
Abstract
Abstract
Objective:
The authors present a multicenter retrospective series of different benign rib lesions in children operated on using thoracoscopy.
Materials and Methods:
Between 2005 and 2015, 17 rib resections were performed thoracoscopically, in four French departments of pediatric surgery. Of these 17 cases, 13 exostoses, 2 endochondromas, 1 synostosis, and 1 Cyriax's syndrome were noted. Inclusion criteria were benign tumors or rib anomalies such as synostosis, in children younger than the age of 18 years, and thoracoscopy. Open surgery and malignant tumors were excluded. Thoracoscopy was put forward using one optical port as well as one or two operative ports.
Results:
Ten patients presented with chest pain, dyspnea, or unexplained cough. Six tumors were incidentally diagnosed. One patient presented with a chest wall deformation. Single-lung ventilation was required in 2 cases. In 1 case of endochondroma, a segmental rib resection was performed, leaving a part of the periosteum and the intercostal vessels and nerve. In this case, rib resection was performed using an endoscopic shaver drill system. As for the other cases, a simple resection of the tumor or of the bridge between two ribs (synostosis) was performed. In these cases, a Codman Kerrison laminectomy rongeur was used. There was no complication during or after surgery. Nevertheless, 2 years after surgery, pain did not disappear in 1 case, probably due to a definitive intercostal nerve damage.
Conclusion:
Benign rib lesions in children are rare. Thoracoscopy may be offered to reduce the functional deleterious consequences of an open surgery. It may be put forward especially in case of hereditary multiple exostoses where redo procedures may be required.
Introduction
R
Multiple costal anterior sections were put forward to prepare and facilitate a Nuss procedure for pectus excavatum. 3 Thoracoscopic cartilage resection with partial perichondrium preservation was proposed in the presence of a unilateral pectus carinatum. 4
Lesions such as synostosis, exostosis, enchondroma, or other benign tumors in children may be treated thoracoscopically. Only 13 isolated cases were reported in pediatric surgery.5–10
The objective was to present a French multicenter series of benign rib lesions in children operated on with thoracoscopy. Indications, the surgical approach, and technical details are discussed.
Materials and Methods
Over the last 10 years, 17 rib resections for benign tumors were performed thoracoscopically in four French departments of pediatric surgery. The patients were placed in a lateral supine position. Port setup depended on the localization of the tumor. The operative technique, pathological findings, and clinical follow-up were recorded. A survey was sent to all departments of pediatric surgery in France. Inclusion criteria were benign tumors or rib anomalies such as synostosis, in children younger than the age of 18 years and thoracoscopy. We excluded thoracotomy and malignant tumors. Epidemiological, clinical, radiological, and surgical data were collected.
Results
Patients were girls in 10 cases and boys in 7 cases. Medium age was 11.9 years (range: 2.8–17). Thoracoscopy was offered in 17 cases for benign tumor resection: 12 exostoses (Figs. 1 and 2), 2 enchondromas, in 1 case for a partial rib resection in case of a Cyriax's syndrome (eighth and ninth right ribs), in 1 case for a synostosis, removing the bone bridge between two ribs (Table 1: case No. 13), and in 1 case for a segmental rib resection (enchondroma) (Figs. 3 and 4), keeping a part of the periosteum and the intercostal vessels and nerve (Table 1: case No. 8).
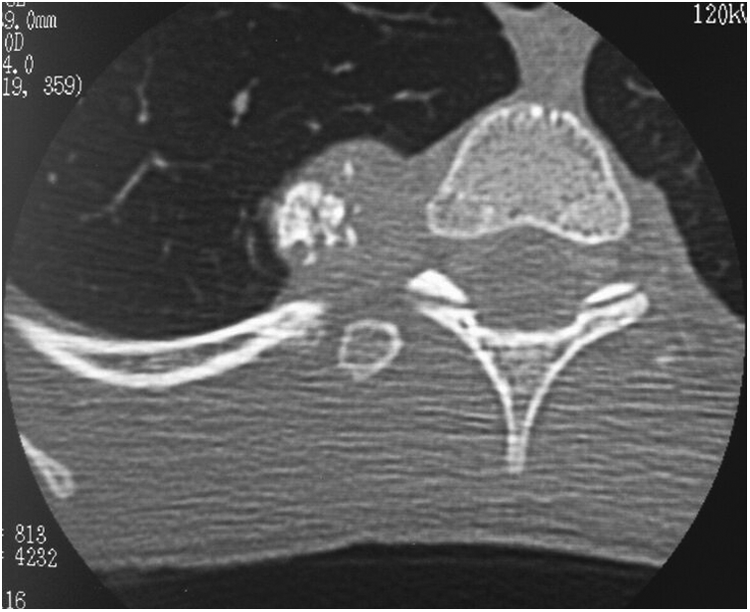
Example of CT scan of exostoses.
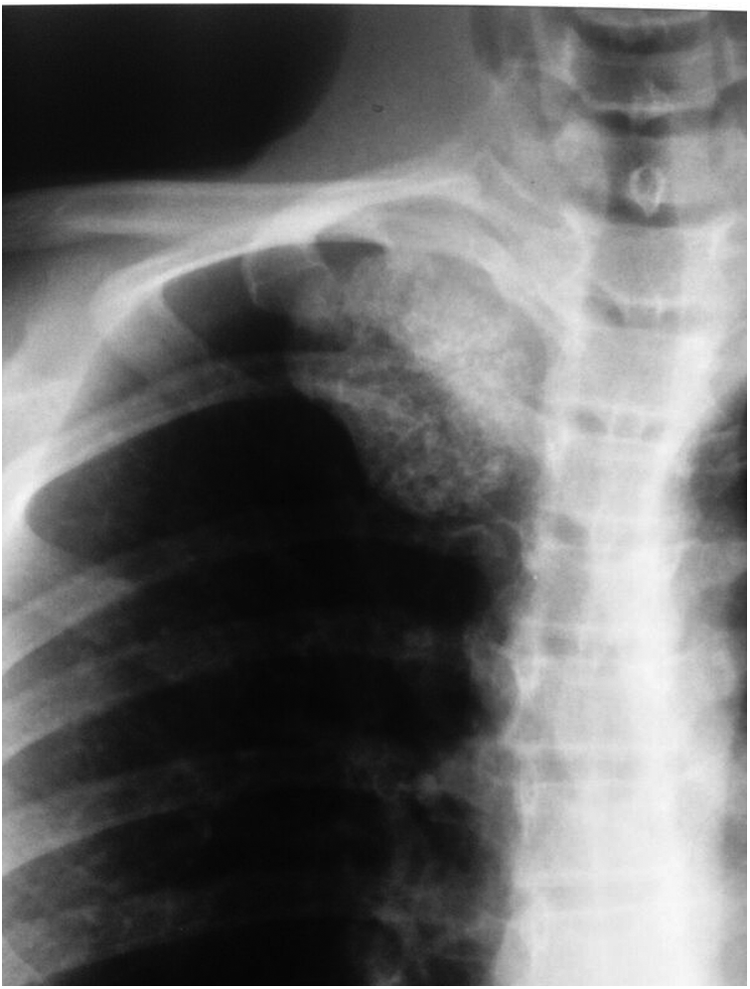
Example of X-ray of exostoses.
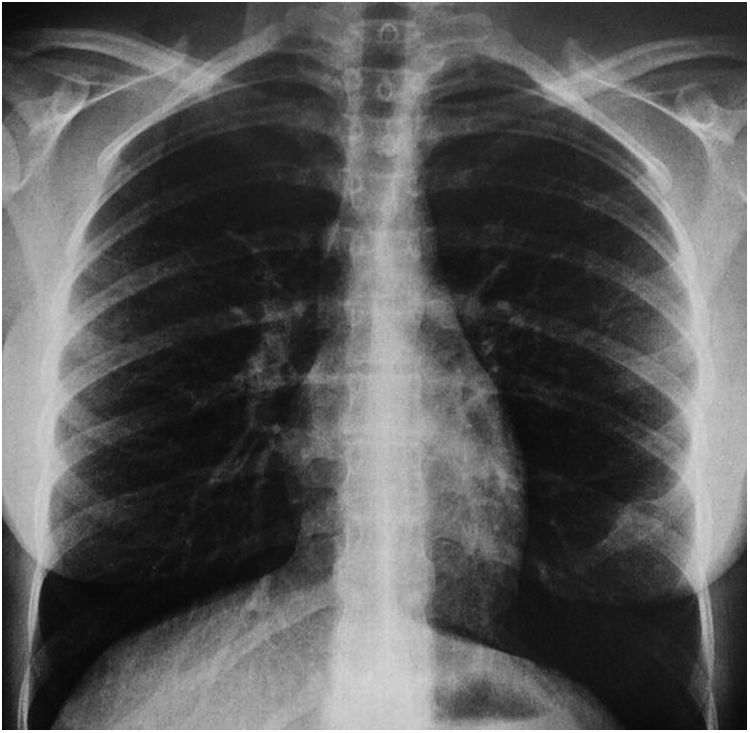
X-ray of case No. 8.

CT scan of case No. 8.
In 8 cases, a 30° camera was used and a 0° camera was used in 9 cases. In addition, in 15 cases, there were three ports, whereas two ports were used only in 2 cases. The insufflation of the pleural cavity with a low flow (1.5 L/min) and a low pressure (4 mmHg) is sufficient in most cases. However, the use of a bronchial blocker was necessary to facilitate the surgical procedure in 2 cases. The resection was performed primarily with an endoscopic rongeur in 15 cases, whereas an endoscopic shaver was used in 1 case (case No. 8). For all cases except 1 (case No. 8), there was no need for rib stabilization. Indeed, the resection targeted the tumor and a part of the rib. In case No. 8, the 6 cm segmental resection preserved the periosteum, and it was unnecessary to perform any osteosynthesis. We never had different tumors on successive ribs.
Average operative time was 78 minutes (range: 40–165 minutes). Total hospital stay, including surgery and postoperative stay, was 4.4 days (range: 2–9 days).
In 3 cases, the diagnosis of rib exostosis was established via general screening among patients known to have hereditary multiple exostoses (HME), and in 3 cases HMEs were found incidentally on a chest X-ray. Two patients presented with acute hemothorax. Neither patient had any history of exostosis (cases No. 11 and 12). Eight patients presented with nonexplained, nonconstant chest pain and on/off dyspnea during efforts or coughing. One patient (case No. 13) had a parietal wall deformation due to a congenital synostosis.
Symptoms disappeared after surgery for all patients, minus one (case No. 3), probably due to a definitive damage of one intercostal nerve, which prolonged the hospital stay. In case of multiple resections or previous hemothorax or previous respiratory symptoms (dyspnea), postoperative drainage, and physiotherapy made the hospital stay longer.
In our series, none of the patients suffered from intraoperative or postoperative complications. In addition, in 3 patients, previously nondetected lesions were discovered during surgery and resected simultaneously.
In case of HME, patients were followed up every year with clinical examination, chest-X-ray, and magnetic resonance imaging (MRI) if necessary. For isolated exostosis, an X-ray performed 1 year after surgery was generally considered sufficient, even if the lesions were not totally removed.
Discussion
Benign lesions of the rib cage are rare and account for 5% to 7% of all primary bone tumors.11,12 There are a variety of benign bone lesions which can occur in the ribs, the most common one being fibrous dysplasia (30% of all benign rib tumors) followed by enchondroma and osteochondroma, respectively. 11 In addition to the ones previously mentioned, aneurysmal bone cysts, osteoid osteomas, osteoblastomas, giant cell tumors, cystic angiomatosis, and eosinophilic granuloma are other benign rib lesions which can occur. 11 Osteochondromas are common benign bone tumors. However, they only account for 8% of rib tumors.12,13 Seventy percent of osteochondroma in the ribs and vertebras are described in patients who suffer from HME. 14 Osteochondromas had the highest prevalence of all other benign tumors (37.5%). 1 Likewise, our series showed a predominant prevalence of osteochondroma.
The clinical presentation of benign rib lesions is variable. Local symptoms may arise because of their size as they can compress a nerve or a vessel, interfere with a joint, or be visible externally as a form of swelling on the external thoracic wall.15,16 Symptoms are highly dependent on the location of the lesion. A first rib osteochondroma presented an axillosubclavian vein thrombosis in the context of venous thoracic outlet syndrome in a 12-year-old girl, whereas the presentation was painful dorsal scoliosis in another boy.17,18 Likewise, benign rib lesions may be totally asymptomatic, present as pleuritic chest pain (chronic or acute), a cough, as a lump on the rib cage, present as hiccups, or they may be detected coincidentally on a chest X-ray.5,9,10,16 More serious presentations can be associated with benign rib lesions, which involve spontaneous pneumothorax, spontaneous hemothorax, pleural effusion, diaphragmatic rupture, and bowel obstruction, pericardial effusion, requiring urgent medical attention.5,14,19,20 The constant rubbing between a rib lesion and the pleura caused by respiration can cause chronic inflammation, then pneumothorax due to a lesion of the lung parenchyma, or hemothorax due to a damage of any vessel. 10
Enchondromas have a 25% rate of malignant degenerations whereas osteochondromas have less than a 5% transformation rate to chondrosarcomas.5,21 In our series, none of the patients suffered from endochromatosis. However, some did suffer from HME.
Plain film chest radiography should be the initial approach to suspected rib lesions as it may identify masses, bony erosions, pulmonary infiltration, and lymphadenopathy among other signs.22,23 Although previous plain chest X-rays are not very helpful to identify the exact location of rib lesions, a computer tomography (CT)-scan is always recommended to localize such lesions, study their morphology, look at their neighboring structures, and potentially help to plan surgical excision among other benefits. 10 Magnetic resonance is becoming more popular nowadays, and it has the added benefit of precisely showing the extent of the cartilage cap, which is not seen on either CT-scans or plain films, thereby improving our understanding of the relationship of the lesion with its surrounding vital structures. 17 Clinicians should consider MRI for patients with a need for repeated imaging in the context of HME to prevent high-dose radiation. 10 Benign lesions which can be assuredly diagnosed on imaging and other preoperative workup do not require to undergo needle biopsy and can proceed directly to excision if deemed so, for both therapeutic and diagnostic purposes. 1
Both conservative and surgical options are described for benign rib lesions, namely using thoracoscopy or open thoracotomies.5,10
The conservative approach is reported in the literature. However, careful care is warranted before choosing this option. Inward protrusions into the thoracic cavity can cause lethal visceral injury and entail acute presentations in patients. Such inward projections have been reported to cause hemothorax, diaphragmatic lacerations, and pericardial lacerations among other complications; hence, conservative management is not advised for such lesions.7,24,25 In addition, patients who suffer from HME and who are treated conservatively, should be followed more vigorously with serial imaging given the nature of their condition and the risk of malignant transformation. 10 Malignant transformation should be immediately suspected if a lesion keeps growing after puberty or if the patient starts complaining of a local pain. 10 Indications for surgical management are numerous. Symptoms, position, and projection (inward protruding lesion), associated skeletal deformity, treatment of intrathoracic injuries caused by the rib lesion, lesions becoming allusive of malignant transformation, cosmetic reasons, and diagnosis of benign lesions are all indications for surgical management.10,14,18,26
In addition, surgical resection is practiced differently depending on the different benign rib lesions where an osteochondroma will only necessitate a simple resection, some enchondroma end up being resected with a part of the rib as in case No. 8.24,26,27
In our series, all 17 patients underwent thoracoscopic resections of their lesions. To our knowledge, in the literature, there are 12 other cases reported with benign rib lesions operated thoracoscopically. The use of a bronchial blockers may be valuable to widen the operative field. 28 However, it seems to be rarely required in our series with only 2 cases. The insufflation of the pleural cavity with a low flow (1.5 L/min) and a low pressure (4 mmHg) is sufficient in most cases. The ports have to face the lesion during their setup. Difficulties may occur in case of multiple lesions.
Most often, Codman Kerrison laminectomy rongeurs are used. Once in our series (case No. 8), an endoscopic shaver drill system was used to cut the rib on both sides and far from the tumor. Cold serum saline was instilled toward the tip of the shaver to prevent burning the tissues around as in arthroscopy.
In the adult literature, the use of a Gigli saw has been described29,30: “the border of the rib lesion was marked with needles and two ports were placed anterior and posterior to the lesion. A submuscular tunnel was created between the two port incisions in order to preserve the overlying muscle and myocutaneous layers. The rib was then divided through these port incisions.” 30
A question remains regarding the use of thoracoscopy for the removal of exostosis—little fragments of the exostosis may be spread accidentally and left in the pleural cavity. In the literature, we never found any remarks about this possible issue. Nevertheless, one should pay attention to this. A control must be performed at the end of the procedure.
Minimally invasive surgery seems to be the best option for surgical indications in case of exostosis. Sometimes, surgery has to be performed to treat a complication; even in case of bleeding, thoracoscopy was a good approach. In case of pain or respiratory difficulties, or to prevent a complication due to a big lesion that was incidentally discovered, the minimally invasive procedure is appropriate with a good final functional result. In case of HME, redo thoracoscopy may be easily offered.
Limitations of the study are as follows: retrospective study, different approaches for operative indications, technical details, and the low number of cases. However, it is the first large study in pediatric surgery literature. This survey did not aim to be compared with open resections. It would be worth of interest to compare the quality of thoracoscopic versus open resections. Do we have more insufficient resections, more recurrences due to the thoracoscopic approach? The main difference is that we could avoid a thoracotomy, and especially so in HME patients who can require multiple metachronous resections.
Conclusion
The removal of a benign rib tumor using thoracoscopy is feasible. When including our French series, there will be 29 cases reported in the literature without any major complications and immediate good results. Long term results are unknown, especially regarding exostosis: is thoracoscopic resection using rongeurs sufficient or insufficient? There are no answers in the published data, and the follow-up of our series is too short. It is also feasible to remove a part of the rib without any damage to intercostal vessels and to the nerve. The Codman Kerrison laminectomy rongeur is probably the best device for exostosis. However, the use of an endoscopic shaver drill system makes partial removal of a rib very precise and atraumatic for the periosteum, intercostal vessels, and nerve.
Footnotes
Disclosure Statement
No competing financial interests exist.