
Abstract
Abstract
The field of laparoscopic surgery has continued to grow exponentially over the years, prompting new innovative technologies. Despite substantial advancements, standard laparoscopic tools have undergone little design changes and fail to optimize mobility in limited spaces. Advancements in robotics have attempted to address this, allowing for increasing degrees of freedom and articulation of instruments. Even so, this system has proven to be cumbersome with questionable cost-effectiveness. In this study, we present the first use of a solely mechanical intuitively controlled articulating laparoscopic needle driver. The ability to naturally articulate allowed for ease during suturing and knot tying during the critical portions of the operation. The FlexDex surgical instrument demonstrates promise in the field of foregut surgery in addition to other areas of minimally invasive specialties.
Background
W
The introduction of minimally invasive robotic surgery attempted to solve this problem, providing articulation and improved degrees of freedom (DOF) for the surgeon and intuitive control. With the standard laparoscopic straight stick, the limited four DOF inhibits knot tying, suturing, and dissection in small spaces.3,4 While the robot provides the benefit of articulation, multiple studies have failed to demonstrate both its clinical- and cost-effectiveness.5–10 This has been the subject of ongoing studies and debate, limiting its widespread adoption. 11 Despite the cost, the robotic industry has witnessed substantial growth over the past decade. Providing a more cost-effective method of articulation and increasing the surgeon's intra-abdominal DOF have been the focus of previous groups in the past (i.e., Cambridge Endo, Novare RealHand, and so on).12,13 Despite showing promise, adoption has been limited by their poor functionality, lack of intuitive control, and inability to lower cost. Over the past decade, FlexDex, Inc. (Brighton, MI) has focused their efforts on this need to provide a purely mechanical method for intuitively controlled laparoscopic articulation. 14 With the recent release of their device, the FlexDex Needle Driver (FlexDex, Inc., Brighton, MI) provides robotic like articulation with novel intuitive hand control through a Virtual Center™ mechanism; the functionality and potential of the device for foregut surgery are promising.
In this study, we present the initial use of the FlexDex laparoscopic needle driver (FDA Class 1) in a case of reoperative foregut surgery. In this patient, the instrument effectively enhanced the operating surgeon's DOF within a small working space. This allowed efficient suturing and knot tying with minimal effort. While the learning curve to proficiency remains to be studied, this case demonstrated the first use of a strictly mechanical intuitively controlled articulating laparoscopic instrument.
Case Report
This is the case of a 2-year-old, 10 kg, male with a history of congenital neuropathy, cortical blindness, and gastrostomy tube dependence, with a recent laparoscopic Nissen fundoplication for gastroesophageal reflux. This initial operation was performed at an outside hospital and was complicated by severe blood loss due to liver injury, but the patient did well postoperatively with no complaints. One year later, he developed an acute onset of worsening nausea with emesis and inability to tolerate feeds. An upper gastrointestinal (GI) contrast study was obtained which demonstrated slippage of the wrap. Based on these findings and clinical symptoms, the patient was taken to the operating room for a reoperative Nissen fundoplication.
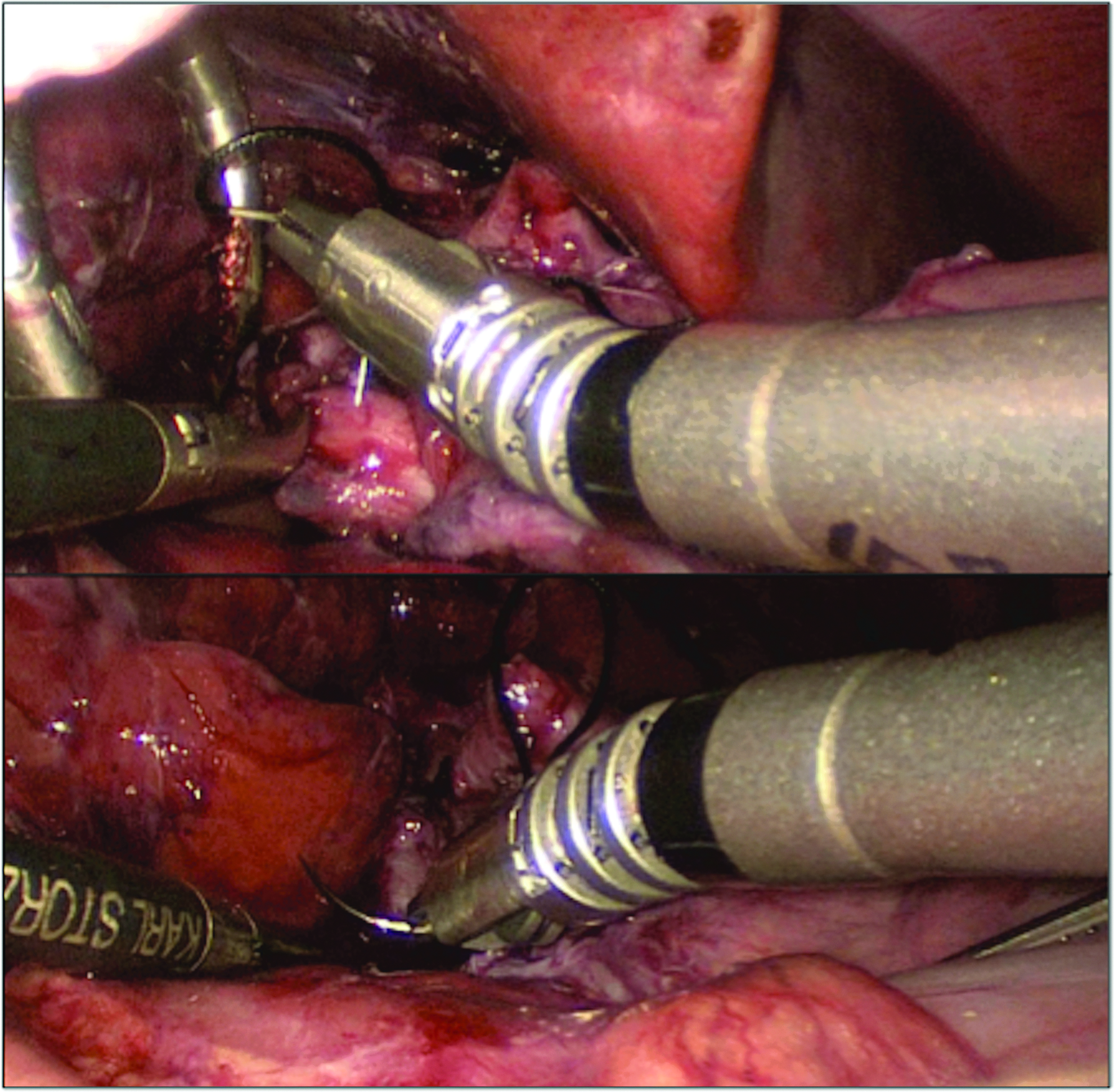
After the induction of general anesthesia and standard patient preparation and positioning, a 5-mm incision was made at the umbilicus, and a Step trocar (Medtronic) was used for port placement. Three additional 5-mm ports and one 8-mm port were placed under direct visualization. A liver retractor was placed into the lateral port for anterior liver retraction. Utilizing both blunt and sharp dissection, the old wrap was visualized and subsequently taken down. There was a substantial amount of adhesions with spleen and liver involvement resulting in an injury to the proximal stomach. Using the FlexDex needle driver, a 3-0 Vicryl suture was used in a running manner to suture the gastrotomy closed. After the wrap had been successfully taken down, a 30F bougie was placed down the esophagus under direct visualization, demonstrating a small hiatal hernia. Using the FlexDex needle driver, a single interrupted 2-0 silk suture was used to bring the hiatus together (Figs. 1 and 2). After the mobilization process, there was adequate fundus coverage and esophageal length, allowing for the reoperative Nissen fundoplication. Using the FlexDex, three interrupted 2-0 silk sutures were used to create the wrap, starting 2 cm cephalad to the gastroesophageal junction and ending 1.5 cm caudal to the gastroesophageal junction (Figs. 3 and 4). The patient had an upper GI swallow study postoperatively, which demonstrated no leak or stricture. The patient tolerated feeding advancement and was discharged on postoperative day four.
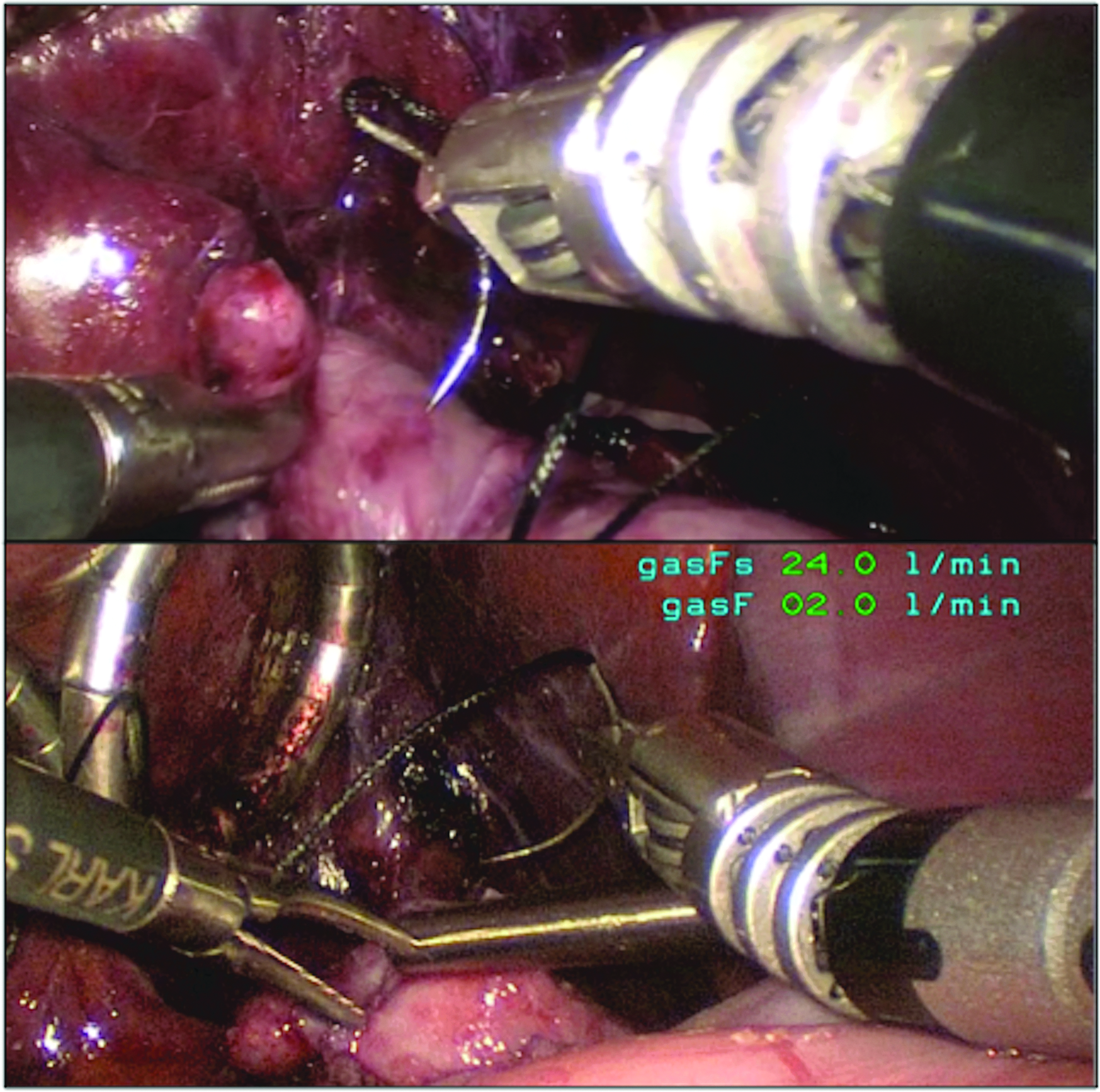
Suturing using articulation.
Suturing using FlexDex.
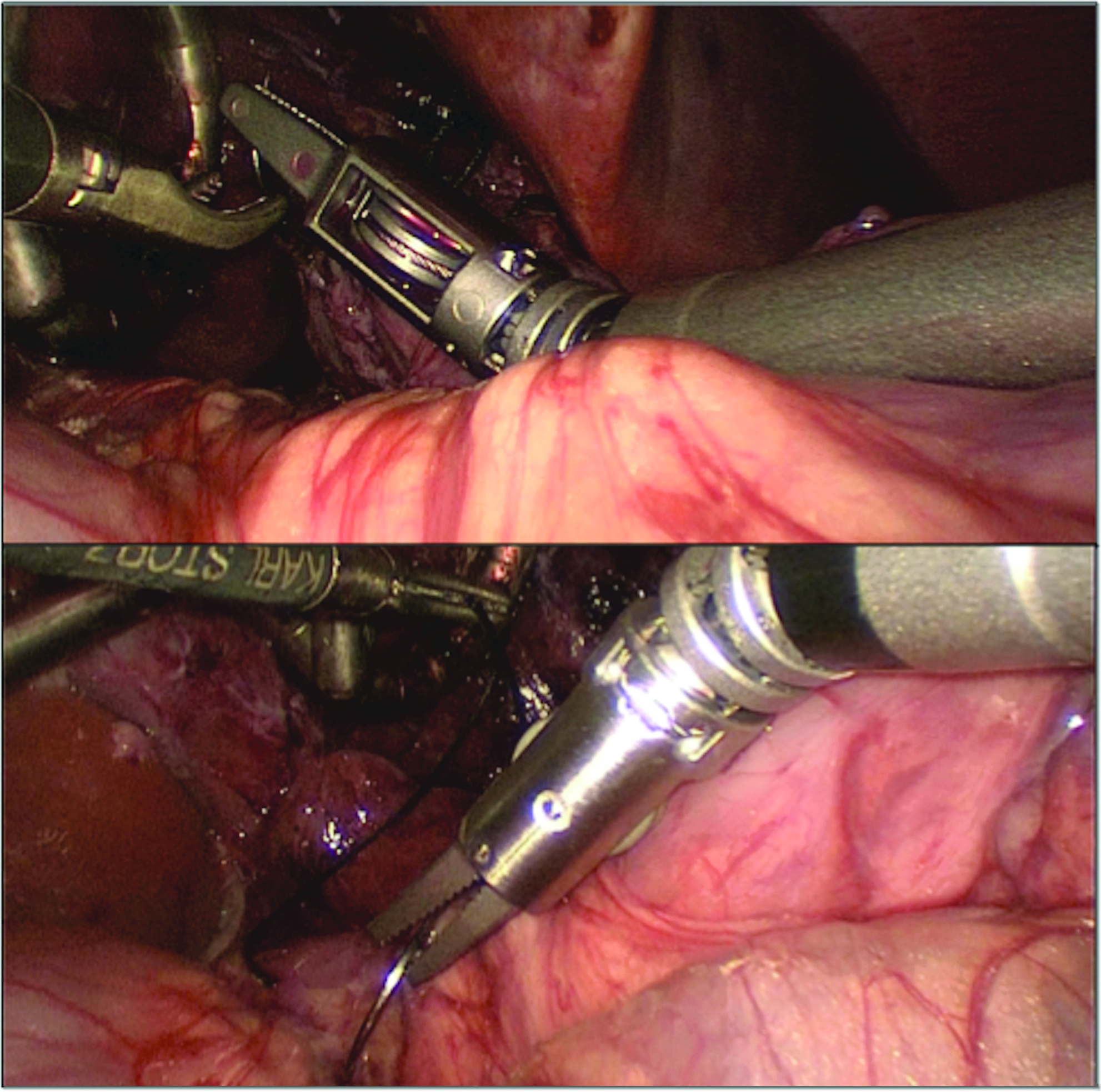
Grasping the needle.
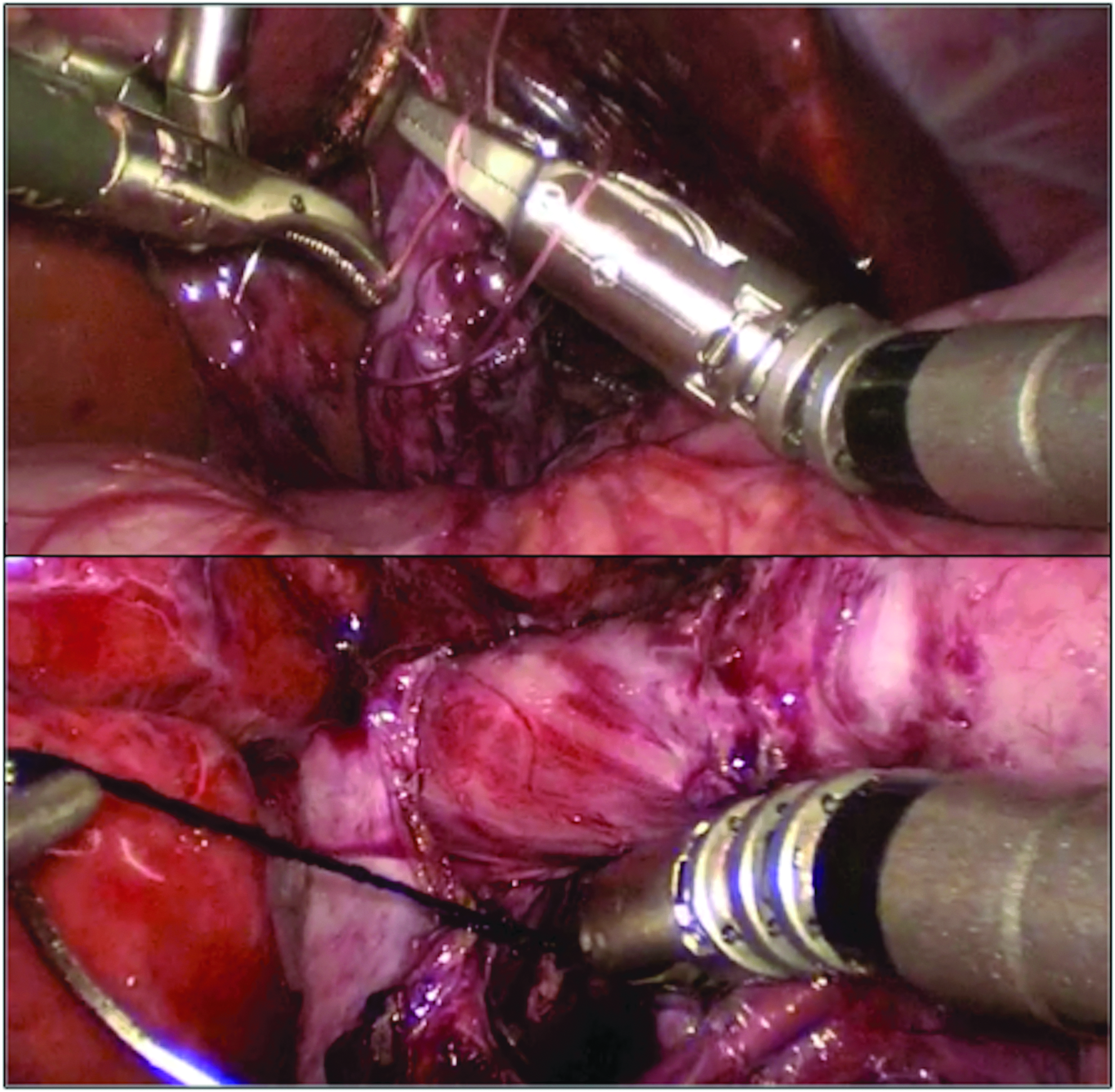
Knot-tying using the instrument.
Discussion
This case demonstrates the first clinical use of the FlexDex Needle Driver, an articulating laparoscopic needle driver with intuitive control. With the ability to improve dexterity and surgical range of motion strictly through mechanical technology, the instrument has the potential to provide a more cost-effective method to improve instrument DOF and thus functionality while operating. In this study, we present a case of a Nissen fundoplication where previous adhesions impacted working space and visualization, prompting the use of the novel laparoscopic instrument to enhance suturing and knot tying. Overall, the instrument demonstrated effectiveness, with an improved ability to suture at the hiatus and distal esophagus.
There has been a great deal of advancements in laparoscopy over the years with the development of improved camera optics, electrocauterization devices, image guidance, and training modules.15–18 Despite this, there have been limited strides in the advancement of the laparoscopic tool itself. 1 While multiple previous iterations of articulating devices have been attempted, their poor functionality likely contributed to their lack of widespread adoption.3,19,20 Overall, one of the most effective improvements in range of motion for the surgeon was the implementation of the robot surgical system. 21 Initially launched in 1999, the da Vinci® System (Intuitive Surgical, Inc., Sunnyvale, CA) allowed a surgeon to operate with higher DOF and range of motion, while potentially enhancing ergonomics and comfortability. Over 2500 da Vinci Systems are installed in the United States, and a number of new robotic surgical systems are expected to be launched in the next 2 years.22,23 Despite representing significant advancements in robotic technology, these products remained remotely controlled, adding to their high cost. Initially developed as a collaboration of Department of Mechanical Engineering and Department of Pediatric Surgery at the University of Michigan, Ann Arbor MI, the FlexDex instrument operates solely on mechanical technology, without the use of tethered cords or electronics. Using a design controlled solely by the hand and wrist, the movements of the instrument tip mimic the surgeon's hand, allowing for maneuverability across the operating room table while still providing force feedback to the surgeon (Fig. 5).
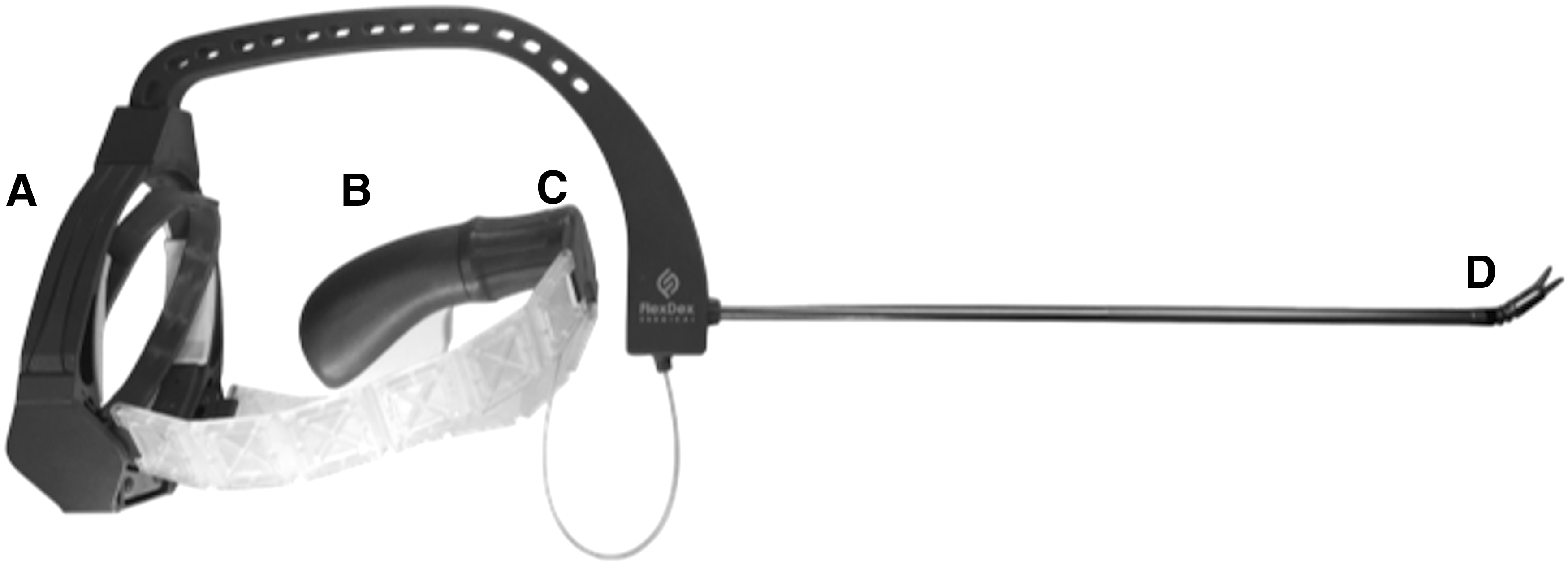
FlexDex Needle Driver.
During laparoscopy, one of the challenges is crowding of instruments both on the inside and outside of the body (Fig. 6). Because of the FlexDex needle driver's unique architecture compared to standard laparoscopic instruments, we anticipated some conflicts of the device frame (e.g., with the light cord or another instrument). However, in this 10 kg patient this was not an issue. Second, with any new instrumentation technology there is a definite learning curve required before utilizing the instrument in the operating room. Surgeons who have a tendency to perform traditional maneuvers in laparoscopy, such as abducting the shoulder, flexing/extending at the elbow, and rotating the forearm for suturing and manipulation of tissue, will have to break those habits as they learn to use FlexDex. In an attempt to help with this, there are self-driven training videos that are highly recommended to be completed before clinical use. In the same manner that surgeons initially were required to learn standard laparoscopy from open procedures, a required effort from the operating surgeon is essential to optimize the potential of the technology and facilitate its adoption. 24
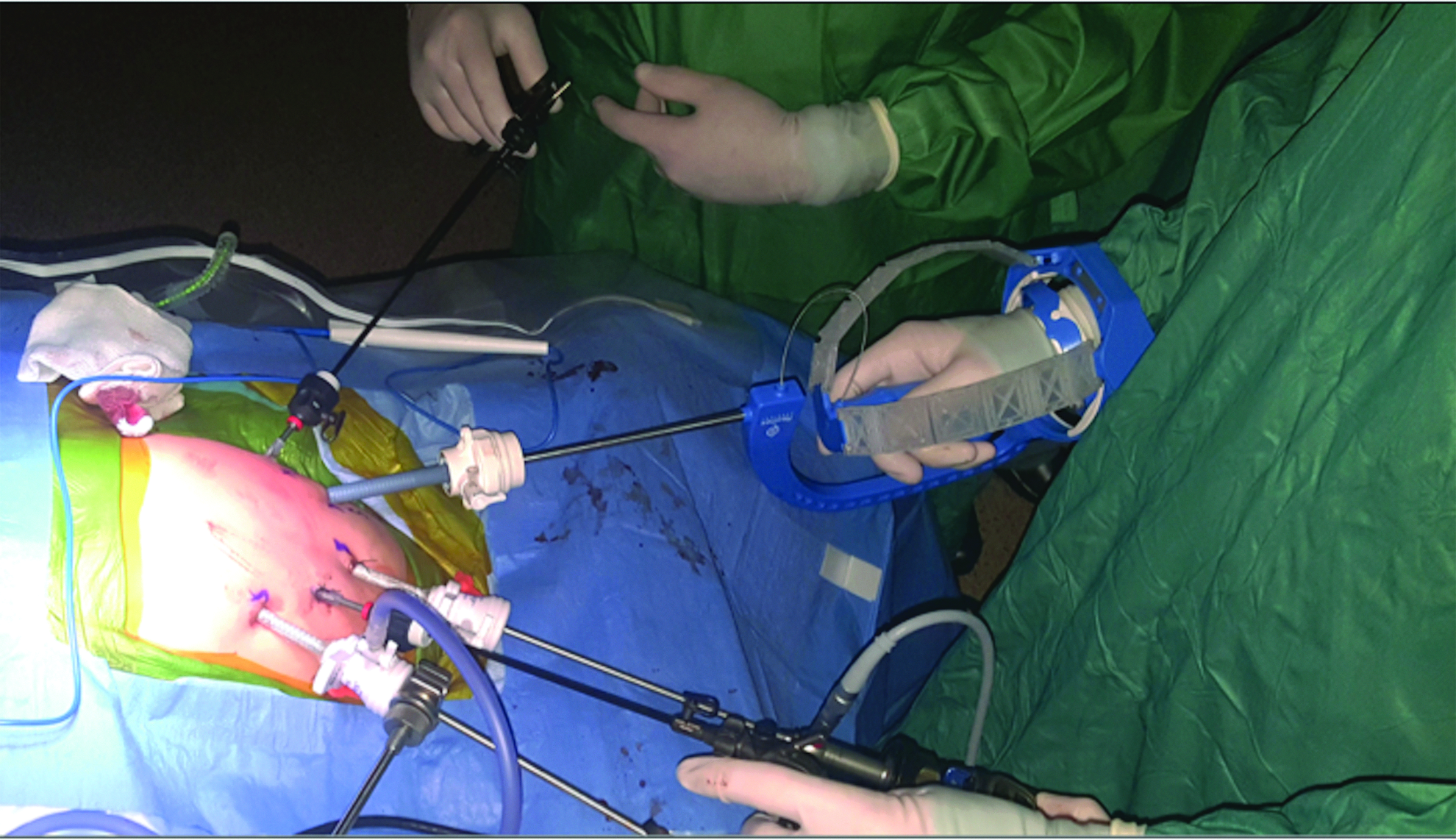
Viewpoint of instrument from outside.
Conclusion
This case demonstrates the initial use of an intuitively controlled articulating laparoscopic needle driver. By providing articulation and intuitive control, the needle driver successfully enables suturing and knot tying in limited spaces, ideal for minimally invasive foregut surgery.
Footnotes
Disclosure Statement
J.D.G. and S.A. are co-owners and coinventors of the FlexDex Needle Driver device (FlexDex, Inc.). No other competing financial interests exist.