
Abstract
Abstract
Background:
Endoscopic intrapyloric Botox (onabotulinumtoxin A; Allergan Pharmaceuticals) injections can improve postfundoplication gastroparesis, but responses are not durable. Surgical pyloroplasty may relieve gastroparetic symptoms, but patient selection criteria are poorly defined. We hypothesize that pyloroplasty provides durable improvement in patients whose symptoms improved after Botox injection.
Study Design:
A retrospective chart review was performed of patients with postfundoplication gastroparesis who improved after Botox injection and then underwent pyloroplasty. Gastric emptying studies (GES), Gastroparesis Cardinal Symptom Index (GCSI) score, symptoms, and outcomes were reviewed.
Results:
Ten patients received Heineke-Mikulicz pyloroplasty after reporting improvement with Botox injection. The mean operative time was 114 minutes (range 55–234 minutes). Three of 10 patients required conversion to open surgery, and the median length of stay was 3 days. Gastroparesis symptom improvement occurred in 9 of 10 patients. Postoperative GES normalized in 5/5 patients (median 205 decreased to 70 min, P < .05). Median preoperative GCSI was 3.67, improved to 2.22 at 1 month postsurgery (P = .010) and to 2.11 on most recent follow-up (P = .015). Median duration of follow-up was 34 months (range 1–101 months).
Conclusion:
Heineke-Mikulicz pyloroplasty can improve symptoms and gastric emptying times in patients with postfundoplication gastroparesis. Improvement with intrapyloric Botox injection may select candidates for pyloroplasty.
Introduction
P
Materials and Methods
After Institutional Review Board approval, a retrospective chart review was performed of patients who presented to our institution between 2006 and 2014 with medically refractory postfundoplication gastroparesis. Inclusion criteria were prior fundoplication(s), gastroparesis symptoms, abnormal gastric emptying studies (GES), subjective temporary symptom improvement after intrapyloric botulinum toxin injection, and treatment with Heineke-Mikulicz pyloroplasty. We excluded patients with diabetic or idiopathic gastroparesis, patients who had only Botox injection or only pyloroplasty, and patients with mechanical gastric outlet obstruction on upper endoscopy. Botox injections were performed by one of the authors (J.F.), using standard endoscopic technique 9 injecting 100 U of Botox divided into 4 quadrants at the pylorus using a 23 gauge endoscopic needle (Interject, Boston Scientific). 7 If patients reported significant symptom improvement at initial clinic follow-up after injection, they were referred to the surgeons (R.G. and E.V.) for pyloroplasty. Preoperative and postoperative symptom data, GES, medication use, and technical outcomes were reviewed. In addition to subjective symptom data from preoperative and postoperative clinic visits, we reached out to all patients and asked them to retroactively complete the Gastroparesis Cardinal Symptom Index (GCSI) survey describing their symptoms before Botox intervention, 1 month postoperatively and at the most recent follow-up. The GCSI is a validated questionnaire and scoring system recently introduced to aid standardization in the diagnosis and treatment response in gastroparesis. 17
Descriptive statistics of demographic and clinical characteristics were reported using the mean (± standard deviation), median (inter-quartile range), and range for continuous variables. Frequency and percentage were reported for categorical variables. A paired t-test was performed to evaluate solid and liquid before and after pyloroplasty. Linear mixed-effect models were used to evaluate the change in Gastroparesis cardinal symptoms index (GCSI) total score and subdomains over time. GCSI scores were measured at baseline, 1 month postsurgery, and at the most recent follow-up visit. This regression model framework adjusted the estimate standard errors to account for within subject correlation. Ninety-five percent confidence intervals and P values were reported from these models. All statistical analyses were conducted in SAS 9.4 (SAS, Inc., NC).
Results
Ten patients met all inclusion criteria. Mean age was 56 years, 70% of patients were female, and mean body mass index was 27.2. All patients had at least one prior fundoplication (range 1–3), and 50% had multiple previous foregut surgeries (range 1–5). The median duration of documented gastroparesis symptoms from the most recent fundoplication to the first Botox treatment was 18 months (range; 4–38 months). Patient characteristics are provided in Table 1. The median time from Botox injection to pyloroplasty was 83 days (range 40–286 days). Pre-Botox GES was obtained in all 10 patients and mean GES T1/2 for solids was 220 minutes (±61 minutes). Laparoscopic pyloroplasty was attempted on all patients, and 3 of 10 patients required conversion to open surgery. The mean operative time was 114 minutes (±57 minutes). The median length of stay was 3 days (range 1–36 days). There were no surgical site infections. One patient had a suture line leak requiring takeback laparotomy and repair followed by postoperative bowel obstruction eventually requiring repeat laparotomy and lysis of adhesions.
One missing observation.
IQR, interquartile range; SD, standard deviation.
Median duration of follow-up was 34 months (range 1–101 months). Five of 10 patients had postoperative GES, and all 5 patients had normalization of gastric emptying. Mean GES T1/2 for solids decreased from 205 (172, 220) to 70 (48, 76) min (P < .001) and for liquids decreased from 50 (37, 50) to 25 (24, 26) minutes (P = .047) (Fig. 1). Nine out of 10 patients reported subjective improvement in overall gastroparesis symptoms, including nausea, bloating, and postprandial fullness, at the initial postoperative follow-up. Prokinetic medications were discontinued in 3/5 patients postpyloroplasty. Symptom improvement was durable in eight of nine patients who completed the GSCI on long-term follow-up. The remaining patient was symptom free at 1-month follow-up, but could not be contacted to complete the GCSI questionnaire. Average pre-Botox GCSI was 3.67 (3.33, 4), with improvement to 2.22 (1.56, 2.44) at 1 month postsurgery (P = .010) and to 2.11 (1.44, 3) at the most recent follow-up (P = .015). Individual GSCI symptom subdomains (nausea, fullness/early satiety, and bloating) also showed similar statistically significant improvement (Fig. 2). One patient developed recurrent gastroparesis symptoms and was successfully treated with conversion to Roux-en-Y gastrojejunostomy 6 years after the initial surgery. Three patients with durable resolution of gastroparesis symptoms required subsequent foregut surgery for recurrent paraesophageal hernia.
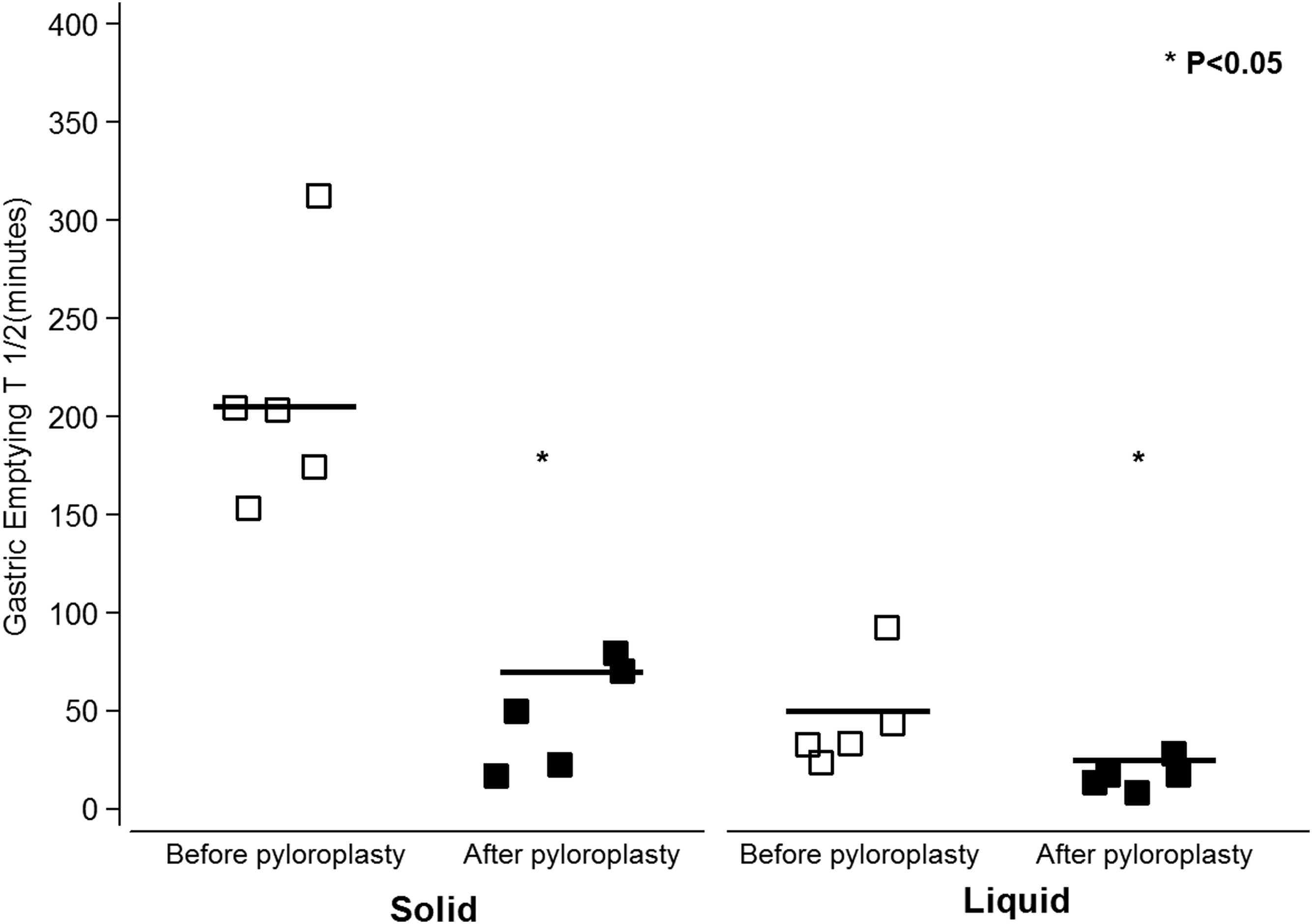
Preoperative and postoperative gastric emptying times (n = 5).
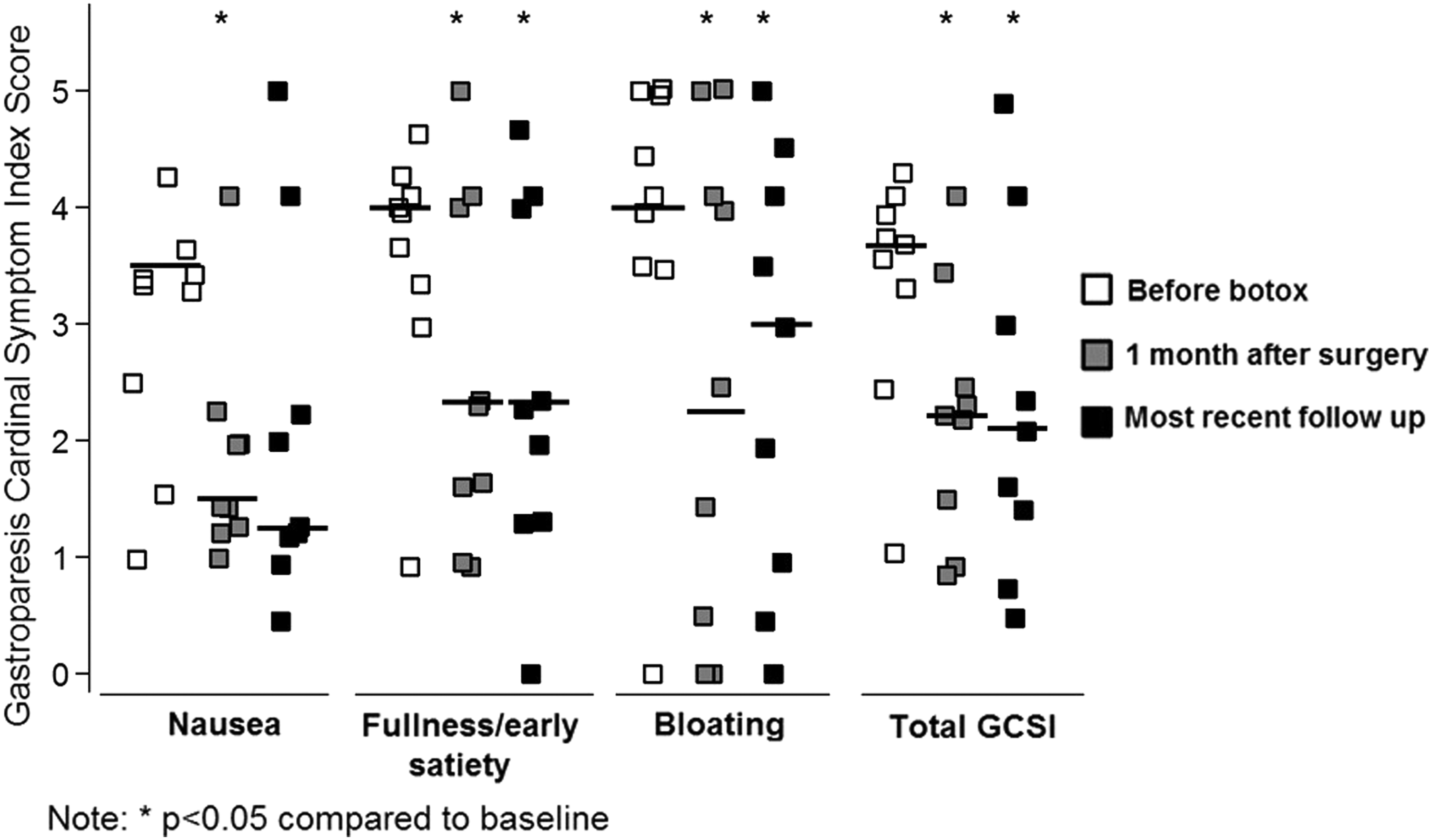
Preoperative and postoperative gastroparesis cardinal symptom index score: individual symptom subdomains and total (n = 9).
Discussion
Symptoms of gastroparesis include nausea, emesis, early satiety, postprandial fullness, bloating, and upper abdominal pain. Gastroparesis causes significant debility, decreased quality of life, and even increased mortality.18–20 It is diagnosed by symptomology, abnormal GES, and exclusion of mechanical gastric outlet obstruction. Dietary modification and medical therapies such as antiemetics and promotility agents are the initial treatment of postfundoplication gastroparesis, but the best intervention in medically refractory gastroparesis remains unclear. Endoscopic intrapyloric Botox injection was initially shown in nonrandomized trials to provide short-term symptom relief,6,8 although the duration of effect is limited.7,9 Subsequent prospective randomized controlled trials did not demonstrate efficacy11,12 and Botox treatment is no longer recommended in current guidelines.12,21 Surgical treatment options for refractory gastroparesis include Heineke-Mikulicz pyloroplasty, subtotal gastrectomy, jejunostomy tube placement, implantable gastric stimulation, and Roux-en-Y gastric bypass. However, criteria for and selection of these various surgical options are unclear.
The role of pyloric dysfunction may be particularly pronounced in the pathophysiology of postsurgical gastroparesis. 4 Postfundoplication vagal nerve injury is identified in 4%–40% of patients undergoing laparoscopic fundoplication, 22 leading to impaired pyloric relaxation and decreased pyloric compliance. 23 Intrapyloric Botox injection has been studied largely in patients with idiopathic or diabetic gastroparesis, where the pathophysiology is more heterogeneous. However, intrapyloric Botox is inadequately studied in patients with pylorospasm. 24 Botox may be more efficaciously useful in postsurgical gastroparesis, where vagal dysfunction and increased pyloric tone may drive gastroparesis and antral motor function is preserved. We hypothesized that a favorable response to Botox may better select patients with this pathophysiology who would benefit from pyloric defunctionalization with surgical pyloroplasty.
Previous studies of pyloroplasty in gastroparesis have examined a mixed population of idiopathic, diabetic, and postsurgical gastroparesis. Toro et al. demonstrated subjective improvement in 82% of patients and improvement of gastric emptying times in 96% of patients in a retrospective study of 50 postpyloroplasty patients with mixed idiopathic, postsurgical, and diabetic gastroparesis. 16 Hibbard et al. demonstrated an 83% subjective success rate in treatment of gastroparesis and a statistically significant improvement in antiemetic use and symptom severity score in 26 patients receiving laparoscopic pyloroplasty. Masquisi et al. reported subjective improvement in 80% of 35 patients who underwent combined fundoplication and pyloroplasty, along with statistically significant improvement in gastric emptying time and bloating as measured by GERD symptom severity score. 25
We demonstrate similar outcomes to these previous studies, while focusing on postfundoplication gastroparesis, a condition in which pyloric relaxation may be uniquely efficacious given the pathophysiologic role attributed to vagal nerve injury in this patient population. Our study demonstrates that in a carefully selected group of postfundoplication gastroparesis patients in whom Botox injection and pyloric defunctionalization resulted in short-term symptomatic improvement, pyloroplasty resulted in durable improvement in gastroparesis symptoms. This benefit is observed in objective measurements of gastric emptying function, in subjective reporting of gastroparesis symptoms, and in retrospective completion of the GCSI questionnaire. Symptom improvement occurred in 90% of patients and was durable in 89% of patients at long-term follow-up. A single patient with recurrent symptoms was managed successfully with Roux-en-Y gastrojejunostomy. GCSI improvement was statistically significant at the initial follow-up and was very close to significance on long-term follow-up despite small sample size. We further suggest that Botox might serve to prospectively identify patients who will benefit from definitive defunctionalization of the pylorus, although further study is needed. Pyloric manometry has been similarly used, but Botox has the advantages of closely replicating the defunctionalization of the pylorus and providing a short-term therapeutic benefit, and is more widely available.
Our study has several limitations as an unblinded retrospective series. It is subjective to the bias inherent to retrospective review, as well as to possible contribution of the placebo effect. In addition, this was a nonblinded study; so our GCSI questionnaire is subject to a recall bias. However, most patients did clearly feel their intervention improved their overall symptoms. It may be reasonable to question whether intrapyloric Botox injection is necessary before pyloroplasty, but given the need for preoperative endoscopy to exclude gastric outlet obstruction, the low complications associated with Botox injection, and the potential for complications with pyloroplasty, we feel Botox trial has a favorable risk-benefit ratio. A limited number of patients with postfundoplication gastroparesis received Botox, but did not have symptom improvement, and therefore did not receive pyloroplasty. Exclusion of these patients from the study could contribute to our long-term success rates. A next step could be a prospective trial randomizing patients to Botox versus placebo injection before offering laparoscopic pyloroplasty, but given the low incidence of the condition, this may not be feasible.
Conclusion
Heineke-Mikulicz pyloroplasty can offer symptomatic improvement and improved gastric emptying for patients with postfundoplication gastroparesis. Symptomatic improvement after intrapyloric Botox injection may help select patients for surgical therapy with pyloroplasty for refractory postsurgical gastroparesis.
Footnotes
Disclosure Statement
Dr. Daniel Gilsdorf, Dr. Eric Volckmann, Abbie Brickley, Linda Taylor, and Dr. Robert Glasgow have no conflicts of interest. Dr. John Fang is a consultant to Boston Scientific and owner of Veritract.