
Abstract
Abstract
Introduction:
Laparoscopy for rectal cancer is a challenge as it presents many technical difficulties and requires high level of expertise. That is the reason for the high conversion rate. Reports on outcomes of converted cases after laparoscopic rectal resection for cancer are conflicting.
Aim:
The present meta-analysis compares short- and long-term outcomes between converted rectal cancer cases with both open and laparoscopically completed cases.
Method:
All studies reporting on outcomes separately for the converted cases were reviewed systematically. Main outcomes were intraoperative complications, procedure duration, short-term mortality and morbidity, length of stay, local recurrence, number of lymph nodes retrieved, and distant metastases. Quality assessment and data extraction were performed independently by 3 reviewers.
Results:
Fourteen studies were eligible for analysis, including 10,845 patients. Overall conversion rate was 11.9%. Converted cases had significantly longer duration, hospital stay, and higher rates of wound infection compared with laparoscopic cases. All other outcomes had no difference. When compared with open cases, conversions displayed longer operative times, but there was no other significant difference in the short- or long-term outcomes.
Conclusion:
Converted cases seem to have some short-term unfavorable outcomes. Further retrospective analysis of big registries will be helpful for further investigation of converted cases.
Introduction
T
According to the aforementioned literature, the laparoscopic approach for colon cancer surgery is associated with conversion to open in rates ranging between 7% and 25%. Reasons for conversion include obesity, previous abdominal surgery, bulky or T4 tumors, and technical factors such as inadvertent visceral damage or bleeding. Conversion rate of laparoscopic surgery for rectal cancer is even higher, overcoming 30%. 3 Male gender, large rectal tumors, and difficulties in dissection and transection of rectum distal to the tumor are additional reasons for conversion.12,18
There are conflicting reports on the short-term and oncological outcomes of converted-to-open cases; some studies show similar, 19 while others show worse,20–23 results compared either with laparoscopically completed cases or with those attempted by the open approach.
In an effort to elucidate the issue, we conducted a meta-analysis of studies reporting on immediate postoperative and oncological outcomes of converted-to-open rectal cancer cases in comparison with both the laparoscopically completed cases and those operated upon by open surgery.
Methods
Study selection
A MEDLINE, Embase, Ovid, and Cochrane database search was performed to identify all comparative studies on laparoscopic versus open rectal cancer surgery, which reported separately on outcomes of the converted cases. The following Mesh search headings were used: rectal cancer, laparoscopic rectal resection, conversions, rectal resection, abdominoperineal resection, low anterior rectal resection, laparoscopic low anterior rectal resection, laparoscopic abdominoperineal resection, comparative study, randomized study, and treatment outcomes. The related articles function from PubMed was used to broaden the search, and all abstracts, studies, and citations scanned were reviewed. No language restrictions were made. The search included the period from January 1991 to June 2013.
Inclusion criteria
The following inclusion criteria were used: (1) all studies had to report only on rectal cancer cases; (2) report at least one of the outcome measures investigated by the study (outcomes of interest); and (3) all studies had to report separately on converted cases. Studies that were reported by the same institution and/or authors were included in the absence of overlap between the results and the patients. In the case of overlap, the larger and/or higher quality study was included in the analysis. All discrepancies were resolved by consensus among the authors.
Exclusion criteria
Studies were excluded from the analysis if (1) the outcomes of interest were not clearly reported for the open, laparoscopic, and converted cases; (2) it was impossible to extrapolate or calculate the necessary data from the published results; and (3) there was considerable overlap between authors, centers, or patient cohorts evaluated in the published literature.
Outcomes of interest
The following outcomes were included: (1) perioperative outcomes, including bleeding, conversion to open (for laparoscopic cases), and duration of the procedure; (2) immediate postoperative mortality and morbidity, including bleeding, anastomotic leak, pelvic sepsis, urinary complications, wound-related complications, and systemic complications; (3) length of hospital stay expressed as days in the hospital after primary surgery; (4) oncological outcomes expressed as 5-year local recurrence and survival rates and number of lymph nodes excised; (5) length of follow-up; and (6) reoperation rates.
Comparisons were made between laparoscopic and converted cases from all included studies and between open and converted cases from comparative studies comparing laparoscopy with the open approach.
Statistical analysis
Qualitative outcomes were expressed as percentages over the total number of patients. Quantitative outcomes were expressed as overall mean. Meta-analytical techniques were used to compare outcomes between the laparoscopic and converted cases as well as between the open cases and the converted ones. The meta-analysis followed recommendations from the Cochrane collaboration and the quality of reporting of meta-analyses guidelines. Odds ratio (OR) was used as the summary statistic to perform statistical analysis of dichotomous variables and was reported with 95% confidence intervals (CI). ORs represent the odds of an adverse event occurring in the preoperative period compared with the postoperative period. OR <1 favored the converted cases, and the point estimate of the OR was considered to be statistically significant at the P < .05 level if the 95% CI did not include the value one. Two strategies were used to quantitatively assess heterogeneity. A fixed- (weighted with inverse variance) or a random-effects model was used for this meta-analysis. Heterogeneity between studies was assessed by the chi-square and I 2 statistic. Higher chi-square and I 2 statistic indicates greater heterogeneity between studies. The assumption of homogeneity between the groups was deemed invalid if the P-value was <.1 and the random-effects model was reported after exploring the causes of heterogeneity. Otherwise, the fixed-effects model was reported. All meta-analyses were performed with Review Manager, version 5.2. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2012. The difference between the groups as far as the staging is concerned was identified with the use of chi-square test performed with IBM SPSS statistics, version 21.
Results
Eligible studies
One hundred sixty-eight publications were identified using the methodology described in Methods section (Fig. 1). Forty-seven studies were deemed irrelevant and another 45 reported on technical issues or other relevant minimally invasive techniques; they were all excluded following title and abstract review. Fifteen studies were reviews and therefore excluded. Thirty-five studies reported on incidence or predictive factors for conversion, but not on outcomes of converted cases, while data could not be extracted from another 12 studies because outcomes of conversion were pooled and reported together with other than rectal cancer colorectal pathologies. The remaining 14 studies were considered for the purposes of the present study and were fully investigated. Examination of the references of these studies did not provide any further studies for evaluation. The last one was excluded because it did not report any of the outcomes of interest. Finally, a total of 13 studies, published between 2001 and 2012, fulfilled the selection criteria and were included in this review.12–14,24–33 Of these studies, 6 were comparative studies between the open and the laparoscopic approach12,13,27,29,30,32 and 7 were laparoscopic series, which reported on outcomes of converted cases.14,24–26,28,31,33 The total number of patients assessed by the included studies was 10,781, of which 3064 were operated laparoscopically and 360 were converted to open (11.75%). The most important characteristics of the included studies are presented in Table 1. Main reasons for conversion to open surgery were obesity, advanced fixed tumors, adhesions, intraoperative bleeding, problems with fashioning of the anastomosis, problems with instrumentation, and ureter-related issues.

PRISMA Flowchart.
Laparoscopy versus conversions
Demographics
Six studies report on patients' age.24,27,29,31–33 Three of them were comparative27,29,32 and three were laparoscopic series.24,31,33 Pooling of all available data on patients' age did not reveal any statistically significant difference between laparoscopic and converted cases (mean diff. −0.83 years [−2.44, 0.79], I 2 : 0%, z: 1.01, P = .31).
Three studies report on body–mass index (BMI).24,31,33 All studies were laparoscopic series. Pooling of data revealed that converted-to-open patients had significantly higher BMIs than those who were completed laparoscopically (mean diff. −2.20 Kg/m2 [−2.96, −1.45], I 2 : 0%, z: 5.71, P < .00001) (Fig. 2).

Laparoscopically completed versus converted cases—Body–mass index (BMI-Kg/m2). SD, standard deviation; CI, confidence intervals.
Four studies reported on the number of patients who received any kind of neoadjuvant treatment (chemoradiation or radiation alone).13,14,24,31 The rates of the laparoscopic group whose patients were offered neoadjuvant treatment ranged from 10.35% to 74.2%. On the other hand, rates for the conversion group ranged from 0% to 100%. Pooling of data from the abovementioned studies did not reveal any statistically significant difference between the two groups (OR: 0.91 [0.18, 4.56], I 2 : 62%, z: 0.11, P = .91). Significant heterogeneity could be identified among the studies available for analysis.
Five studies had data on the staging of patients according to the Union for International Cancer Control (UICC).13,24,29,30,33 These studies included 1700 patients with 160 converted-to-open cases and 1540 cases completed by the laparoscopic approach. Analysis with cross-tabulation with the chi-square test revealed that significantly more patients with advanced stage (stages III and IV) were converted (stage III: converted 63/160%–39.4% versus laparoscopic 411/1540%–26.7%, stage IV: converted 17/160%–10.6% versus laparoscopic 102/1540 6.6%, chi-square test 18.629, P < .001).
Intraoperative outcomes
Operation duration was reported by eight studies.14,24,27–31,33 Three were comparative27,29,30 and the rest five were laparoscopic series.14,24,28,31,33 Pooling of all data showed that converted-to-open cases lasted significantly longer than the ones completed by laparoscopy [mean diff.: 25.28 minutes (2.62, 47.94), I 2 : 95%, z: 2.19, P = .03], although there was significant heterogeneity among studies (Fig. 3).

Laparoscopically completed versus converted cases—Operation duration (minutes).
Immediate postoperative outcomes
Hospital stay was reported by eight studies.14,24,27–31,33 Analysis of all available data from all studies identified a statistically significant difference favoring the laparoscopic group by a mean difference of 2.86 days [mean diff.: 2.86 days (1.81, 3.92), I 2 : 29%, z: 5.32, P < .00001] (Fig. 4). No significant heterogeneity could be identified among the studies.

Laparoscopically completed versus converted cases–Hospital stay (days).
Five studies reported data on mortality.12,28,29,32,33 Mortality rates ranged from 0% to 8.3% for converted cases and from 0% to 15.2% for the laparoscopic group. Pooling of data did not reveal any difference between the two groups (OR: 2.8 [0.29, 26.96], I 2 : 52%, z: 0.89, P = .37). The analyzed studies displayed marginal heterogeneity.
Six studies had available data on overall morbidity.12,28–31,33 The conversion group displayed rates ranging from 15.3% to 54.2%, while the laparoscopic group's morbidity ranged from 20.9% to 37.1%. Analysis of pooled data revealed no difference between the two groups (OR: 1.58 [0.83, 3.01], I 2 : 68%, z: 1.4, P = .16) (Fig. 5). Significant heterogeneity could be identified among the studies.

Laparoscopically completed versus converted cases—Morbidity rates.
Morbidity was further analyzed to leak and wound infection rates. Leak rates were reported by eight studies.14,24,27,28,30–33 The conversion group displayed leak rates ranging from 4% to 21.4%. On the other hand, the laparoscopic group's leak rates ranged from 7.2% to 19%. Pooling of data revealed a difference favoring the laparoscopic group, which could not reach the level of statistical significance (OR: 1.85 [1.01, 3.37], I 2 : 45%, z: 2.00, P = .05) (Fig. 6). The studies displayed significant heterogeneity. Wound infection was reported by four studies.24,27,32,33 Wound infection rates ranged from 8% to 23.07% for the converted cases and from 0% to 12.04% for the laparoscopic group. Pooling of data revealed a difference favoring the laparoscopic group with no heterogeneity among studies (OR: 3.01 [1.82, 5.00], I 2 : 0%, z: 4.27, P < .0001) (Fig. 7).

Laparoscopically completed versus converted cases—Leak rates.

Laparoscopically completed versus converted cases—Wound infection rates.
Data on reoperation rates could be identified in six studies.24,27,28,30,31,33 The conversion group displayed rates ranging from 0% to 14.3%, while the laparoscopic group's reoperation rates ranged from 1.1% to 17.6%. Pooled data were analyzed and did not show any difference between the two groups or any heterogeneity among studies (OR: 0.91 [0.52, 1.61], I 2 : 0%, z: 0.31, P = .75).
Short- and long-term oncological outcomes
Six studies reported data on the total number of lymph nodes harvested.27,28,30–33 Pooling of these data, although significantly heterogeneous, did not reveal any difference between the two groups (Mean diff.: 0.5 [−1.67, 2.67], I 2 : 89%, z: 0.45, P = .65).
Local recurrence rates were reported by six studies.12,24,27,30–32 The rates ranged from 0% to 16% for converted cases and from 1.5% to 6.7% for laparoscopic cases. Pooling of all available data could not identify any difference between the groups (OR: 1.92 [0.88, 4.21], I 2 : 1%, z: 1.63, P = .1). The studies did not display any heterogeneity.
Five studies offered data on distant metastasis rates.12,24,30–32 The conversion group displayed rates ranging from 8% to 26.9%, while the laparoscopic group showed rates ranging from 4.7% to 12.7%. After pooling the data, no significant difference could be revealed between the two groups, but with significant heterogeneity among studies (OR: 1.79 [0.86, 3.19], I 2 : 51%, z: 1.57, P = .12).
Tumor-free survival rates at 60 months were possible to extrapolate by four studies.12,24,30,31 The conversion group displayed rates ranging from 55.3% to 79%, while the laparoscopic group's rates ranged from 58.3% to 89.1%. The meta-analysis of pooled data revealed a statistically significant difference favoring the laparoscopic group (OR: 1.74 [1.14, 2.66], I 2 : 19%, z: 2.58, P = .01). There was no heterogeneity among studies.
Overall survival rates at 60 months were reported by four studies.12,26,30,31 For the converted cases, rates ranged from 62.5% to 91%, and for the laparoscopic cases, they ranged from 70.6% to 87.8%. Pooled data did not reveal any difference between the two groups and the studies did not display any heterogeneity (OR: 0.79 [0.47, 1.33], I 2 : 31%, z: 0.89, P = .37).
Open approach versus conversions
Demographics
Three studies report on patients' age.27,29,32 Pooling of all available data on patients' age did not reveal any statistically significant difference between open and converted cases (mean diff.: 1.75 years [−3.51, 7.00], I 2 : 76%, z: 0.65, P = .51). Included studies displayed significant heterogeneity.
No other demographic data could be meta-analyzed.
Intraoperative outcomes
The duration of the operation was reported by three studies.27,29,30 Pooling of all data showed that converted cases lasted significantly longer than the ones offered the open approach (mean diff.: 53.55 minutes [13.87, 93.22], I 2 : 93%, z: 2.65, P = .008), although there was significant heterogeneity among studies (Fig. 8).

Open versus converted cases—Operation duration (minutes).
Immediate postoperative outcomes
Hospital stay was reported by three studies.27,29,30 Analysis of all available data from all studies could not identify a statistically significant difference between the open and the converted cases (mean diff.: 1.77 days [−0.49, 4.03], I 2 : 0%, z: 1.53, P = .13). No significant heterogeneity could be identified among the studies.
Three studies reported data on mortality.12,29,32 Mortality rates ranged from 0% to 8.3% for the converted cases and from 2.5% to 5.9% for the open group. Pooling of data did not reveal any difference between the two groups (OR: 1.02 [0.26, 3.93], I 2 : 0%, z: 0.02, P = .98). The analyzed studies did not display any heterogeneity.
Three studies had available data on overall morbidity.12,29,30 The conversion group displayed rates ranging from 16.7% to 58.3%, while the open group's morbidity ranged from 29.3% to 44.7%. Analysis of pooled data revealed no difference between the two groups (OR: 1.14 [0.3, 3.86], I 2 : 82%, z: 0.21, P = .84) (Fig. 9). Significant heterogeneity could be identified among the studies.
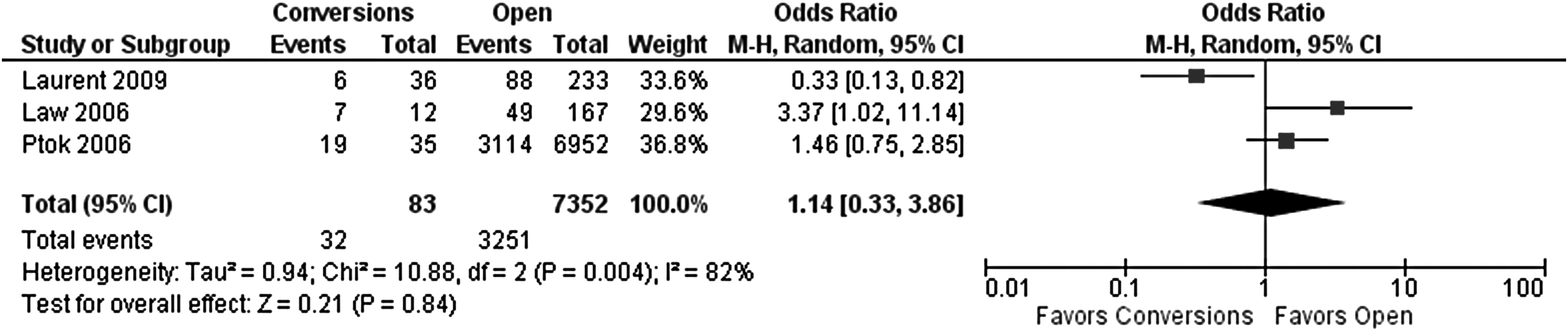
Open versus converted cases—Morbidity rates.
Leak rates were reported by three studies.27,30,32 The conversion group displayed leak rates ranging from 4% to 19.2%. On the other hand, the open group's leak rates ranged from 4.5% to 15.2%. Pooling of data could not identify any difference between the two groups (OR: 0.91 [0.4, 2.06], I 2 : 46%, z: 0.23, P = .82) (Fig. 10). The studies displayed no significant heterogeneity.
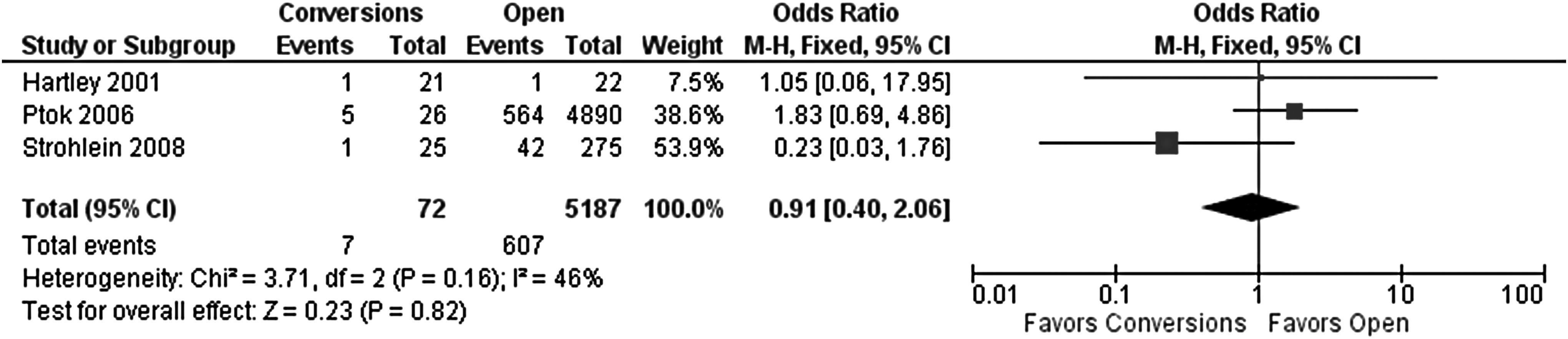
Open versus converted cases—Leak rates.
Short- and long-term oncological outcomes
Local recurrence rates were reported by four studies.12,27,30,32 The rates ranged from 0% to 16% for the converted cases and from 4.5% to 9.5% for the open cases. Pooling of all available data could not identify any difference between the groups (OR: 1.45 [0.69, 3.06], I 2 : 0%, z: 0.98, P = .33). The studies did not display any heterogeneity. No other data on oncological outcomes were available for a meta-analysis.
Three studies offered data on distant metastasis rates.12,30,32 The conversion group displayed rates ranging from 8% to 26.9%, while the open group showed rates ranging from 7.9% to 24.9%. After pooling the data, no significant difference could be revealed between the two groups with no significant heterogeneity among studies (OR: 0.89 [0.48, 1.66], I 2 : 0%, z: 0.35, P = .72).
Discussion
The results of the present review indicate that conversion of the laparoscopic approach to open for the resection of rectal cancer is associated with increased duration of surgery and increased specific morbidity compared with the laparoscopically completed procedures. In detail, although overall morbidity, mortality, and reoperation rates do not differ significantly between the two groups, converted-to-open cases present a marginally increased rate of anastomotic leak, which does not reach statistical significance, and increased rate of wound infection compared with the laparoscopically completed cases. Although explanation for the increased wound infection rate is rather obvious, interpretation of the increased anastomotic complications observed in the converted cases cannot be attributed to any specific factor with certainty; Slim et al. 34 consider surgeon's fatigue and consequent technical compromise as key factors of increased anastomotic leak rate, while others 35 consider extensive surgical manipulation and damage to the vascular supply of the tissue around the anastomosis as possible etiological factors of increased anastomotic complications. Increased specific morbidity translates into an increased duration of hospital stay of the converted versus the laparoscopically completed cases, although this parameter usually may reflect different policies in the postoperative rehabilitation policies between centers.
As far as the oncological long-term outcomes are concerned, numbers of retrieved lymph nodes, local recurrence rate, and overall survival rate are similar between converted and laparoscopically completed cases. In contrast, converted cases present a higher rate of distant metastases and tumor-free survival rate, compared with the laparoscopically completed cases. The latter findings can be attributed to the fact that converted cases present with more advanced stages of disease as a source of selection bias and cannot be attributed to conversions.
The present review also showed that obesity is a main factor for conversion of a laparoscopic approach to open for the surgical treatment of rectal cancer: converted cases presented with a significantly higher BMI than the laparoscopically completed ones. Obesity and also the presence of advanced rectal tumors cause increased technical difficulties, particularly in dissecting the distal rectum to the pelvic floor, transecting the rectum distal to the tumor, and fashioning the anastomosis by the laparoscopic approach,10–12,18,35 thus justifying the higher conversion rate in case of rectal cancer compared with the respective figure for colon cancer.3,10,12–14,16,17 Preoperative radiation or chemoradiation does not seem to have any impact on anastomotic complications since the rate of neoadjuvant treatment does not differ significantly between converted and laparoscopically completed cases.
In addition to the comparison between the laparoscopically completed and the converted cases, the present study reviewed the literature for any differences in the outcomes between converted cases and cases operated upon by the open approach for rectal cancer.
No differences are accounted whatsoever in demographics, immediate postoperative outcomes, and long-term oncological results between the two groups. The only significant difference seen is in the duration of surgery: converted cases last significantly longer than the open ones.
Based on the results of the present review, definite conclusions regarding outcomes of converted cases with rectal cancer cannot be drawn as quality of included studies in the meta-analysis is limited. Lack of randomized trials may signify patient selection and thus higher rates of laparoscopic completion of the procedure as well as lower complication rate in the converted cases. An additional limitation caused by the included studies is the discrepancy in the definition of conversion, which ranges from inability to complete certain stage of the procedure, for example, safe vascular control, proper dissection of the mesorectum, transection of rectum distal to the tumor, or even fashioning the anastomosis by the laparoscopic approach, to a larger than anticipated abdominal wall incision. The latter definition of conversion is vague and does necessarily signify worse outcomes as different sizes of abdominal wall incisions may be associated with different morbidity rates.35,36
Conversion of a laparoscopic colorectal procedure to open could be considered either as a complication of the approach with distinct clinical outcomes or a limitation to safety of completing the procedure by the laparoscopic approach and rational on-table judgment. 35 The latter view is supported by the fact that early or pre-emptive conversion to open is not associated with increased complication rates.35,37 Unfortunately, due to lack of reported timing of conversion by most of the included studies, this hypothesis could not be tested by the present meta-analysis.
It has been suggested that high conversion rates are the result of inadequate surgical experience or of low volume of cases, and that by improving surgical expertise and performing large number of cases, conversion rates are expected to reduce. However, according to available evidence, neither surgical experience nor high-volume laparoscopic colorectal surgery can be considered as predictive factor for conversion.18–23,35,38–40 Thus, conversion remains a disadvantage of the laparoscopic approach, expected to decrease in case of significant technical improvements in instrumentation; that is, innovation of a device that achieves a technically perfect and safe transection of the rectum at the level of the levator ani deep in the pelvis. Until then, laparoscopic resection of rectum can be offered to selected patients (i.e., nonobese, with rectal tumor of limited size) in whom conversion rate is expected to be low. Alternatively, a hybrid approach could be adopted: completion of the intraperitoneal stage of the procedure and possibly dissection of the rectum by the laparoscopic approach and completion of the procedure by an on-purpose and pre-emptive conversion to open, through a small and low abdominal wall incision, for the transection of distal rectum. Of course, this hypothesis should be tested within the frame of clinical trials.
In conclusion, conversion to open of a laparoscopic procedure for the resection of rectal cancer seems to be associated with longer duration of operation, increased rates of wound infection, nonsignificant increase in anastomotic complication, and more prolonged hospital stay in comparison with the laparoscopically completed cases. Patients to be converted to open are those with increased BMI and advanced stage of the disease. Advanced stage seems to be associated with increased rate of metastasis and reduced tumor-free survival. The only difference in the outcomes between converted and open cases is the increased duration of surgery in the former group of patients. Pre-emptive conversion may reduce complication rates.
Footnotes
Disclosure statement
No competing financial interests exist.