
Abstract
Abstract
Background:
Laparoscopic cholecystectomy (LC) is the treatment of choice for mild and moderate acute cholecystitis. The aim of this study was to analyze the utility of C-reactive protein (CRP) as a predictor of difficult laparoscopic cholecystectomy (DLC) in patients with acute cholecystitis.
Materials and Methods:
We conducted a prospective study. All patients included were treated with emergency LC. Patients were analyzed as DLC and nondifficult laparoscopic cholecystectomy (NDLC). Multiple logistic regression and receiver-operating characteristic curve analysis were employed to explore which variables were statistically significant in predicting a DLC. Two different models were analyzed.
Results:
A total of 66 patients were included (37.9% DLC versus 62.1% NDLC). Ideal cutoff point for CRP was calculated as 11 mg/dL, with sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) for predicting DLC being 92% (95% CI 75–97.8), 82.9% (95% CI 68.7–91.5), 76.7%, and 94.4%, respectively. In the first model multivariate analysis, age >45 years, male sex, gallbladder wall thickness ≥5 mm, and pericholecystic fluid collection were significant predictors of DLC, with an area under the curve (AUC) of 0.89. In the second model multivariate analysis, only CRP ≥11 (odds ratio, OR = 17.9, P = .013) was significant predictor of presenting DLC, with an AUC of 0.96.
Conclusions:
Preoperative CRP with values ≥11 mg/dL was associated with the highest odds (OR = 17.9) of presenting DLC in our study. This value possesses good sensitivity, specificity, PPV, and NPV for predicting DLC in our population with acute calculous cholecystitis.
Introduction
T
Previous studies have identified predictors for DLC, these predictors are as follows: male sex, advanced age, acute and chronic cholecystitis, obesity, liver cirrhosis, adhesions from previous upper abdominal surgery, emergency cholecystectomy, large liver and big gallbladder (GB), GB carcinoma, anatomic variation, biliodigestive fistula, and surgical experience. 4 Thus, detecting patients at risk is of paramount importance for planning and counseling.
There are some existing scores that evaluate the risk of conversion from laparoscopic to open surgery,5–9 but few scales that predict DLC.2,10,11 In the majority of previous studies, they included mixed patients with acute and chronic cholecystitis or with another associated disease such as pancreatitis, cholangitis, and common bile duct stones. 2 CRP has already been studied as a predictor for conversion from laparoscopic to open surgery.5,12,13
The aim of this study was to analyze the utility of CRP as a predictor of DLC in patients with acute calculous cholecystitis.
Materials and Methods
We conducted a prospective observational study in which we included patients with acute calculous cholecystitis who required emergency LC.
The study was performed at Gea Hospital in Mexico City, from March 1, 2015, to February 28, 2016. This study was approved by the institutional research and ethics board of our hospital.
Patients >18 years with confirmed diagnosis of acute calculous cholecystitis (grade I or II) according to Tokyo guidelines criteria 1 were included. All patients provided written informed consent before participation. Exclusion criteria included any state of immunosuppression, uncontrolled comorbidities (diabetes, autoimmune diseases, and liver failure), previous ingestion of antibiotics, anticoagulants or anti-inflammatories, and pregnancy. We also excluded patients with any other acute biliopancreatic disorder (cholangitis, pancreatitis, common bile duct stones, or Mirizzi syndrome).
All patients were treated with emergency LC (<12 hours from diagnosis to surgery) by the same surgical team specialized in advanced laparoscopic procedures.
Baseline variables included age, sex, body mass index (BMI) kg/m2, comorbidities, and previous abdominal operations. Clinical data included fever (≥38.3°C), Murphy's sign, tender right upper quadrant (RUQ), and palpable mass in the RUQ. Preoperative laboratory analysis included total leukocyte count (μL), liver function test, amylase, and CRP in mg/dL. Ultrasound findings of gallstones, thickening of the GB wall, GB dimensions, pericholecystic fluid collection, and intramural gas were assessed. Intraoperative information included operative times, estimated blood loss, intraoperative complications (bleeding and bile duct injury), presence of severe inflammation or dense adhesions, type of cholecystectomy required (complete or subtotal), and need to conversion.
We classified intraoperatively the grade of noncomplicated or complicated cholecystitis. Noncomplicated cholecystitis included edematous and GB hydrops, whereas complicated cases included empyema of the GB, necrotizing and perforated cholecystitis, and pericholecystic abscess.
We defined DLC as that that required >120 minutes of total operative time or >40 minutes to achieve critical view of safety (CVS), 14 was associated with technical difficulties or complications (bleeding), or required conversion to open procedure. Patients without these characteristics were classified as nondifficult laparoscopic cholecystectomy (NDLC). Patients were divided according to this definition into two groups: DLC and NDLC. Variables were analyzed between the two groups.
We summarized data as means (standard deviation), medians (interquartile range), or percentages. The chi-square and Fisher exact test were used for categorical variables and the Student's t test or the Mann–Whitney U test for continuous variables depending on distribution. All statistical tests were two tailed and a value of P < .05 was considered statistically significant. The data were analyzed using SPSS version 18.0 for Windows (SPSS, Inc., Chicago, IL).
Receiver-operating characteristic (ROC) curve analysis was used to identify a cutoff threshold to CRP value as a predictor of DLC. Sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) of CRP for predicting DLC were determined.
Multiple logistic regression analysis was employed to explore which variables were statistically significant in predicting a DLC. Two different risk-assessment models were analyzed: A-model, including demographics + ultrasound-adjusted data, and B-model, including demographics + ultrasound + laboratory-adjusted data. Odds ratios (ORs) and their 95% confidence intervals (CIs) were calculated from logistic regression. ROC curve analysis with area under the curve (AUC) was obtained.
Logistic regression and ROC curve analysis were analyzed using EpiData version 3.1 (The EpiData Association, Odense, Denmark)
Results
From March 1, 2015, to February 28, 2016, a total of 105 patients required emergency LC. We excluded 39 patients from analysis because of the presence of uncontrolled comorbidity (diabetes and hypothyroidism), had previous ingestion of antibiotics or anti-inflammatories, or had a concurrent biliopancreatic disorder (cholangitis, pancreatitis, Mirizzi syndrome, or common bile duct stones).
We included to the analysis 66 consecutive patients who fulfilled the inclusion criteria. Of the 66 patients, 37.9% (n = 25) were classified as DLC and 62.1% (n = 41) as NDLC.
Table 1 summarizes comparative analysis between both groups regarding preoperative data (demographic, clinical, laboratory, and ultrasound). We found statistically significant differences regarding age (DLC 53.64 ± 14.53 versus NDLC 41.41 ± 15.64 years, P = .02), sex (DLC n = 14 (56%) versus NLDC n = 7 (17%) males, P = .001), presence of comorbidity (DLC n = 9 (36%) versus NDLC n = 4 (9.7%), P = .023), mean value of total leukocyte count (DLC 15.65 ± 3.69 versus NDLC 12.36 ± 3.60 μL, P = .001), mean CRP value (DLC 24.38 ± 9.96 versus NDLC 5.02 ± 5.57 mg/dL, P = .000), GB transverse axis (DLC 45.58 ± 11.25 versus NDLC 36.51 ± 7.80 mm, P = .000), GB wall thickness (DLC 5.24 ± 1.73 versus NDLC 4.21 ± 1.91 mm, P = .032), and presence of pericholecystic fluid collection (DLC n = 7 (28%) versus NDLC n = 1 (2.4%), P = .004).
Values shown in bold signify P < .05.
ALAT, alanine aminotransferase; ALP, alkaline phosphatase; ASAT, aspartate aminotransferase; BMI, body mass index; CRP, C-reactive protein; GB, gallbladder; RUQ, right upper quadrant; SD, standard deviation; Tot bil, total bilirubin.
Intraoperative variables were compared; results are shown in Table 2. DLC group tended to have a higher estimated blood loss 108.9 versus 21.4 mL (P = .000) and longer mean operative time 116.8 versus 69.8 minutes (P = .000). The DLC group was associated with more cases of complicated cholecystitis 92% versus 17% (P = .000), whereas the NDLC group was associated with noncomplicated cholecystitis 83% versus 8% (P = .000). One patient in the DLC group required conversion to open procedure because of dense adhesions and bleeding, so the rate of conversion to open procedure was 4% (1/25) in the DLC group. No biliary duct injury was registered in any group. Five patients in the DC group required subtotal cholecystectomy and none in the NDLC group (P = .006).
Values shown in bold signify P < .05.
GB, gallbladder; SD, standard deviation.
The ROC curve is shown in Figure 1 for CRP values, with an AUC of 0.96. Ideal cutoff point was calculated as 11 mg/dL, with sensitivity, specificity, PPV, and NPV for predicting DLC being 92% (95% CI 75–97.8), 82.9% (95% CI 68.7–91.5), 76.7%, and 94.4%, respectively.
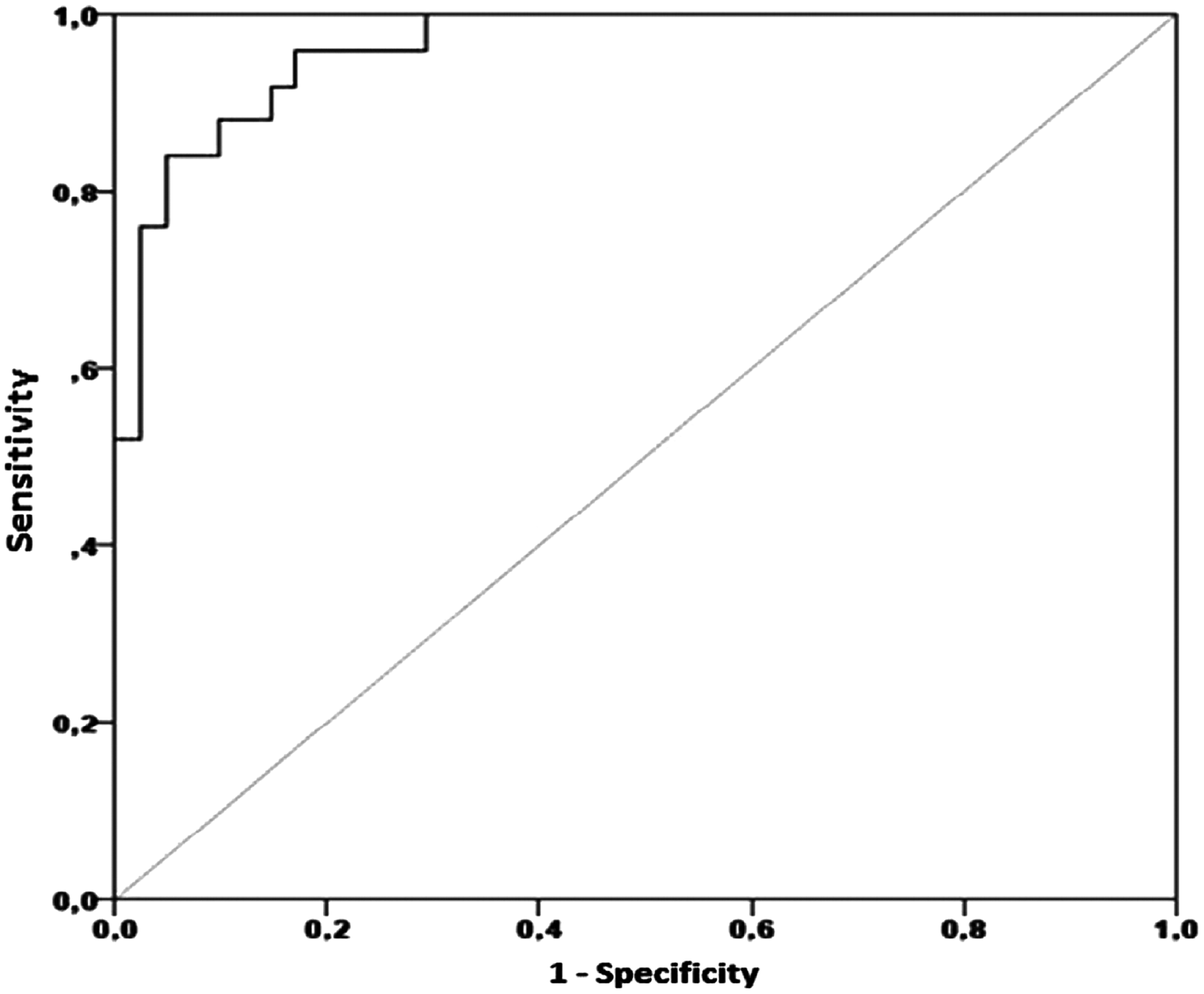
The CRP as predicting factor assessed by ROC curve(area under the curve [AUC] 0.96). CRP, C-reactive protein; ROC, receiver-operating characteristic.
In A-model multivariate analysis, age >45, male sex, GB wall thickness ≥5 mm, and pericholecystic fluid collection were significant predictors of DLC, with an AUC of 0.89 (Table 3). In B-model multivariate analysis, only CRP ≥11 (OR = 17.9, P = .013) was a significant predictor and associated with the highest odds of presenting DLC, with an AUC of 0.96 (Table 3).
Values shown in bold signify P < .05.
CI, confidence interval; CRP, C-reactive protein.
Discussion
LC is the treatment of choice for grade I (mild) or grade II (moderate) acute cholecystitis 1 ; however, the timing for surgery remains controversial. 15 In the past, surgeons argued against early LC in the acute setting and preferred a delayed interval surgery. 16 Recent publications favor early cholecystectomy against delayed surgery, with better results such as less overall morbidity, shorter total hospital stay, reduced cost, and less risk of readmissions.15,17,18 Despite these benefits, early LC for acute cholecystitis is considered related to higher intraoperative difficulties and increased risk of conversion.2,19 Thus, predicting difficult cases represents an important part of the evaluation of patients with acute cholecystitis.
Previous studies focused on the rate of conversion from laparoscopic to open surgery, ranging from 2% to 10%, and the risk factors associated with conversion.5–7 With the development of more advanced laparoscopic skills, conversion rates are now decreasing. This is the reason why recent studies should aim to describe factors that predict difficulties during cholecystectomy rather than only find the factors associated with its conversion.
Finding predictive factors of DLC obligate us to think in intraoperative solutions to overcome difficulties. Hussain 4 reviewed the current evidence and strategies of management of DLC. He found that subtotal cholecystectomy, antegrade or fundus first techniques, and intraoperative cholangiogram significantly reduced the complications and conversion rate in DLC.
In a prospective study, Patil and Inamdar 20 evaluated preoperative data that could serve as predictors of DLC. They reported history of hospitalization (P < .001), previous abdominal surgeries (P < .01), palpable GB (P < .01), BMI >27.5 (P < .01), and thickened GB wall (P < .001) to be significant predictors of DLC. In our study we found that the DLC group had male predominance (P = .001), larger GB dimension on ultrasound (P = .000), thicker GB wall (P = .032), and more pericholecystic fluid collections (P = .004).
Hayama et al. 19 described in their retrospective study that in early surgery for acute cholecystitis, histopathological necrotizing cholecystitis is a risk factor for DLC. For patients treated with delayed surgery, a higher white blood cell count and older age showed significant correlations with DLC and conversion rate. We did not analyze the histopathological result, but the majority of patients in the DLC group (92%) presented with complicated cholecystitis (P = .000), including 11 patients with macroscopic necrotizing/gangrenous cholecystitis and 10 patients with GB empyema.
Some argue against the consideration of the time requirement for the procedure as a part of DLC definition, largely because it is dependent on the surgical expertise of the operating surgeon.4,21 We tried to overcome this effect by performing all the procedures by a surgeon with advanced laparoscopic skills.
The vast majority of publications19,20,22 aiming to find predictive factors of DLC based their results on comparative analysis, lacking of true predictive model analysis with ROC curve and AUC analysis, as well as sensitivity, specificity, PPV, and NPV of each factor.
Bourgouin et al. 2 proposed a preoperative scoring system for both planned and emergency surgery with five preoperative variables: gender, previous cholecystitis attack, neutrophil count, fibrinogen, and alkaline phosphatase. Risk-assessment model was generated with an area under the ROC curve of 0.80. Our study found in A-model analysis an AUC of 0.89 when considering age > 45, male sex, GB wall thickness ≥5 mm, and presence of pericholecystic fluid collection as predictor factors of DLC. Another difference is the inclusion of elective cholecystectomy in the study by Bourgouin et al. We consider important to separate both elective and emergency procedures, because of the difference in the pathophysiology process and prognosis.
CRP is an acute-phase protein with a half-life of 19 hours. It is synthesized and secreted by the liver in response to Interleukine-6 and other proinflammatory cytokines. CRP activates the classical complement cascade and stimulates phagocytosis. A rise in CRP concentrations in serum may be seen with infection, inflammation, trauma, malignancy, and tissue infarction. It is, therefore, not specific for a particular disease. 23
One of the first studies evaluating CRP as a predictor of severity of inflammation in cholecystectomy (both open and laparoscopic) found an OR = 0.979 (95% IC 0.969–0.989). 12
Jessica Mok et al. 13 evaluated in a retrospective cohort parameters that predict DLC or conversion, and also described cutoff points of CRP for predicting conversion. They found that patients with CRP of ≤220 (3.2%) had significantly less chance of conversion than those with CRP >220 (61.9%) (P < .001). In the multiple logistic regression analysis for predicting difficult dissection, the adjusted ORs were CRP (OR = 1.007, 95% CI 1.001–1.012), white blood cell count (OR = 1.12, 95% CI 1.00–1.26), and pancreatitis (OR = 0.03, 95% CI 0.003–0.38). The AUC was 0.782, with a 95% CI 0.678–0.886. This study differs from ours with regard to the inclusion criteria (acute and chronic cholecystitis), type of LC (early and delayed), coexisting illnesses (pancreatitis and common bile duct stones), and rate of conversion.
In a recently published study by Onoe et al., 24 they developed a preoperative scoring system to predict the ability to achieve the CVS in patients undergoing emergency LC for acute cholecystitis. The multivariate logistic regression analyses revealed that CRP >5.5 mg/dL (OR = 9.60, CI 12.54–36.27, P = .001), gallstone impaction (OR = 3.8, CI 1.01–14.24, P = .048), and symptom onset to operation >72 hours (OR = 11.69, CI 3.10–43.57, P < .001) were independently correlated risk factors for the failure to create the CVS. They proposed a scoring system using these three preoperative factors. Some differences exist between this study and ours: they only evaluated the ability to achieve CVS, in our study a more wide definition of DLC was employed (taking into account operative time, time to CVS, intraoperative complications, and conversion to open procedure), and we found different factors associated with DLC (age > 45 years, male sex, GB wall thickness ≥5 mm, and presence of pericholecystic fluid collection on ultrasound).
The limitations of our study are largely attributed to the sample size and lack of external validation of results.
Conclusions
Preoperative CRP with values ≥11 mg/dL was associated with the highest odds (OR = 17.9) of presenting DLC in our study. This value possesses good sensitivity, specificity, PPV, and NPV for predicting DLC in our population. Other significant factors associated with DLC in patients with acute cholecystitis included age > 45 years, male sex, gallbladder wall thickness ≥ 5 mm, and presence of pericholecystic fluid collection on ultrasound. The majority of patients with DLC presented with complicated cholecystitis (necrotizing, perforated, or abscess) and more commonly required subtotal LC.
Footnotes
Disclosure Statement
No competing financial interests exist.