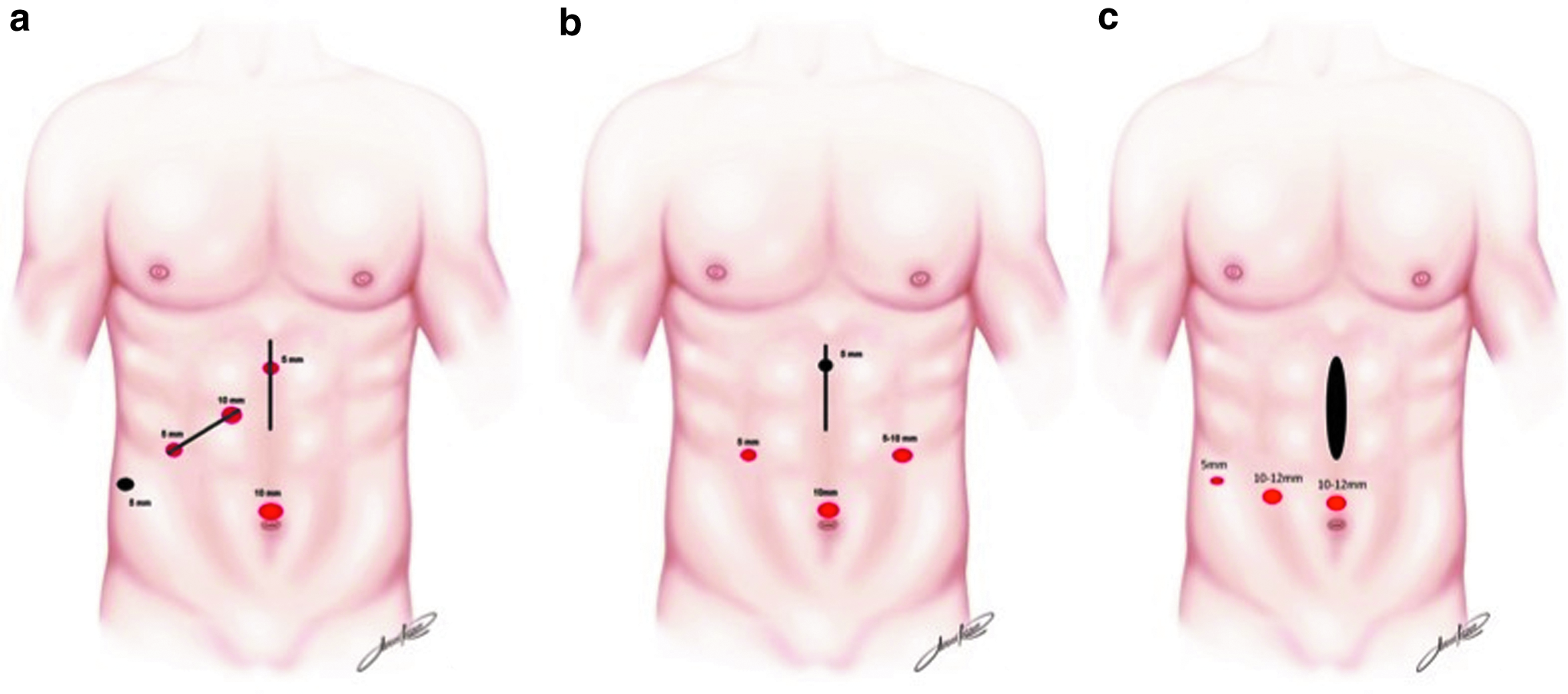
Port placement illustration for hybrid resections.
We preferably used the hybrid technique in lesions located in posterosuperior segments of the liver (“difficult resections”) and selected cases of bilobar disease. For standard major hepatectomies (right and left), the pure laparoscopic technique was preferred, with hybrid operations being applied in cases where a straightforward resection cannot be performed.
Statistical analysis
Continuous data were expressed as median and interquartile range or mean and standard deviation. T test was used when the distribution was normal (verified by Anderson Darling test). When data were not normally distributed, Mann-Whitney test (equal variances) or Brunner-Munzel T test (different variances) was used. Categorical variables were expressed as percentage and compared by using Fisher or Chi-square tests. Statistical analyses were done by using R program 3.1.2 (Foundation for Statistical Computing, Vienna, Austria). A P value <.05 was considered statistically significant.
PSM was used to avoid possible selection bias, as it overcomes the different distribution of covariates among individuals who are allocated to specific interventions in the study. The propensity score model was estimated by using logistic regression, including all potential covariates that could affect the group allocation. We included all the laboratory tests, epidemiologic, tumor, and surgical characteristics. After multivariate logistic regression, two models were obtained: a model with two variables (type of hepatectomy [major versus minor] and presence of cirrhosis) and a model with one variable (type of hepatectomy [major versus minor]). Using the Akaike information criterion, 25 the model with two variables showed the best performance for hybrid × OLR comparison and the model with one variable was the best for hybrid × PLLR comparison. After this step, a 1:1 “nearest neighbor” match was used for each comparison. Then, the two matched groups were compared with respect to the study endpoints.
Results
During the study period, 735 consecutive liver resections were performed in 668 patients; LLR techniques were employed in 189 patients (25.7%). After applying the exclusion criteria, 644 liver resections (in 630 patients) were included in comparative analysis: 470 OLR, 120 PLLR, and 54 hybrids. After matching by PSM, 54 patients were included in each group.
Hybrid × OLR
In patients undergoing hybrid resection, the procedure was initiated by the totally laparoscopic technique in 51 (96.3%) patients and by hand assistance in 3 patients (5.6%). Midline auxiliary incision was used in 36 patients (66.7%), and right subcostal incision was used in 19 patients (33.3%). The median size of the incision was 10.5 cm (8–15 cm). There was no conversion in the group undergoing hybrid surgery.
Pathologic diagnoses of patients included in the hybrid group were as follows: colorectal liver metastases (CRLM) (N = 22, 40.7%), hepatocellular carcinoma (HCC) (N = 17, 31.5%), hepatocellular adenoma (n = 5, 9.3%), intrahepatic cholangiocarcinoma (N = 3, 5.6%), cystic mucinous neoplasm (N = 2, 3.7%), neuroendocrine tumor metastases (N = 1, 1.9%), other metastases (N = 1, 1.9%), and other diagnoses (N = 3, 5.6%). In the OLR group, diagnoses were as follows: CRLM (N = 24, 44.5%), HCC (N = 21, 38.9%), neuroendocrine tumor metastases (N = 2, 3.7%), other tumor metastases (N = 2, 3.7%), intrahepatic cholangiocarcinoma (N = 2, 3.7%), hepatocellular adenoma (N = 1, 1.9%), and other diagnoses (N = 2, 3.7%).
Baseline characteristics of patients in both groups after PSM are shown in Table 1. There were no significant differences in epidemiologic, clinical, and surgical characteristics between the two groups.
ASA, American Society of Anesthesiologists; BMI, body mass index; INR, international normalized ratio; OLR, open liver resection; SD, standard deviation.
Perioperative results of patients who underwent hybrid and OLR are shown in Table 2. There was no statistical difference between both groups in estimated blood loss, transfusion rate, and ICU stay. The hybrid group showed shorter operative time (319.5 ± 108.6 minutes versus 376.2 ± 139.3 minutes, P = .033) and shorter length of hospital stay, with an average decrease of 2.1 days (6.0 ± 2.7 days versus 8.1 ± 5.6 days, P = .012).
A maximum of 90 days.
Dindo-Clavien III–V.
ICU, intensive care unit; OLR, open liver resection; SD, standard deviation.
Regarding postoperative morbidity, hybrid resection showed a lower rate of complications (18.5% versus 40.7%, P = .003). Major complications (5.6% versus 13%, P = .32), minor complications (13% versus 27.8%, P = .09), biliary complications (1.9% versus 5.6%, P = .617), and wound-related complications (1.9% versus 3.7%, P = 1) were more common in the OLR group; however, the individual analysis did not reach statistical significance. Perioperative mortality was similar between groups (1.9% versus 3.7%, P = 1.0).
There was no significant difference in the clearance of surgical margins between techniques (98% versus 84.4%, P = .059), and the hybrid group showed larger resection margins than the OLR group (9 mm [4–14.5] versus 3 mm [2–8.7], P = .002).
Hybrid × PLLR
Seven (13%) patients who underwent PLLR required conversion to open surgery: 5 cases due to bleeding and 2 due to technical difficulty. Surgical indications of patients included in the PLLR group were as follows: CRLM (N = 15, 27.8%), HCC (N = 13, 24.1%), hepatocellular adenoma (N = 14, 25.9%), intrahepatic lithiasis (N = 1, 1.8%), cystic mucinous neoplasm (N = 2, 3.7%), other tumor metastases (N = 2, 1.7%), and other diagnoses (N = 6, 11.1%).
After PSM, both groups were matched in terms of age, sex, BMI, malignant and benign indications, proportion of chronic liver disease, and number of nodules resected (Table 3). There was a significant difference in the size of the largest nodule (36.8 ± 26.3 mm versus 50.3 ± 32.3 mm, P = .036). Other clinical and laboratory characteristics were similar, except for higher serum albumin level in the PLLR group, although both groups had values within normal range. There was a similar proportion of major resections between groups; however, the hybrid technique was employed more frequently for lesions located in posterosuperior segments (47.9% versus 20%, P = .007) (Table 3).
Values shown in bold denote statistical significance.
ASA, American Society of Anesthesiologists; BMI, body mass index; INR, international normalized ratio; OLR, open liver resection; PLLR, pure laparoscopic liver resection; SD, standard deviation.
Perioperative results of patients who underwent hybrid and PLLR are shown in Table 4. Conversion rate was lower in the hybrid group (0% versus 13%, P = .013). Estimated blood loss, blood transfusion rate, and operative time were similar between groups. There was no difference in the length of ICU (1.8 ± 1.3 days versus 1.8 ± 1.1 days, P = .991) or hospital stay (6.0 ± 2.7 days versus 6.1 ± 3.6 days, P = .366).
Values shown in bold denote statistical significance.
A maximum of 90 days.
Dindo-Clavien III–V.
ICU, intensive care unit; PLLR, pure laparoscopic liver resection; SD, standard deviation.
Postoperative morbidity (18.5% versus 24.1%, P = .64), major complications, wound-related complications, and biliary complications were similar between groups. There was no significant difference regarding R0 resections (98% versus 93.5%, P = .342) or width of resection margins (9 mm [4–14.5] versus 7 mm [3–14], P = .313).
Discussion
Since the first LLR for peripheral lesions reported by Reich et al., 26 great advancements occurred, and anatomical resections and, subsequently, more complex resections were described as feasible and safe.27–29 The pure laparoscopic approach was the initial and preferred method in most centers. By the year 2008, 75.1% of the published cases were PLLR, 16.5% were HALR, and 2.1% were hybrid. 4
The long learning curve associated to LLR might be reflected by a slow diffusion of minimally invasive liver techniques. Vigano et al. 2 published a seminal paper on the subject and concluded that 60 cases were needed to achieve optimal results. For major liver resections, the learning curve included 45 to 75 patients.8,30
As a technically demanding operation, difficulties can occur any time during PLLR. A risk-bearing step is parenchymal transection, which is responsible for most of the blood loss. Importantly, intraoperative hemorrhage represents the most frequent cause of conversion.4,6 As cited earlier, the location of tumors (central or posterosuperior segments) and the extent of resection (major hepatectomies) are also complex resections in which PLLR may have limited applicability. Limitations of LLR were depicted in a recent survey including 27 specialized centers with 11.712 liver resections showing that 32.1% were performed laparoscopically. The minimally invasive approach was used in 61.8% of left lateral sectionectomies; however, for major hepatic resections, this percentage fell to 24.8%. 31
In this context, other modalities of LLR such as the hybrid technique have been performed to overcome limitations of the totally laparoscopic approach and, thus, expand the access and increase the safety of LLR. 14
The first laparoscopic-assisted resections were reported by Huscher et al., 32 in particular for major resections as right hepatectomies. This technique joins the benefits of laparoscopy for liver mobilization with the safety of OLR. Large incisions are avoided and high-risk operative steps, such as parenchymal transection, are safely performed.10,14 Closest to the conventional method, hybrid hepatectomy requires a smaller learning curve and can be used by surgeons with less experience in laparoscopic surgery.15,17
The hybrid technique can be used for any type of liver resection; however, our understanding is that this approach is best indicated when the surgeon foresees difficulty to localizing or resecting lesions, that is, those located in the segments of difficult laparoscopic access, multiple bilateral resections, and on major hepatectomies. In a recent study published by our group with the laparoscopy-assisted technique, these conditions were present in 66.7% of patients. 10 Currently, we preferably use the hybrid technique in “difficult resections” and selected cases of bilobar disease. For standard major hepatectomies (right and left), the pure laparoscopic technique is preferred, with hybrid operations being applied in cases where a straightforward resection cannot be performed. 6
In 2014, a multicentric study with 1.184 major LLR reported that the hybrid or HALR was used in 19.1% of right hepatectomies and 16.1% of left hepatectomies. 33 A systematic review comparing PLLR, HALR, and hybrid for major resections showed that hybrid has its best applicability in the resection of lesions in difficult locations, patients scheduled to technical difficulties, and resections that require delicate hilar dissection, such as living-donor hepatectomy. 11
The hybrid technique is used more often in Eastern centers, especially in Japan. Soyama et al. 34 reported that the hybrid technique was used in 47% of LLR performed between 2009 and 2012 at the University of Nagasaki. Recent national surveys, including 124 Japanese centers (2.259 patients), showed that 32.7% of all laparoscopic resections were performed by the laparoscopy-assisted technique. 35 Nitta et al. 36 observed that 88.7% of major hepatectomies were performed through the hybrid technique in specialized Japanese centers, 7.5% in PLLR, and 3.8% in HALR.
Despite being considered a modality of LLR, few studies regarding the benefits of the hybrid technique over OLR were published. The main advantage over the open approach is the use of smaller incisions, avoiding extensive abdominal wall neuromuscular transection. 15 However, some authors point out the following potential disadvantages: inadequate liver exposure through the auxiliary small incision, longer operative time, and a potential loss of the benefits of the laparoscopic approach.10,15,34 In a systematic review of comparative studies between hybrid, HALR, and OLR, Hasegawa et al. 37 showed no evidence of superiority of any of these different techniques. The present study is the first to address the results of the hybrid technique, in comparison to the open and PLLR in well-matched groups employing PSM.
Hybrid versus OLR
A few comparative studies regarding hybrid versus OLR were published. Our data indicate shorter operative time, with a mean reduction of 19.5% in the hybrid group, as opposed to other reports.16,34,38 This finding might be explained by our large experience with laparoscopic liver mobilization when compared with other groups that employed and reported their results with the hybrid technique in their early experience with LLR. The choice of the auxiliary incision is also an important aspect for technical success and decrease in operative time. Right subcostal incision is an option for right posterior sector lesions; however, some authors reported good results through a midline approach in these situations.14,34 The midline incision is the auxiliary incision of choice for left-sided and bilateral disease since it allows access to all liver segments.10,14
We did not find a significant difference in estimated blood loss or transfusion rate between studied groups, in accordance to previously published data.16,19,38
We showed a shorter length of hospital stay in the hybrid group, with a mean reduction of 25.9% (6.0 ± 2.7 days versus 8.1 ± 5.6 days, P = .012). This finding has been repeatedly reported and should be interpreted as a consequence of fewer postoperative complications, faster return of bowel movements, and less postoperative pain.16,21,38
Postoperative complications were reported in 3.4% to 30% of patients who underwent hybrid resections.10,12,16,17,19,34 In our series, postoperative morbidity was 18.5%, which was significantly lower than the open group (40.7%). Major complications occurred in 3 patients (5.6%), which was not significantly different from the OLR group (3.7%). Most comparative studies showed similar postoperative morbidity in both groups, and none reported a higher morbidity in the hybrid group.16,17,38 Regarding wound and biliary complications, our results are in accordance with available comparative data.19,21,38
The two initial queries on this study can be answered from the current data: The hybrid technique does not compromise the safety and feasibility of liver resections when compared with the open approach, and it improves outcomes by reducing the length of stay and the incidence of postoperative complications.
Hybrid versus PLLR
A comparison between hybrid and PLLR is impaired due to the paucity of available studies.21,39 Conversion rates reported for the laparoscopy-assisted technique varied between 0% and 10%.15,17,20 In our series, we observed a lower conversion rate in the hybrid group (0% versus 13%, P = .013). In fact, there is no clear definition of conversion for the hybrid method. A well-accepted definition is a non-elective auxiliary laparotomy that is performed due to intraoperative complications, such as bleeding.3,7 There is no universally accepted maximal length of the minilaparotomy. Some groups, especially in Japan, set the limits between 8 and 12 cm14 whereas others used 15 cm as the maximal length of the incision. 40 In our study, auxiliary incisions larger than 15 cm were considered as conversion.
Koffron et al. 17 compared PLLR versus HALR versus hybrid versus OLR and showed that the hybrid technique had similar results of other LLR modalities, except for a longer operative time. In our study, while comparing PLLR and hybrid groups, we were not able to show any difference regarding operative time, blood loss, transfusion rate, and length of hospital stay. In summary, our study and other comparative studies found that PLLR and hybrid have similar results.20,21,39 Therefore, it should be considered an LLR modality with real benefits over OLR.
Our study was designed to minimize bias, and to overcome its retrospective character. Selection bias was reduced, excluding cases in which the open approach is typically employed, such as two-stage liver resections and hilar cholangiocarcinoma. We believe that the use of PSM equalized groups strengthened our data. Therefore, the evidence from this article is one of the best available since randomized clinical trials were not performed.
In conclusion, the hybrid technique is feasible, safe and has better perioperative results than the open approach. When compared with PLLR, hybrid resections show similar perioperative results. Our data show that the hybrid approach does not lead to loss of benefits of laparoscopy and is a consistent modality of minimally invasive liver surgery.
Footnotes
Disclosure Statement
No competing financial interests exist.