
Abstract
Abstract
Background:
The aim of this study was to evaluate the efficacy and safety of a new articulating bipolar energy device, the EndoWrist® One™ Vessel Sealer (VS), in da Vinci® robot-assisted gastrectomy.
Materials and Methods:
Patients (n = 17) with cT1/2 gastric cancer who underwent robotic gastrectomy using the VS were prospectively enrolled in the study group (VS group). The clinicopathological outcomes, including operative time, intraoperative blood loss, amount of postoperative drainage, postoperative biochemical analysis results, and complication rates, were prospectively collected and compared with those of patients who underwent robotic gastrectomy using conventional ultrasonic shear force ([US] group, n = 52) during the same time period.
Results:
Although the VS provided a good direction for dissection because of the articulating function, the ancillary use of conventional bipolar coagulation was occasionally needed due to the blunt, nonactive end tip of the VS. The operative time, intraoperative blood loss, postoperative drainage, and absence of complication rates did not differ between the VS and US groups, but the C-reactive protein levels on the second postoperative day (8.06 versus 11.7, P = .002) and serum albumin levels on the fifth postoperative day (3.51 versus 3.32, P = .019) were superior in the VS group.
Conclusion:
Use of the VS in robotic gastrectomy was feasible and provided good configuration in the direction of dissection. The learning process for use of the VS in the initial series was relatively rapid, resulting in comparable results between the VS and US groups. Reduced inflammation and albumin loss were identified as possible benefits of the VS.
Introduction
R
One of the most successful surgical systems is the da Vinci® system (Intuitive Surgical, Inc., Sunnyvale, CA), which integrates a high quality 3D visual system and articulating effector instruments with 7 degrees of freedom of movement to overcome the aforementioned limitations. Although the da Vinci system provides many articulating instruments, no articulating energy-based cutting device, which may be one of the most important tools, has been available thus far due to the physical difficulty of developing bendable ultrasonic shear devices.
Recently, an articulating energy-based cutting device using advanced bipolar technology, the EndoWrist® One™ Vessel Sealer (Intuitive Surgical, Inc.), has been launched for the da Vinci system.5–7 This device can be bent up to 50°, and the effector is composed of two rows of coagulators that deliver bipolar electrical energy on either side of the blade to cut tissue. Configured with a relatively sharp blunt tip, this device could be useful for a variety of dissecting procedures in robotic laparoscopic surgery.
The purpose of the present study was to evaluate the feasibility of using this new energy-based device in radical gastrectomy, to explore the possible benefits and drawbacks of the device compared with previous nonarticulating ultrasonic shears and to develop a safe and effective method optimized for radical gastrectomy.
Materials and Methods
Patients
The da Vinci system (Intuitive Surgical, Inc.), which is used to perform robotic surgery, has been explained to patients as an alternative laparoscopic instrument at our institution. The benefits of this system have not been quantitatively demonstrated, and the possible benefits are still under investigation in diverse aspects. Of the patients who agreed to undergo robotic gastrectomy, 18 were prospectively enrolled in the study group using the Vessel Sealer® (VS group) from December 2014 to December 2015 according to the following indications: (1) pathologically proven adenocarcinoma of the stomach, (2) preoperative Tumor Node Metastasis (TNM) stage T1 or T2 and M0 according to the seventh American Joint Committee on Cancer/Union for International Cancer Control (AJCC/UICC) classification, (3) age ≥20 and ≤75 years, and (4) the acquisition of voluntary informed consent. All patients were enrolled in this study only after they voluntarily agreed and provided written informed consent. The study was explained to every patient who met the indications and agreed to robot gastrectomy during the study period, and all the patients enrolled, who voluntarily agreed to this prospective study using the Vessel Sealer, and provided written informed consent. Otherwise, operation was performed using ultrasonic shears (da Vinci Harmonic™ ACE).
One patient was excluded from the study after enrollment due to unexpected peritoneal seeding. The data of remaining 17 patients were compared with comparable data obtained from the patients (n = 52), who underwent robotic gastrectomy using ultrasonic shear force (da Vinci Harmonic ACE) during the same period of the study with preoperative TNM stage as T1 or T2 and M0 (US group).
This study was approved by the Institutional Review Board of Seoul National University Hospital, Seoul, Korea (IRB No.: 1404-129-574).
Operative procedure
All operations followed the general principles of conventional or robotic laparoscopic gastrectomy and standardized stepwise procedures. The operations were performed by 1 operator who was highly experienced in conventional and robotic laparoscopic gastrectomy (>200 laparoscopic gastrectomies annually and >50 cases of robotic gastrectomy before initiation of the study).
The patients were placed under general anesthesia in a supine position, and an 11 mm camera port was inserted below the umbilicus (Fig. 1). After establishment of the pneumoperitoneum, three 8 mm-sized trocars for the robotic arms were inserted in the right lateral area (second arm), left middle area (second arm), and left lateral area (second arm). Another 11 mm trocar for an assistant was inserted at the right middle area. The distance between each trocar was intended to be more than 8 cm. The table was lifted to an ∼15° head-up position. The tower of the da Vinci Si system approached from the direction of the head of the patient and the camera and three robotic arms were attached to the 8 mm trocars.
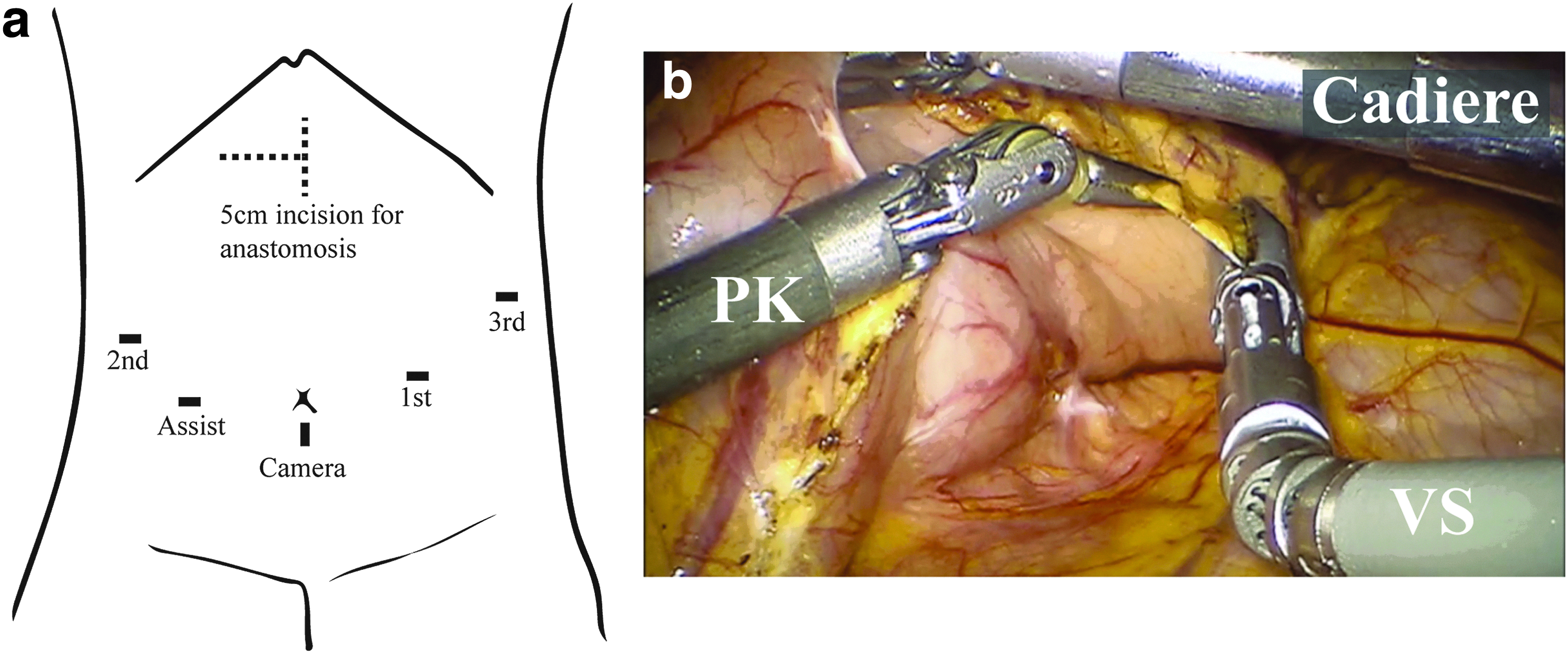
Partial omentectomy was performed in all patients, and D1+LN dissection was performed according to the Japanese treatment guidelines of 2014. 8 The vessel sealer (VS) was installed in the first arm placed at the left middle abdomen and was operated by the right hand of the operator using the remote console. PK® dissecting forceps (PK) and Cadiere forceps were installed onto the second and third arms, respectively. Partial omentectomy and most of the LN dissection were performed using the VS, and the named arteries were ligated using clips. For cancers located in the upper third of the stomach, total gastrectomy was performed without routine splenectomy or LN dissection at the splenic hilum. Pylorus preserving gastrectomy was performed for early gastric cancers located in the middle third of the stomach. LN dissection of the infrapyloric area was meticulously performed with preservation of the infrapyloric artery and vein, and LN dissection around the right gastric artery was omitted to preserve the hepatic branch of the vagus nerve, as in our previously reported standardized procedure for pylorus preserving gastrectomy. 9 For distally located cancers, distal gastrectomy was performed without preservation of the vagal nerve branches.
All anastomoses were made extracorporeally through an incision of ∼5 cm in the upper abdominal wall. For total gastrectomy, end-to-side esophagojejunostomy was performed using a circular stapler. A one-layered hand-sewn gastro-gastric anastomosis was made for pylorus preserving gastrectomy. For distal gastrectomy, an end-to-end anastomosis was created using a circular stapler between the tip of the stapler line at the greater curvature side of the remaining stomach and the duodenum.
Evaluation
The clinicopathological information, operative time, intraoperative blood loss, amount of drainage, postoperative laboratory examination results, incidence and severity of complications, duration of hospital stay, and readmission rate until the 30th postoperative day were prospectively collected. The amount of intraoperative blood loss was evaluated by measuring the added weight of the sponges and the amount of aspirated blood. A closed suction drain was inserted in the subhepatic area, and the amount of the drainage was measured daily until the third postoperative day. Laboratory tests, including a complete blood count, liver function test, renal function test, and C-reactive protein (CRP) test, were performed on the second and fifth postoperative days. All adverse events and complications that occurred during the in-hospital period were documented and graded according to the Clavien-Dindo classifications. 10
All the parameters were compared with comparable data obtained from patients who underwent robotic gastrectomy using ultrasonic shears (da Vinci Harmonic ACE) during the same period of the study (US group). The operative procedure and method of data collection for these patients were performed in the same manner as the study group according to the standard protocol for robotic surgery at our institute. The complication rate and Clavien-Dindo grade were also prospectively collected for all patients in weekly tumor rounds, which ensured for comparability of the data with the VS group.
Statistical analyses were performed using SPSS version 19.0 (SPSS, Chicago, IL). Chi-squared tests and independent t tests were used for comparisons between the 2 groups, and a P < .5 was regarded as statistically significant.
Results
Feasibility of the VS in gastrectomy
A total of 18 patients were enrolled in the VS group, and 1 patient was excluded from the study due to unexpected peritoneal seeding; no resection was performed in this patient.
The remaining 17 operations were successfully performed to fulfill the goal of each procedural step in the standard procedure for robotic gastrectomy.
The articulator function of the VS was useful for dissecting along the desirable dissection plane (Fig. 2a, b) and enabled easier access and dissection behind anatomical structures, such as the right gastric artery and vein (Fig. 2c, d). The VS could be placed along the desirable dissection plane, either left to right or right to left, without the need to change the instruments between the first and second arms, which is sometimes needed when a straight ultrasonic shear is used (Fig. 2e–h).
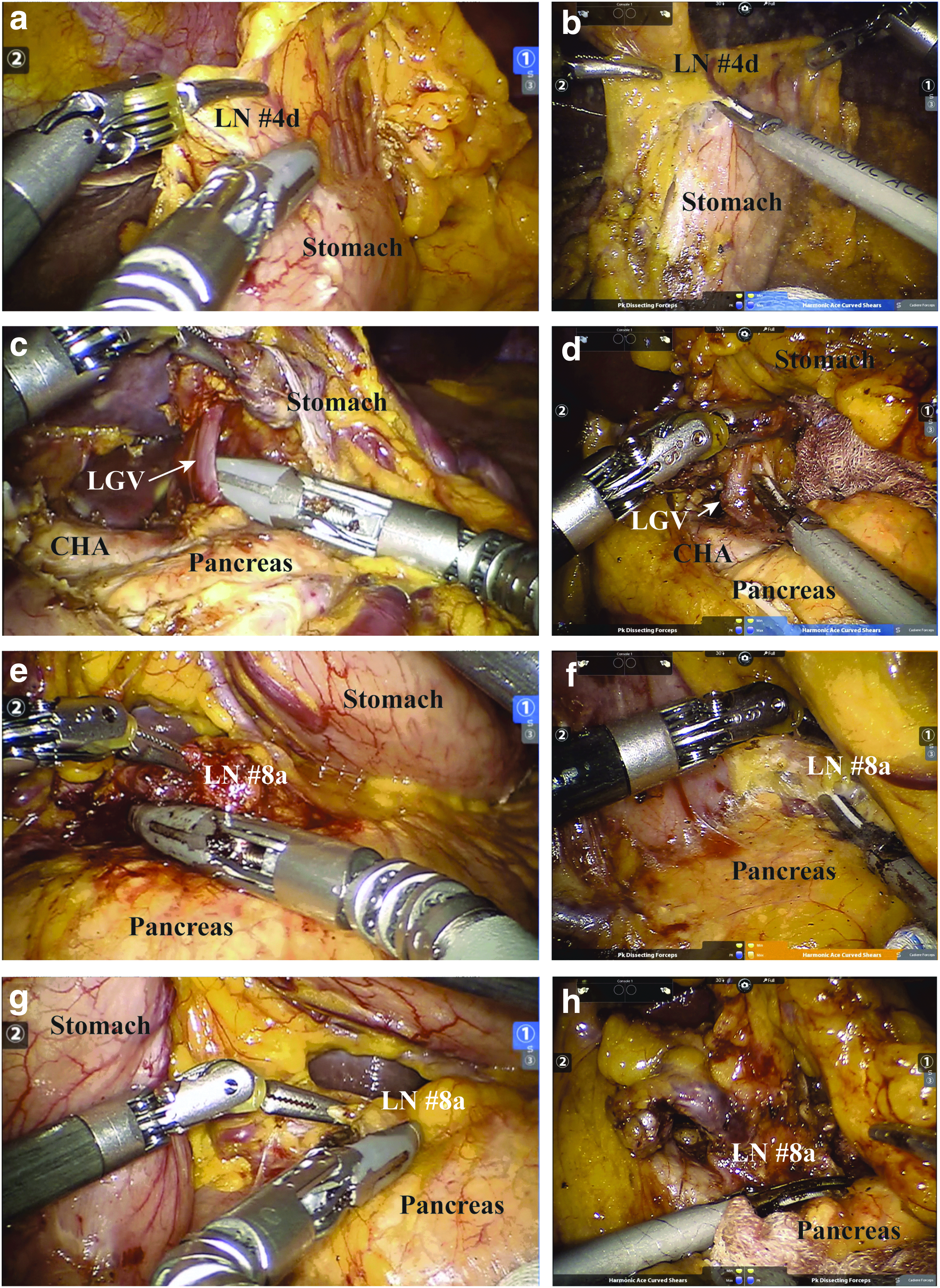
Comparison of the direction of ligation between VS and US.
Coagulation of the small tissues was not possible using the tip of the VS because the bipolar effectors ended a few millimeters distal to the “transection boundary.” These small tissues could be dissected and coagulated by ancillary usage of the PK forceps (Fig. 3a, b). Moreover, because the relatively blunt tip of the device was ineffective at making an entrance hole for one blade of the device, the PK forceps were used to create a small entrance hole for further dissection using the VS (Fig. 3c–e).

Limitations of VS and compensation for them using PK forceps.
Comparisons between the VS and US groups
Table 1 shows the clinicopathological findings of the VS and US groups. There were no significant differences between the 2 groups.
ASA, American Society of Anesthesiologists; BMI, body mass index.
The operative time, estimated blood loss, and number of retrieved LNs were also comparable between the 2 groups (Table 2).
DG, distal gastrectomy; pN, pathologic node; PPG, pylorus preserving gastrectomy; pT, pathologic tumor; TG, total gastrectomy.
Although the complete blood cell count and amount of drainage did not differ between the 2 groups, the CRP level on the second postoperative day and decrease in the serum albumin level on the second and fifth postoperative days relative to the preoperative level were significantly lower in the VS group than in the US group (Table 3).
CRP, C-reactive protein; WBC, white blood cell.
The length of the postoperative stay was similar between the groups. Three hospital readmission cases (5.8%) occurred only in the US group. No significant differences in the complication rates were found between the groups.
There were five complication cases (29.4%) in the VS group. Four cases were graded II and one case was graded IIIa according to the Clavien-Dindo classification system. Among the grade II cases, 1 patient had postoperative extraluminal bleeding at the staple site and recovered after transfusion, two had parenteral nutrition for a postoperative ileus, and another was treated with antibiotics for pneumonia. The grade IIIa case showed delayed gastric emptying resulting from a pyloric spasm after pylorus preserving gastrectomy and recovered after radiologic intervention with balloon dilatation (Table 4).
Discussion
The purpose of this study was to evaluate the application of a new articulating energy device in radical gastrectomy in an initial series. The feasibility and basic safety of the VS were assessed in 17 cases undergoing different types of radical gastrectomy.
An articulating wrist function provided easier access to the target structure in a desirable direction without the need to change the instruments between the robotic arms. The straight energy device should be installed in the second robotic arm on the right side of the patient, especially for parallel dissection along the gastroduodenal artery, common hepatic artery, and splenic artery during LN dissection, and the device should be manipulated by the left hand of the surgeon. Although some experts have expressed the opinion that using the nondominant left hand to manipulate the energy-based cutting device is easier in the da Vinci system than in conventional laparoscopic surgery, there was still a correlation between proficiency of the robotic procedure and manual ambidexterity, and most right hand-dominant operators may have discomfort when manipulating the main surgical instruments with their nondominant hand. 11 Similarly, left hand-dominant surgeons may benefit from using an articulating device to avoid changing the instrument when the dissection plane is better approached from the right side to the left.
The absence of the acting area at the tip of the device beyond the transection boundary limited fine dissection and coagulation in a narrow space, and the bluntness of the tip also needs to be improved to optimize gastrectomy. While PK forceps seem to be helpful in compensating for these drawbacks, we believe that this combined technique may currently be one of the best options for using the VS in radical gastrectomy. The similar number of retrieved LNs between the VS and US groups supports the notion that the adequacy of LN dissection is comparable to previous operative methods using US.
Before this articulating device was developed, some surgeons used articulating monopolar or bipolar electrocautery devices instead of energy-based devices for gastrectomy.12,13 However, the risk of free cancer cell spillage from the lymphatic channels associated with monopolar electrocautery is theoretically higher compared with that associated with the use of energy-based devices because the lymphatic channel is easily opened when cut by electrocautery; thus, free cancer cells that may be present in the lymphatic fluid can spill out. 14 A few previous studies have reported that advanced bipolar or ultrasonic shears provide better security for ligating the lymphatic duct than monopolar electrocautery, with no evident differences between advanced bipolar and ultrasonic devices.15,16 However, the smaller decrease in the serum albumin level in the VS group in this study suggested a possible advantage of the VS over the ultrasonic shear in sealing lymphatic ducts to decrease protein loss. Advanced bipolar shears are known to be more effective in sealing larger vessels than ultrasonic shears due to the inclusion of a mechanism to coagulate protein structures.17,18 Unlike experimental settings testing the lymphatic ducts only, both the lymphatic duct and adjacent soft tissues are dissected and coagulated together during most parts of the surgery. In this sense, it can be interpreted that the VS might provide a better sealing effect. In another interpretation, the lower CRP level in the VS group on the second postoperative day indicated that the VS induced less inflammation around the dissection area and caused less inflammation-related proteins. Although some studies have shown similar lateral thermal damage between different energy devices with a single use, higher temperatures can persist for a longer duration in ultrasonic shears.19–21 Operators tend to use only part of the ultrasonic shears for dissection due to the lack of an articulating function, resulting in a prolonged hot temperature at the tip and an increased risk of collateral thermal damage during laparoscopic surgery. 22 By contrast, the articulating VS system can be aligned to a spatially desirable position to ligate a larger amount of tissue. Consequently, the reduced activation time may have caused less thermal spread during the total operative time and resulted in less inflammation. This interpretation is only theoretical and based on a small sample size, and the possible benefit of the VS to reduce inflammation needs to be validated in well-designed, randomized controlled trials.
One special aim of this pilot study was to examine the feasibility and safety of a new surgical device for the application of a specific surgical procedure immediately after the launch of the device in the market. In particular, the study was partly supported by the manufacturing company so that the initial validation of the device could be made without payment by the patients. Unlike clinical medication trials, in which the use of a medication for another indication is regarded as “off-label,” or clinical trials supported by manufacturers are aimed at expanding the indications of the medication, many surgical devices are launched for general use in a variety of surgical procedures and used directly in the operation without any evaluation of procedure-specific safety. Although the “Idea, Development, Exploration, Assessment, and Long-term Follow-up (IDEAL)” recommendation suggested by McCulloch et al. 23 sufficiently explains the development and evaluation of the surgical innovation, this recommendation does not fully consider the application of the new device in specific surgical procedures. 24 In the case of the VS, for example, we found that the blunt tip was not sufficient for fine dissection in specific areas and that the tip was not electrically active. If ignored, these factors might cause unexpected complications or a larger amount of bleeding if the device is used in the same manner as ultrasonic shears.
We designed this study as a single-arm study to evaluate the initial feasibility and safety of the VS, which may correspond to the “2a development” stage in an IDEAL recommendation. The optimal dosage is decided during the second phase of clinical trials for medications; this phase is replaced with a stage of evolution of the procedure and learning processes in surgical clinical trials. Depending on the learning curve, surgical trials can yield different results in randomized controlled trials.25,26 Therefore, a randomized controlled trial that is performed too early can be biased by initial cases before overcoming the learning curve. Fortunately, we could still compare the results with those obtained from surgeries performed with ultrasonic shears by means of some important parameters because our routine robotic gastrectomy and perioperative evaluation methods followed standardized protocols. For example, the method for measuring intraoperative bleeding and ex vivo LN station separation aided in accurately counting the resected LNs, and all of the postoperative complications were subject to the same prospective identification and grading criteria.27,28 Comparable results between the experimental and control groups showed an early adaptability and short learning curve for using the VS in gastrectomy, at least by an experienced hand.
In summary, this initial pilot series showed the feasibility and safety of the VS in gastrectomy for gastric cancer, and some limitations of the device were identified that could be overcome using possible compensatory methods, with the simultaneous use of a conventional bipolar device. Comparable results between the experimental and control groups suggested the early adaptability of the device and the possible benefits of its use in terms of reduced inflammation and protein loss. These results may justify its application in gastrectomy and diffusion of its usage. In the future, a randomized controlled trial with a larger cohort will determine the possible benefits of the VS assessed in this initial series.
Footnotes
Acknowledgment
This study was partially supported by Intuitive Surgical®, Inc (Grant No. 062014318).
Disclosure Statement
No competing financial interests exist.