
Abstract
Abstract
Introduction:
Recurrence of achalasia may occur in 10%–20% of cases operated by Heller's cardiomyotomy. Most of these patients will require further surgery to relieve symptoms. Major technical difficulties can be found in these reoperations.
Case Report:
A 50-year-old female patient with relapsed idiopathic achalasia after Heller's technique was treated with an unusual procedure, for the first time in the literature, by minimally invasive access with robotic assistance.
Conclusions:
The Serra-Doria operation allows preserving the esophagus and alleviating dysphagic symptoms with low rates of postoperative complications. The use of robotic technology is perfectly feasible and allows minimally invasive access in complex cases and reoperations.
Introduction
A
The diagnosis is usually made between 25 and 60 years of age. The predominant symptom is dysphagia, which is reported as being of long duration, improving with ingestion of liquids or maneuvers that increase the intraesophageal pressure. Thus the symptoms are mitigated with position adjustments such as lifting head and shoulder, decreasing food intake, and with the help of liquids for swallowing. As complementary examinations, a barium radiograph (upper GI) constitutes the main diagnostic examination. The upper endoscopy (UE) is performed to avoid an associated neoplasm. Upper GI reveals narrowing of the distal portion of the esophagus (LES) and upstream dilatation and spastic contractions (tertiary waves). 3
Patients usually present themselves emaciated due to chronic difficulty of food intake. The treatment aims to relieve dysphagia, since it is not possible to restore the autonomic innervation of the esophagus. All therapeutic, medicinal (nitrate and calcium channel blocker), endoscopic, or surgical methods aim to abolish achalasia. With the exception of the surgical treatment, none of them is considered ultimate, with recurrence of dysphagia in a few months or years. The type of surgical intervention is usually indicated according to the amount of esophagus dilation. The most common procedure is the Heller operation with Dor fundoplication. 1
When it comes to megaesophagus with a dolicomegaesophagus (very dilated esophagus lying on the diaphragm) or a relapse of symptoms after Heller's operation, reoperations are more complex to be accomplished. Options are esophagectomy with gastroplasty or jejunal interposition. In Brazil, due to the large number of patients with advanced megaesophagus, the frequent failure of conservative treatment and to avoid esophagectomy, the Serra-Doria operation was proposed in 1970. This technique consists in Grondhal cardioplasty (latero–lateral [LL] esophagogastrostomy between the lower esophagus in the last 6 cm above the cardia and gastric fundus close to the Hiss angle) associated to partial gastrectomy with Roux-en-Y gastrojejunal reconstruction. 4
The objective of this report is to describe, for the first time in literature, the application of this technique through a robotic minimally invasive access for the treatment of recurrent achalasia after Heller's cardiomyotomy.
Case Report
This report is about a 50-year-old female with dysphagia for solid food in the past 5 years. Twenty years ago the symptoms started, with progressive worsening over the years. During diagnostic investigation, idiopathic megaesophagus was evidenced. She underwent clinical treatment without improvement, and UE was performed with cardia dilatation by pneumatic balloon. However, the patient reported little improvement after this procedure. For a few years, she still related dysphagia, but for the past 9 years the symptoms got worse, referring dysphagia for fluids. At this moment, surgery was indicated and a Heller's cardiomyotomy performed without fundoplication. Although the patient presented momentary improvement of the symptoms after the operation, dysphagia recurred 5 years after this surgical procedure.
In this new diagnostic investigation, an upper GI was performed, which showed esophageal dilatation with tortuosity of the esophagus (Fig. 1). UE showed enlargement of esophagus caliber, food stasis, and distal esophagitis. Esophageal electromanometry revealed hypertonia of the LES associated with hypocontractility and aperistalsis of the esophageal body (Fig. 2). Considering the relapse of achalasia after Heller's cardiomyotomy, a new surgical treatment was indicated, such as robotic Serra-Doria operation.

Upper GI showing narrowing of the distal esophagus with upstream dilatation and tortuosity.
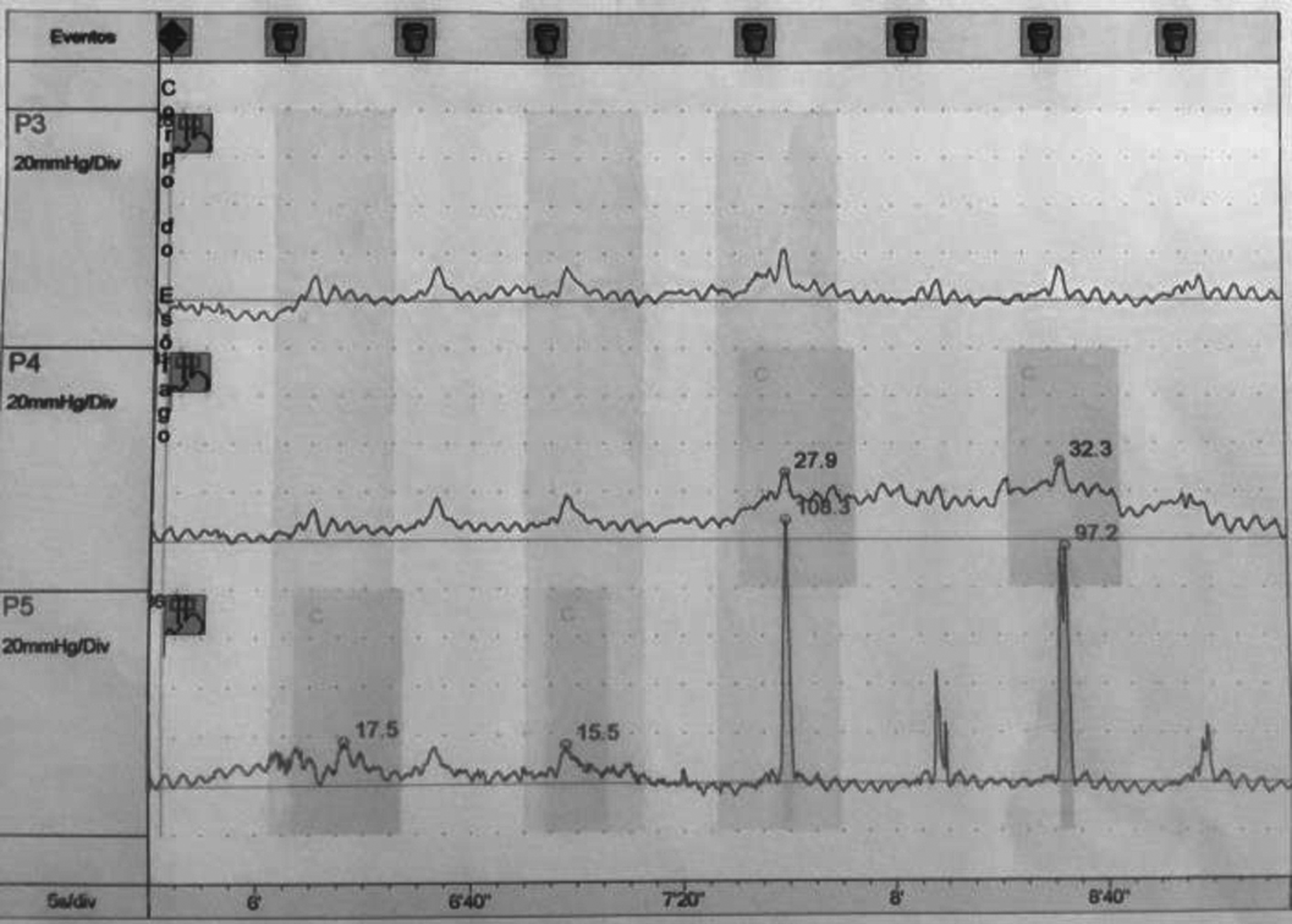
Electromanometry showing hypocontractility and aperistalsis of the esophageal body.
Description of the Technique
The patient was placed in the dorsal recumbent position under general anesthesia. Six portals were used according to Figure 3.
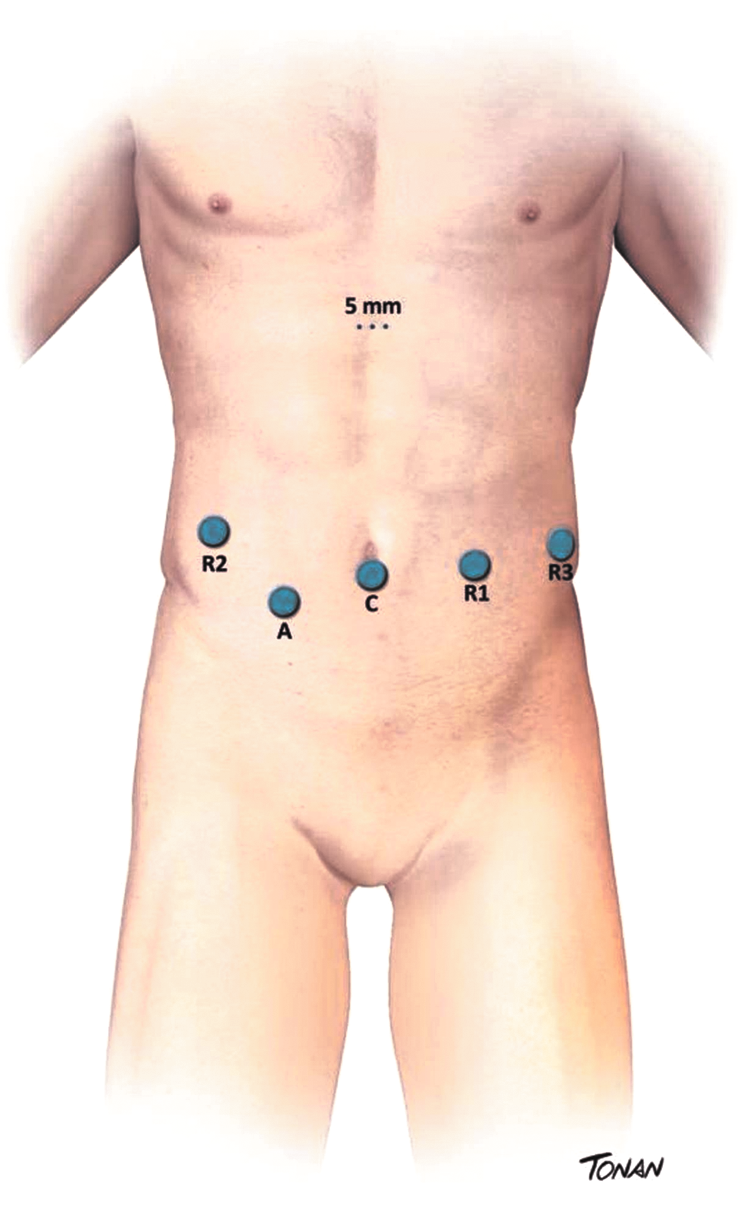
Trocar placement.
The procedure began with the dissection of the esophagogastric transition and release of the adhesions of the previous surgery. The lower esophagus was then released and drawn with a Penrose drain. This traction conditioned the apposition of the gastric fundus to the inferior esophagus. A small opening was made at the level of the esophagogastric junction for the introduction of the 60 mm endostapler with blue cartridge for mechanical LL anastomosis between the distal esophagus and the gastric fundus (Fig. 4). The stapler defect was sealed with manual suture assisted by the robot with a 3-0 PDS in a single layer. Partial gastrectomy was then performed with dissection of the stomach inside the vascular arcade, which was greatly facilitated by the application of the robot. After dissection of the gastric antrum, the duodenum was sectioned just below the pylorus and the gastric antrum above the incisura angularis, completing the subtotal gastrectomy. The reconstruction of the digestive tract was done by transmesocolic route, in Roux-en-Y, preserving a biliary loop of about 30 cm from Treitz's angle and feeding loop with 70 cm of length. The gastrojejunal and jejunojejunal anastomosis were performed mechanically with 60 mm blue cartridges, and the stapler defect were sutured manually with 3-0 PDS. The final aspect of the procedure is demonstrated in Figure 5. The abdomen was drained with silastic drain.
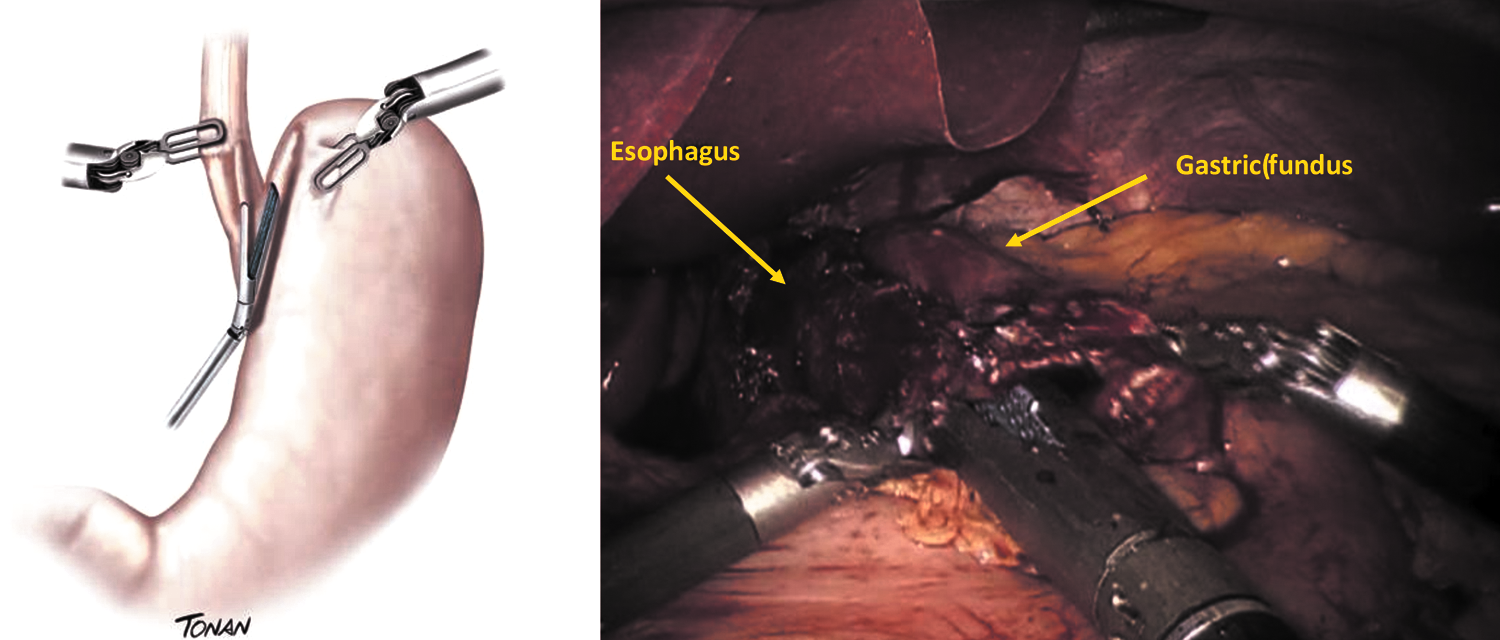
Grondhal's cardioplasty (latero–lateral esophagogastrostomy between the lower esophagus and gastric fundus).
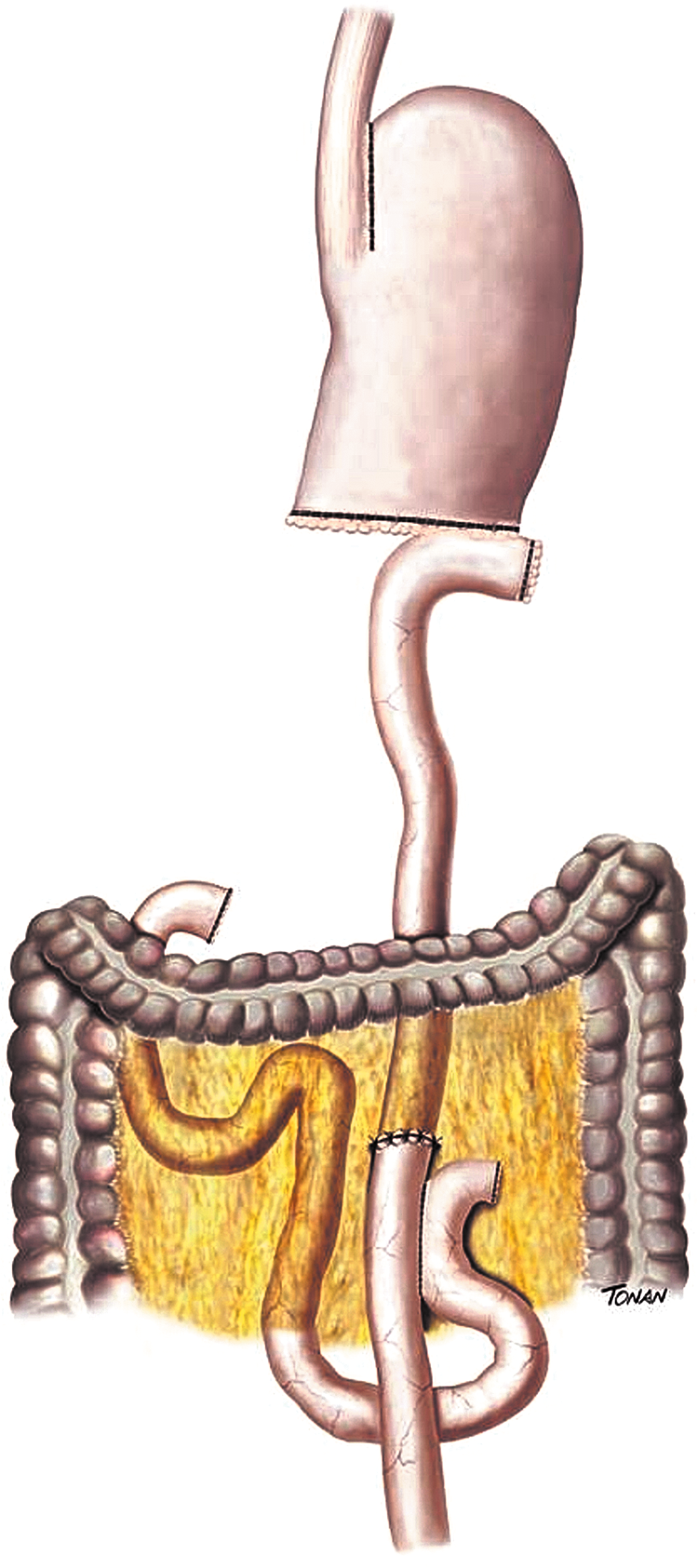
Final aspect of Serra-Doria technique.
The procedure was performed completely robotically. The operative time was 220 minutes, and the surgery was uneventful. There was no significant bleeding.
Oral feeding was initiated on the first postoperative day (PO) with good acceptance of the liquid diet and evolution to a subsequent pasty diet, with good acceptance.
An upper GI performed in the third PO showed a significant improvement in the esophageal emptying time (Fig. 6). Patient was discharged without complications in the fourth PO, receiving pasty diet and without dysphagia. The follow-up time is 13 months and the patient remains symptom-free.

Postoperative upper GI showing improvement on the esophageal emptying.
Discussion
Due to the low morbidity and mortality rates and the great improvement in the relief of symptoms, laparoscopic Heller's cardiomyotomy is the surgical treatment of choice for achalasia. However, over time, recurrence of dysphagia can occur between 10%–20% of cases. 1 The cause of recurrence of the symptoms may not be easy to identify, but among the main ones, we can mention the healing of the distal border of the myotomy, failure of the operative technique, gastroesophageal reflux, and esophageal cancer. 5
Most patients with dysphagia will require reintervention, done whether by endoscopic dilatation or surgical reoperation. Zaninotto et al. reported a 78% efficacy in relieving symptoms with endoscopic pneumatic dilatation (median two sessions) in patients with recurrent achalasia after Heller cardiomyotomy. 6 In the present case, the patient had major dilatation mainly of the distal portion of the esophagus that laid over the diaphragm, making it impossible for endoscopic dilation to be considered a therapeutic option. For megaesophagus grade IV and totally organ dysfunction, esophagectomy is recommended. There is no doubt that esophagectomy allows the patient to swallow again and the treatment is effective. 7 Devaney et al. analyzing 93 patients who underwent esophagectomy for achalasia reported that 95% of them had diet with normal consistency. However, at least 50% of them required endoscopic dilation in the postoperative period. In addition, severe complications occurred in 30% of the patients, with 2% in-hospital mortality. 8 It should be emphasized that because it is a benign condition, a long-term survival is expected, and another long-term complication of this technique is the onset of Barrett's esophagus in the esophageal stump occurring in ∼20% of patients leading to cancer in about 2% of them. 9
The high morbidity rates and the considerable mortality lead us to consider, when possible, procedures that aim to relieve symptoms and improve the quality of patients' life with organ preservation. For patients with recurrent achalasia following Heller's operation, in which esophagectomy is not clearly indicated, one of the options is redoing Heller's cardiomyotomy. This type of procedure can be quite challenging due to the intense fibrosis present in this region. Loviscek et al. analyzing 43 patients reported that 79% of them improved dysphagia with this type of treatment, with 1 year follow-up. However, in 32 (74%) patients the new myotomy could not be made in the same place as the previous one due to intense fibrosis. There were two esophageal perforations, which were primarily treated. There was no mortality and 4 patients required esophagectomy due to the persistence of dysphagia. 10
Another alternative that allows preserving the esophagus and alleviating the symptoms is the Serra-Doria operation. This technique consists the following: annulling the LES obstacle through Grondhal's cardioplasty (esophagogastric LL anastomosis), preventing late stenosis; avoiding the formation of hydrochloric acid and blocking gastric stasis through subtotal gastrectomy (antrectomy) where the parietal cells producing hydrochloric acid are located; and finally to extirpate the bile, pancreatic, and duodenal refluxes through jejunojejunostomy by Roux-en-Y reconstruction. Thereby, gastritis and alkaline reflux esophagitis are averted. 4 In the presented case, this type of operation was indicated because it was a post Heller's cardiomyotomy recurrence with marked dilatation only in the distal portion of the esophagus. The operation of Serra-Doria allowed resolution of symptoms, with organ preservation, which was still functional in its middle and proximal portions. In a study published by Aquino et al., in which 32 patients underwent this technique, the resolution of symptoms in the medium and long term occurred in 81% of the patients. There were 12.5% complications, including three pneumonias and one anastomosis fistula treated conservatively. There was no mortality in this series of cases. 11 Ponciano et al. published a study, in which 23 patients underwent this type of operation after failure of Heller's myotomy. The total resolution of symptoms occurred in 80% of the patients and only 2 patients presented regurgitation after 2 years of follow-up. There was a reduction on esophageal diameter in 53% of patients, and there was no increase on the others. Still, fistula of gastrojejunal anastomosis occurred in 10% (2) of patients, both treated conservatively. 12 Serra-Doria et al. did not report this type of complication in 130 patients operated by this technique. 4 Some degree of dysphagia may persist with this technique. This is due to changes in preexisting esophageal motility that do not improve with surgery.
All the reports found in literature about this technique are from procedures performed through laparotomies. To the best of authors' knowledge, there are no reports about the use of minimally invasive access for such procedure, probably due to the intense fibrosis and adhesions found in the esophagogastric junction and by the complexity to perform this operation. This is the first report with the use of robotic technology. The da Vinci system enables more accurate and safe dissections of structures and tissues under such conditions. In the present study, the use of the robot allowed the identification of all structures, as well as lysis of adhesions. Moreover, it allowed the partial gastrectomy and the accomplishment of anastomosis to be performed safely and ergonomically.13–15
Conclusions
The Serra-Doria operation is an acceptable alternative to treat recurrent achalasia after Heller's cardiomyotomy. It allows adequate relief of symptoms and significant improvement in quality of life. The use of robotic technology for reintervention on the esophagogastric junction facilitates its accomplishment and allows extremely complex procedures to be performed minimally invasively. The methodology of digestive tract reconstruction after gastrectomy with this technology is well established and standardized. Yet, its efficacy and safety have been proved in previous reports.
Footnotes
Disclosure Statement
No competing financial interests exist.