
Abstract
Abstract
Background:
A significant gap presently exists between box-lap and virtual-reality simulators and live surgery. Live animal and cadaver use has significant downsides. We have developed a high fidelity, real tissue simulator that allows training in laparoscopic foregut operations.
Methods:
Our foregut surgery model is based on porcine tissue blocks that include lungs, heart, aorta, esophagus, diaphragm, stomach, duodenum, liver, and spleen. The tissue block is mounted in a human mannequin and perfused with artificial blood. The anterior abdominal wall is constructed so as to allow for laparoscopic or robotic surgical training. We sought to test the model with procedures performed by expert surgeons. After completing the procedures, face validity was measured by surgeon responses to a questionnaire defining the perceived relationship to real surgery.
Results:
Five expert foregut surgeons performed laparoscopic Heller myotomy, Nissen fundoplication, and sleeve gastrectomy on the model. The simulator was rated as highly realistic in terms of tissue feel, instrument usage, and conduct of the operation for all three procedures. In addition, all surgeons felt the model could significantly shorten the learning curve for performing these procedures.
Conclusions:
The results of this study show that our simulation model, based on animal tissue blocks, offers a very realistic representation of laparoscopic foregut operations, thus achieving a high level of face validity. The model should be very useful for training surgeons in laparoscopic foregut procedures.
Introduction
S
Current surgical simulators available include box-trainers, virtual-reality simulators, human cadavers, and live animals. Box-lap trainers can only simulate a variety of basic skills, including laparoscopic suturing, knot-tying, and coordination drills. 5 While virtual-reality simulators offer high-fidelity training that can replicate entire operations, most of them lack haptic feedback with the use of surgical instruments, and they have a very high initial cost of system acquisition. 6 Although cadavers most closely approximate reality, they are infrequently used because of their cost and limited availability. 7 The use of live animals offers realism and opportunities to mimic many operations. However, their use is problematic because of ethical concerns, high costs, and the need for specialized facilities. 8
The objective of our simulation laboratory was to design a high-fidelity surgical simulator for foregut surgery, able to offer high quality training without the drawbacks of current simulation tools. The aims of this study were to (1) describe our laparoscopic surgical simulator, and (2) evaluate the model by surgeon responses to a questionnaire.
Methods
The simulation model is based on porcine tissue blocks that include lungs, heart, aorta, esophagus, diaphragm, stomach, duodenum, liver, and spleen. Tissue is preserved in an alcohol-based solution that retains fresh tissue characteristics for several weeks (945 cc of 200 proof ethanol into 2840 cc of water). We perform anatomical modifications to the block, to counteract the pig's anatomy differences as compared to humans: the liver and the spleen are reduced in size to simulate a human anatomy, and part of the thick muscular portion of the diaphragmatic pillars is resected to mimic a human diaphragmatic hiatus.
The abdominal aorta is cannulated and the tissue block is perfused with artificial blood (Crime scene thine blood; Manhattan Wardrobe supply). The tissue block is then mounted in a human mannequin (Fig. 1). The anterior abdominal wall is constructed with a Smooth-On product (Dragon Skin FX-Pro) that is poured into a thin sheet about ¼” thick and attached to the mannequin with marine grade snaps to secure it in place. The thickness of the silicone also allows for the placement of laparoscopic trocars so as to allow laparoscopic or robotic surgical training. The room is finally set up the same way as the OR to simulate a clinical environment (Fig. 2).
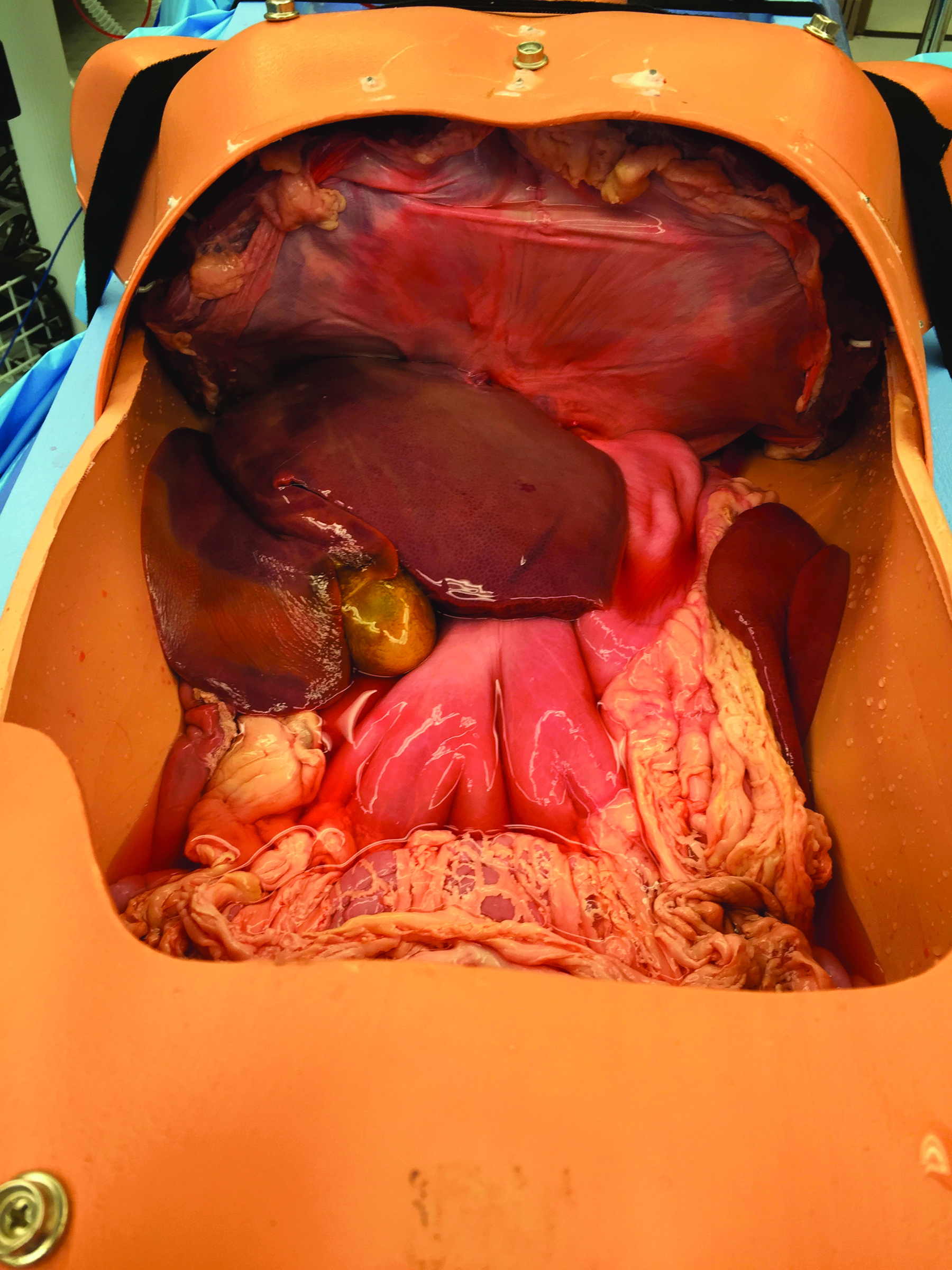
Perfused tissue block mounted in a human mannequin.

Simulation room set up as an operating room.
We sought to test the model with procedures performed by surgeons whose daily practice is mostly based on laparoscopic foregut surgery. After completing the procedures, face validity was measured by surgeon responses to a questionnaire (Likert scale based) defining the perceived relationship to real surgery. The questions were anonymously answered by all the participants after performing the procedures.
Results
The initial cost of the simulator is $400 (mainly represented by the male torso mannequin, silicone-based abdominal wall, tissue block, and artificial blood). The laparoscopic instruments do not represent any additional cost, since they are all disposable instruments that are washed after usage. Once the initial expenses are covered, the simulator cost is $50 for each surgical training session (tissue block+artificial blood).
Five surgeons whose laparoscopic foregut surgery represents 90% of their practice performed three different procedures on the simulator during a full-day training trial in our simulation laboratory (Fig. 3):
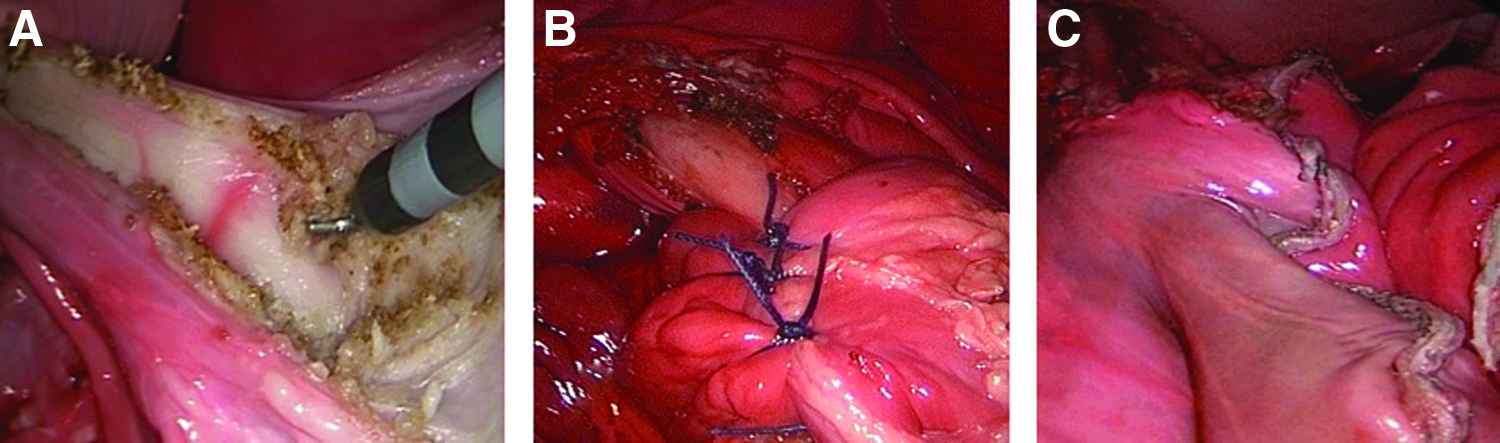
Laparoscopic procedures performed with the simulation model:
(1) Laparoscopic Nissen fundoplication: The gastrohepatic ligament was divided to the right pillar of the crus. The peritoneum and the phreno-esophageal membrane overlying the esophagus were transected and the left pillar of the crus was then separated from the esophagus. The short gastric vessels were divided, starting midway along the greater curvature of the stomach toward the left pillar of the crus. The posterior and anterior vagus nerves were clearly identified and preserved. A window was created between the stomach, left pillar of the crus, and esophagus.
A Penrose drain was placed around the esophagus, also incorporating the anterior and posterior vagus nerves. The right and left pillar of the crus were approximated using nonabsorbable sutures, placed posterior to the esophagus. The stomach was passed behind the esophagus and a shoe-shine maneuver was performed to verify sufficient fundic mobilization. A 360° fundoplication was created by placing three stitches of nonabsorbable material at 1 cm intervals to approximate the right and left side of the fundoplication.
(2) Laparoscopic Heller myotomy: The gastrohepatic ligament was divided to the right pillar of the crus. The peritoneum and the phreno-esophageal membrane overlying the esophagus were transected and the left pillar of the crus was then separated from the esophagus. The short gastric vessels were divided, starting from a midway along the greater curvature of the stomach. A myotomy was performed on the right side of the esophagus in the 11 o'clock position using a hook cautery. The myotomy was extended proximally for about 6 cm above the gastroesophageal junction, and distally for 2.0–2.5 cm onto the gastric wall. After the myotomy, an anterior 180° fundoplication was created with two rows of nonabsorbable material.
(3) Laparoscopic sleeve gastrectomy: The short gastric vessels were divided, starting from a midway along the greater curvature of the stomach. Once the fundus was mobilized, the dissection proceeded toward the pylorus. The antrum was stapled first starting 2–3 cm proximal to the pylorus. The choice of staple cartridge was green in the first case. However, due to the thickness of the gastric wall of the pig, the following 4 surgeons used black cartridges. The final cartridge was placed at least 1 or 2 cm from the gastroesophageal junction (total of six cartridges). The staple line was sutured with nonabsorbable material.
All the participants thought that the model was very realistic in terms of operative space, haptic feedback during suturing, and haptic feedback while using energy instruments, and fairly realistic in terms of organs size and shape. Vascularization of the tissue was evaluated as fairly realistic by 2 surgeons, while the other three stated as neutral.
All the surgeons strongly agreed that this model should replace the use of live animals, it is an excellent training tool for surgical residents, and it could shorten learning curve and improve operative outcomes. In addition, most of the participants believed that performing the procedure was as real as in the OR, and that this model could be a useful tool also for trained surgeons (Table 1).
Discussion
Shorter workweek for residents and increasing emphasis on OR efficiency have dramatically diminished the available teaching time in the OR. In addition, the increasing number of legal litigations and complexity of cases have reduced faculty's ability to assist residents in the OR. In this scenario, simulation training has evolved as an important component of surgical education. We aimed to design a simulation model for laparoscopic foregut surgery, and experienced surgeons tested the simulator with optimistic evaluations.
Most of the simulation programs of laparoscopic training are focused on teaching basic laparoscopic skills.9,10 Box-lap trainers provide a relatively easy and cheap simulation model to acquire basic psychomotor skills needed to perform minimally invasive surgery, and remain an interesting tool for novice learners 5 . In contrast to box-trainers, virtual-reality simulators have the capacity to train both basic skills and simulate full procedural surgical tasks. 11 In fact, previous reports have shown that residents who received virtual-reality training made fewer errors and had higher economy of movements during a laparoscopic cholecystectomy, as compared to residents without such training.12,13 However, their ability to train in more complex laparoscopic operations, such as foregut procedures, is limited.
The use of cadavers represents the only “true” anatomy simulator currently, with the highest possible fidelity available to practice entire operations. Nevertheless, their cost, availability, tissue compliance, infection risk, and inability to simulate complications such as bleeding outweigh the advantages of cadaver models. Live animal models, on the other hand, provide access to a wide variety of procedures and allow training in realistic conditions. Porcine models, in fact, have proven to be an adequate tool to learn complex laparoscopic procedures.14,15 Drawbacks of using live porcine models include anatomical differences with humans, and high costs due to their housing and handling requirements. In addition, they are not universally available because of ethical or national legal restrictions.
Our porcine tissue block simulator, has a similar surgical anatomy as compared to humans, is mounted in a space comparable to a human abdominal cavity, and it is perfused with artificial blood, offering a valuable training tool. All surgeons believed the model was realistic in terms of operative space, organs size and shape, and haptic feedback while using laparoscopic instruments. Moreover, all agreed that the model is an excellent training tool for surgical residents, and should replace live animals models.
Foregut procedures, such as laparoscopic antireflux surgery (LARS), can be considered advanced laparoscopic operations requiring suturing and knotting under tension in multiple planes with two-dimensional visual feedback. LARS, as compared to open surgery, is associated with better perioperative outcomes, and lower costs for the healthcare system. 16 A learning curve of 20 procedures per surgeon was established previously for LARS, showing significant higher rates of complications during the first 5 individual cases.17,18
We believe acquiring technical skills such as dissection of the posterior window behind the esophagus, closure of the diaphragmatic crura, and suture of the fundoplication with a high-fidelity simulator may shorten the learning curve of LARS. Botden et al. developed a simulator for LARS with artificial organs and tissue placed in a box trainer. 19 Participants considered the artificial stomach unrealistic for making an adequate wrap because it was too rigid and thick. In addition, it was not possible to simulate dissection of tissue with the artificial model. 19 Our model, in contrast, allows to perform all the critical steps of the operation with a realistic tissue feel and instrument usage, in the setting of an abdominal cavity. In addition, with our model trainees are able to perform additional procedures such a Heller myotomy or sleeve gastrectomy.
Surgical training generally occurs on individual basis. In practice, however, operations are conducted by a multidisciplinary team in the OR. Simulated OR environments offer training in both technical skills and teamwork, promoting cooperation and reducing the number of communication errors. 20 While teamwork-based training has been well recognized in emergency and trauma procedures, team simulation has not been advocated for laparoscopic surgery.21,22 With our model set up in the simulated OR, we are able to train the complete surgical team: surgeon (performing the operation), assistants (camera, retraction maneuvers), and nurses (knowledge of instrumental usage during different steps of the operation).
Surgical simulation is expensive and its cost constitutes a barrier for the universal embracement of simulation in surgical training programs. 23 In fact, simulation remains an uncommon component of surgical education in low- and middle-income countries.24,25 One of our main goals was to design an economic simulator to allow training surgeons in laparoscopic foregut procedures worldwide. Our model consists of a porcine tissue block mounted in a human mannequin covered with an artificial abdominal wall, and perfused with artificial blood, which all represent very low expenses. Cost effectiveness and return-on investment studies of surgical simulation training are needed to convince hospital and university administrators to invest in simulation.
Our study has several limitations. The model was tested by only 5 surgeons, and further experienced evaluators are needed to confirm the high fidelity of the simulator. It is uncertain whether skills acquired with our foregut simulator will directly transfer to the operative setting, and future validation studies are mandatory. As the participants of the study considered that the vascularization of the tissue was not highly realistic, we are currently working with smaller cannulas to perfuse small vessels in addition to the abdominal aorta to enhance the perfusion of the tissue.
In conclusion, The University of North Carolina foregut model represents a promising simulator to train in LARS, Heller myotomy, and sleeve gastrectomy. The model was regarded as an excellent training tool for surgical residents by all the participants of the study. Further validation studies are needed to assess if skills acquired by using our surgical simulator are transferable to the clinical setting.
Footnotes
Disclosure Statement
No competing financial interests exist.