
Abstract
Abstract
Objective:
We present a laparoscopic and single intercostal space thoracoscopic approach (SICS group) for Ivor Lewis minimally invasive esophagectomy (MIE) and provide postoperative analgesia with a continuous multiple intercostal nerve blocking technique. The characters of this technique are evaluated.
Materials and Methods:
From October 2015 to April 2016, 18 consecutive patients with esophageal cancer were treated with Ivor Lewis MIE by a SICS group. Moreover, from July 2014 to September 2015, 48 patients with esophageal cancer received Ivor Lewis MIE by four-port video-assisted thoracic surgery (VATS) approach. Among those patients, by using propensity-score matching, 18 matched patients who underwent four-port VATS MIE (four-port group) were retrospectively selected for further statistical analysis. Patient demographics, short-term postoperative outcomes were recorded.
Results:
None of the patients in the SICS group required conversion to an open procedure. No failure of the intrathoracic esophagogastrostomy occurred. No perioperative mortality or readmission was observed in this series. No patient suffered from anastomotic leak or complained remarkable dysphasia during follow-up. SICS group had a shorter duration of both docking procedure and closure of chest incisions compared with four-port group. The visual analog scale (VAS) pain scores on 24 hours after surgery was significantly lower in SICS group than in four-port group, while the values on 6 hours were comparable. The level of creatine kinase on postoperative day (POD) 1 was significantly lower in SICS group than in four-port group.
Conclusion:
Single intercostal space thoracoscopic procedure is safe and technically feasible and can therefore be viewed as an attractive alternative approach for performing Ivor Lewis MIE.
Introduction
S
Materials and Methods
From October 28, 2015 to April 21, 2016, 18 consecutive patients underwent Ivor Lewis MIE by a SICS thoracoscopic approach. All of the procedures were performed by the same team of surgeons. Each patient was well informed about the new technique and written informed consent was obtained.
Pathological diagnoses of esophagus cancer were preoperatively made in all 18 patients (13 male and 5 female). The location of the esophagus tumor was evaluated by gastroscopy. Seven were located in the middle thoracic esophagus, 8 were located in the distal thoracic esophagus, and 3 were located in the gastroesophageal (GE) Junction. The median age of the patients was 64.5 years (range, 53–86 years), and their median body mass index was 22.3 kg/m2 (range, 17.3–29.3 kg/m2).
As a new approach to perform Ivor Lewis MIE, specific characters of SICS approach are unknown. To demonstrate its unique feature, we retrospectively collected another 18 cases by using propensity-score matching from previous cases who underwent four-port video-assisted thoracic surgery (VATS) Ivor Lewis MIE from July 2, 2014 to September 30, 2015. Some comparison data of the 18 pairs of matched patients from the SICS group and four-port group were provided. All MIE operation videos were recorded and kept in our division, therefore, the duration of docking procedure (wherein the anvil was connected and locked with the shaft of the circular stapler) and closure of chest incisions (which is defined as the suturing of the incised muscles and skin of the three thoracic incisions) were timed in both groups.
All patients were provided with analgesics according to the hospital's standard of postoperative care. Additional morphine was given according to pain scores (visual analog scale [VAS] score > 4) during the entire hospital stay. The patients in the SICS group was provided with continuous multiple intercostal nerve blockade plus intravenous (IV) analgesics once a day. However, the postoperative pain management for four-port group was administrated by IV patient-controlled analgesia. Pain intensity was assessed using VAS in which 0 indicates no pain and 10 indicates the worst pain possible. VAS pain scores were separately measured both on 6 and 24 hours after surgery in the two groups. In addition, the level of creatine kinase, C-reactive protein (CRP), and white blood cell count on postoperative day 1 were separately recorded for analysis.
Surgical technique
The SICS thoracoscopic procedure described here is primarily comprised of two phases. During the initial laparoscopic phase, gastric mobilization, gastric conduit creation, and feeding jejunal tube placement are performed by a widely used approach. 2 In the subsequent thoracoscopic phase, the patient is placed in the left lateral decubitus position with single-lung ventilation. Typically, all of the thoracic incisions are placed at the sixth intercostal space (Fig. 1). A 3-cm incision, used as a main utility port, is expanded with a wound protector that is placed in the anterior axillary line. A 1-cm manipulative port is placed posterior to the middle axillary line. A 1-cm camera port is placed anterior to the scapular line. After thoracoscopic exploration, a retracting suture is placed at the right lower lobe dorsal segment (S6) and brought out through the anterior chest wall with a crochet hook. This aids with exposure and isolation of the distal esophagus.
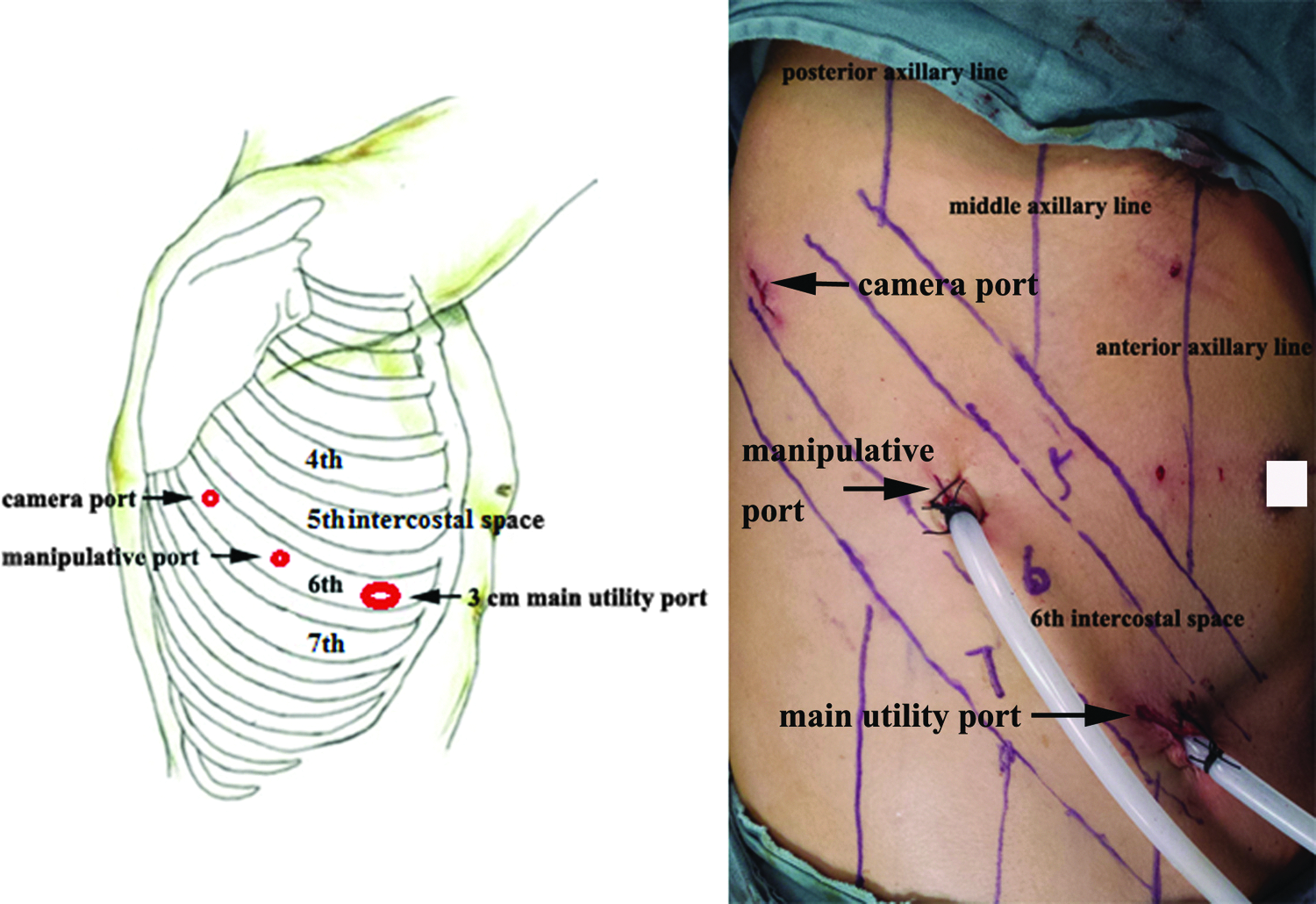
Chest incision sites for thoracoscopy.
Subsequently, to facilitate the mobilization of the upper thoracic esophagus, a secondary retracting suture is placed at the right upper lobe posterior segment (S2) and brought out through the anterior chest wall. The thoracic esophagus is mobilized above the arch of the azygos vein. Meanwhile, the esophagus-surrounded mediastinal lymphatic tissue, subcarinal lymph nodes, and recurrent laryngeal nerve lymph nodes are retrieved. Then, a 25-mm EEA anvil (Covidien DST) is placed into the proximal esophagus using the “Reversal Penetrating Technique” that we have described in a previous report. 3
Esophageal specimens are removed and sent for frozen section analysis of their margins. Thereafter, the gastric conduit is introduced into the thorax through diaphragmatic hiatus. A circular EEA stapler (Covidien) is introduced into the thorax through the main utility port and then advanced into the gastric conduit after gastrostomy is created at the cardia. Then, the circular stapler is docked with the anvil (Fig. 2a), and the anastomosis is performed. During a SICS approach, the camera port is usually located near the posterior upper mediastinum, where the anastomosis is usually made. This facilitates the endoscopic evaluation of the anastomosis from the inside of the gastric cavity (Fig. 2b). The completeness of each anastomosis is therefore ensured.
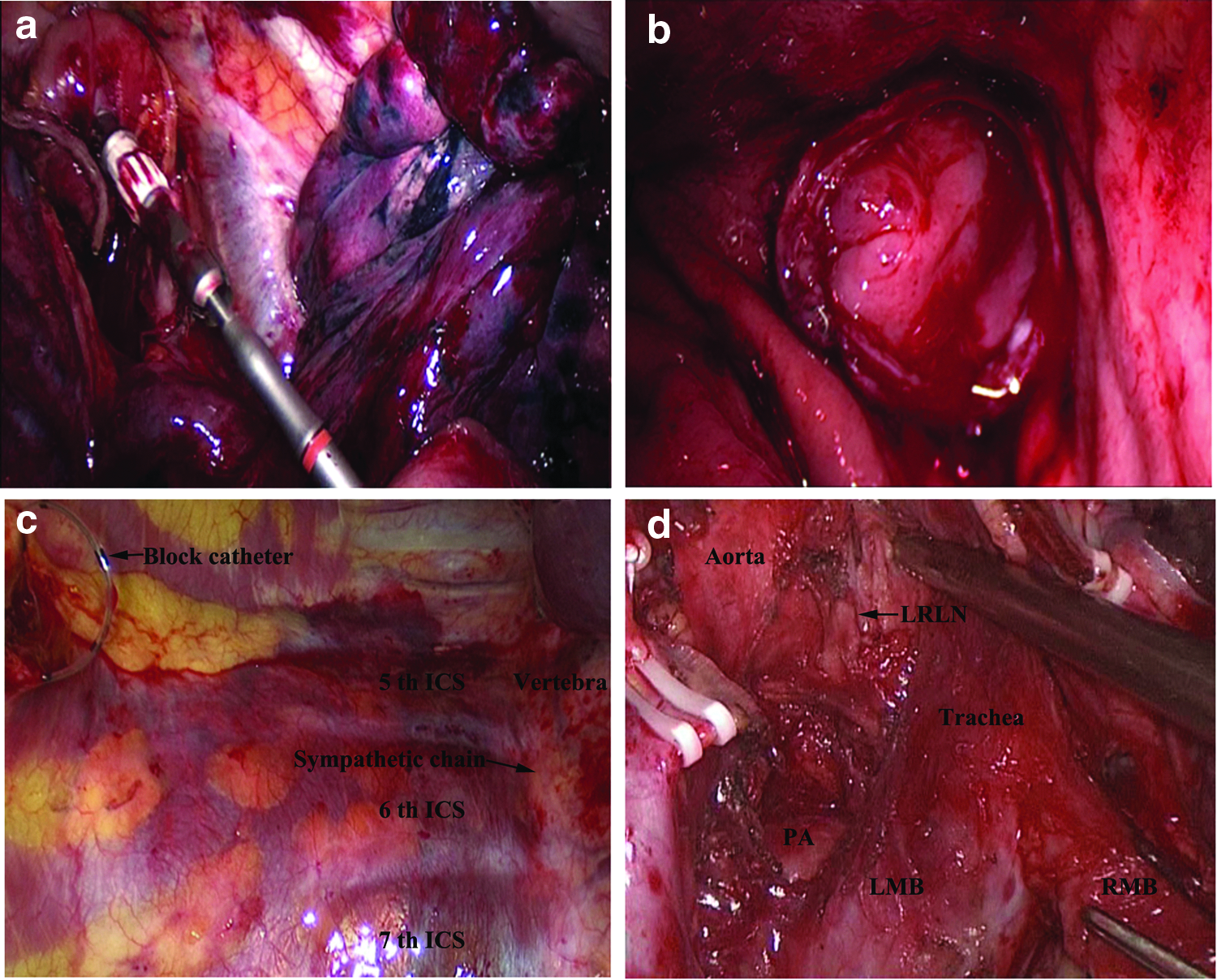
At the conclusion of the procedure, the endoscopic camera is relocated to the main utility port for monitoring. Then, a purpose-designed instrument (Fig. 3) is inserted into the sub-parietal pleura space through the camera port. This instrument is moved toward the vertebra until the level of the thoracic sympathetic chain is reached. Dissection of the sub-parietal pleura tissue is also made by this instrument to enlarge the isolated sub-parietal pleura space to a range extending from the fifth to seventh intercostal space (Fig. 2c). Thereafter, an intercostal nerve block catheter (Plexolong Nanoline, 19G × 100 mm; Pajunk, Germany) (Figs. 2c and 4a) is introduced into the sub-parietal pleura space through the inner column of the instrument, and then one dose of ropivacaine (75 mg/10 mL), used as a preinjection, is given through the catheter to achieve a blockade of fifth to seventh intercostal nerves. Typically, the catheter remains in the sub-parietal pleura space for at least 48 hours before removal.

A purpose-designed instrument used in achieving a blockade of multiple intercostal nerves.

Results
None of the patients in the SICS group required conversion to an open procedure or needed extra thoracic incision. There were no major intraoperative complications such as gross blood loss or tracheal rupture. All the surgical margins were proved negative. The mean operative time for thoracoscopic phase was 135 minutes (range, 110–216 minutes). The median blood loss was 132 mL (range, 65–258 mL). Each patient was scheduled for Gastrografin swallow on the sixth postoperative day. They were allowed to start oral intake on the seventh postoperative day after excluding anastomotic leak.
Postoperative major complications were recorded. No perioperative death was observed. Pneumonia occurred in 3 patients, 4 patients developed atrial fibrillation, and 2 patients were diagnosed with vocal fold paresis/paralysis. No patient experienced gastric tube necrosis or anastomotic leak. No other complications, such as chylothorax, pancreatitis, intestinal obstruction, or wound infection were observed. The mean postoperative hospital stay was 11 days (range, 9–18 days). The mean dissected lymph nodes was 30 (range, 16–48). Their pathological stage classification varied from stage I to stage III (according to the American Joint Committee on Cancer). Seven patients had stage I, 8 had stage II, and 3 had stage III disease. Up to present, only 1 patient complained discomfort in swallowing some solid foods during the follow-up and no localized recurrence was identified.
The duration of docking procedure and closure of chest incisions were separately assessed (Table 1). It shows significant differences between the two groups. VAS postoperative pain scores for two groups at 6 and 24 hours were summarized (Table 2). The SICS group showed significantly lower pain scores at 24 hours than four-port group (0.94 ± 0.64 versus 1.39 ± 0.7, P = .048). No significant differences were observed between the two groups in 6 hours VAS pain scores (0.55 ± 0.61 versus 0.83 ± 0.71, P = .228). We found that the level of creatine kinase was significantly lower in the SICS group than in the four-port group (454.7 ± 31.95 versus 634.3 ± 214.5, P < .005). No differences were noted in terms of CRP (89.19 ± 23.11 versus 111.3 ± 56.59, P = .135) and white blood cell count (14.08 ± 3.69 versus 16.27 ± 5.04, P = .146) (Table 1).
t-Test, SAS (Version 9.3).
SICS, single intercostal space; SD, standard deviation; POD postoperative day.
Kruskal–Wallis H test, SAS (Version 9.3); values are mean ± standard deviation.
SICS, single intercostal space.
Discussion
Minimally invasive esophagectomy is implemented with increasing frequency and offers many potential benefits over other treatment options for esophageal cancer. 4 Despite the increasing adoption of the VATS approach, the techniques suitable for esophagus resection and anastomosis construction are diverse. A four-port VATS approach is frequently used for Ivor Lewis MIE. It is known that the ports should ideally be placed on multiple intercostal spaces and that the main utility port is best placed on the fourth intercostal space. This approach has sometimes raised complaints regarding the difficulty of docking the anvil with the EEA stapler. 5 In an attempt to make this docking procedure easier, to make the MIE procedure even less invasive, and to minimize postoperative pain, we gradually developed an SICS thoracoscopic technique for Ivor Lewis MIE.
We submit that our approach has the following four major beneficial characteristics as compared with other established MIE procedures. (1) The location of the main utility incision provides a proper position relation between the anvil and the EEA stapler. The docking procedure appears to be easy with our approach and does not require a specifically designed instrument to stabilize and assist the establishment of the connected portion in a parallel alignment position 5 (Fig. 2a). We observed that a shorter duration for docking procedure was achieved compared with four-port VATS approach (Table 1). This approach allows the surgeon to work in the cephalad orientation and facilitates lymph node retrieval (Fig. 2d).
(2) In comparison with an incision at the fourth intercostal space, which generally refers to incision at the pectoralis major or the female breast, the main utility incision at the sixth intercostal space in the anterior axillary line mainly cuts off intercostal muscles. When making the manipulative port and the camera port, after the skin is incised, the chest wall is punctured with a 10-mm trocar without fully cutting off the muscles. This can be considered as a further muscle-sparing measure. Interestingly, this study provides statistically significant differences in terms of the level of creatine kinase and the duration of chest incisions closure between the groups. We concluded that less chest muscles were incised and sutured, which might probably be the reasonable explanation.
(3) In our approach, a blockade of the fifth to seventh intercostal nerves is performed while only the sixth intercostal space is incised. The patients complained of only negligible pain after this procedure (Fig. 4b). It appears that better postoperative analgesia is achieved with this approach than in the four-port VATS procedure (Table 2). (4)The sixth intercostal space at the anterior axillary line is relatively wide and elastic, making the insertion of linear staplers or EEA staplers much easier. Since all of the incisions are placed in the same intercostal space, any conversion to an open approach, if it became necessary, is easy.
During the last 2 years, besides our experiences with four-port VATS Ivor Lewis MIE, we have performed hundreds of SICS VATS lobectomy. We believe unequivocally that this experience was supportive for the adoption of the SICS Ivor Lewis MIE. We had previously attempted to perform the Ivor Lewis MIE by single-port VATS. We experienced mutual interference among the instruments and insufficient exposure of the surgical field, so we ultimately adopted the SICS approach because we felt it might preclude such limitations. Remarkably, the SICS approach for MIE might be relatively technically demanding, as surgeons need to be familiar with both SICS VATS and four-port Ivor Lewis MIE.
Admittedly, it was a retrospective study. Although the patients were propensity score-matched, information bias were still exist. Considering the limited amount of involved patients, some other indicators such as the postoperative major morbidities, hospital stays, and pain experiences after discharge were not compared between the two groups. Therefore, a prospective and randomized study that includes an even larger group of patients needs to be conducted.
Conclusions
As the first report of Ivor Lewis MIE performed with SICS approach, SICS procedure is safe and effective. This approach is worthy of clinical practice for professional surgeons in high-volume centers.
Footnotes
Acknowledgments
The study was supported by funds from National Natural Science Foundation of China (81272594) and Zhejiang Provincial Natural Science Foundation (LY16H010004).
Disclosure Statement
No competing financial interests exist.