
Abstract
Abstract
Background and Aims:
In the last decades, the three-dimensional (3D) imaging systems have been introduced in an attempt to improve depth perception and image quality during laparoscopic cholecystectomy interventions. The goal of our systematic review was to provide enough convincing evidences on superiority and benefits of 3D over two-dimensional (2D) imaging systems, from both surgeon's and patient's point of view, justifying the cost-effectiveness of newly developed 3D systems.
Methods:
Two authors separately performed a full literature search aiming to find randomized controlled trials evaluating the advantages and disadvantages of 3D versus 2D laparoscopic cholecystectomy procedures. The patients who underwent elective laparoscopic cholecystectomy were included in this study irrespective of their age and sex. Differing opinions between the two authors were reviewed by the third author.
Results:
A total of 912 articles were initially reviewed by their titles and abstracts for eligibility. After being filtered through predetermined inclusion and exclusion criteria, and excluding the duplicates, only 10 studies underwent the final evaluation by the full text assessment. Eventually, only five randomized controlled studies were included in this study. Operative time and depth perception/image quality were set as the primary and secondary outcomes, respectively. The operative time was significantly shorter in 60% of the studies. Of five studies that evaluated the depth perception and image quality, all five (100%) reported a better depth perception and image quality.
Conclusions:
3D imaging systems tend to shorten the operative time compared to 2D systems and result in a better depth perception. More studies and investigations with bigger cohort sizes and using unique 3D visual systems are necessary to justify the cost-effectiveness of the new, more expensive 3D systems.
Introduction
Background and 2D Challenges
E
3D Advantages Expected
During the past 3 decades, 3D imaging systems have been introduced in an attempt to improve depth perception during Minimal Access Surgery. 5 The anticipated advantages for the surgeon are greater accuracy and speed in manual skills, translating to decreased operative time, a reduced learning curve, and enhanced safety. Nevertheless, studies, to date, examining the potential advantages and disadvantages of 3D systems have produced contradictory results. 6 The contradictions between the studies that have been carried out on advantages and disadvantages of 3D versus 2D imaging systems were the leading initiatives and motives of our systematic review. During the past few decades, with the evolutionary advancements in surgical laparoscopic technology, the 3D imaging systems have been introduced and developed. Many studies have been conducted on laparoscopic simulator box trainers, trying to compare variety properties of 3D and 2D visual systems, and have shown different results concerning benefits of 3D imaging.
Aims and Objectives
Due to lack of studies comparing the advantages and disadvantages of 3D versus 2D imaging systems in real clinical settings, and heterogeneity in evaluated outcomes of these studies, we decided to conduct a systematic review focusing on all the studies performed on real clinical laparoscopic cholecystectomy procedures, comparing the benefits of 3D versus 2D systems. The goal of our systematic review was to provide enough convincing evidences on superiority and benefits of 3D systems over 2D, from both surgeon's and patient's point of view, justifying the cost-effectiveness of newly developed 3D systems.
Materials and Methods
In this study, in accordance with the PRISMA guidelines, we conducted a thorough systematic search through literature, aiming to identify randomized controlled trials (RCTs) comparing and contrasting the advantages and disadvantages of 3D versus 2D laparoscopic cholecystectomy procedures (Fig. 1). The literature search was completed in March 2017. The online databases MEDLINE/PubMed, Excerpta Medical Database (EMBASE), and the Cochrane library were explored. Patients who underwent elective laparoscopic cholecystectomy, irrespective of age and sex, were included in the study (Appendix 1). Only randomized clinical trials (irrespective of publication status or sample size) were included. Studies having their full text published originally in any language other than English were not considered. Two authors (I.K. and G.C.) independently conducted the initial search and identified all relevant articles by screening their titles and abstracts. The final selection of articles was made by the two authors after reading the full-text articles and references, and their selection was based on the reporting of all necessary data and in accordance with the predefined inclusion and exclusion criteria. Differing opinions on whether to include or exclude articles were resolved through discussion by two authors. If agreement could not be reached, a third author (G.N.) reviewed the article and made the final decision. Furthermore, the reference lists of the included RCTs were examined to find additional relevant trials.
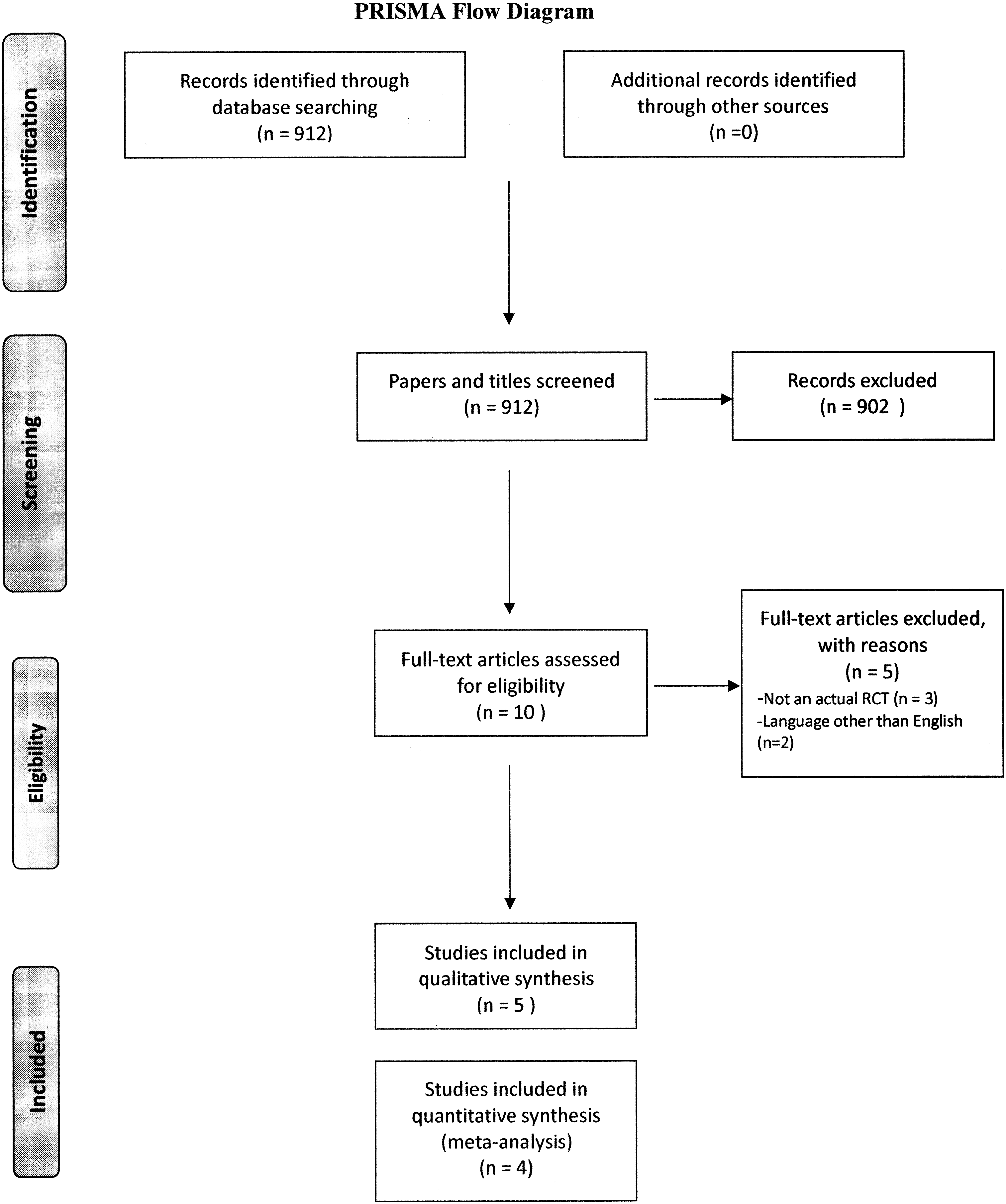
Flowchart of the selection process of included articles. RCT, randomized controlled trial.
Study design
Only RCTs were included. We defined RCTs as studies with abstracts or full texts that stated that the trial participants were randomly assigned to operate using either 2D or 3D laparoscopic vision conditions.
Data extraction
Data extracted from the included randomized clinical trials were as follows: Country and year of publication, number of surgeons, number of patients, exclusion criteria, 3D equipment, performance time, results, and conclusion. Only the performance time of the intervention was included as the quantitative analysis, given the heterogeneity in the studies in terms of methodology, 3D equipment used, and outcome measures.
Results
A total of 912 articles were initially screened for eligibility by their title and abstract. After the primary screening and applying the pre-determined inclusion and exclusion criteria, 10 potentially relevant studies were identified and read in the full text. Of the 10 trials, five studies were excluded because they were not actually RCTs or their original full text was published in languages other than English (Fig. 1). Thus, we included five trials, all performed in clinical settings (Table 1). Based on the results obtained from reviewed RCTs, we set the primary and secondary outcomes as follows:
Primary outcomes:
1. Operating time 2. Depth perception 3. Conversion to open cholecystectomy
Secondary outcomes:
1. Postoperative complications 2. Errors 3. Surgeon's discomfort
2D, two dimensional; 3D, three dimensional.
3D versus 2D effect on operating time
All the five studies evaluated the operative time in 3D versus 2D laparoscopic cholecystectomy surgeries (four quantitatively, one quantitatively 8 ). Three out of these five studies (60%) reported a significant reduction in operative time in 3D laparoscopic cholecystectomies compared with 2D9–11 ; two studies (40%) showed no significant difference in the operative time between the 3D and 2D visual systems.5,8
3D versus 2D effect on depth perception
All five (100%) studies reported the differences in depth perception between 3D and 2D laparoscopic cholecystectomy procedures. All the five studies demonstrated better depth perception and image quality in 3D imaging systems in contrast to 2D ones. However, the result was not statistically significant in one of the studies. 8
Rate of conversion to open cholecystectomy between 3D versus 2D imaging systems
Four out of five studies (80%) reported no need for conversion to open cholecystectomy during 2D and 3D laparoscopic surgeries. One study did not report this outcome. 10
Postoperative complications
Three studies have reported no postoperative complications in neither 2D nor 3D laparoscopic cholecystectomies.
Error rate
Four studies reported the error rates during the 2D and 3D laparoscopic procedures. A total of 22 errors occurred, of which a total of 13 errors occurred during 2D, while 9 errors occurred during 3D laparoscopic procedures.
Surgeon's discomfort
While two studies reported increased surgeons's discomfort (↑ visual strain, headache, facial discomfort, ear discomfort, physical discomfort, ↓ ease to handle and user-friendly, and ↑ dizziness),5,8 only one study reported decreased visual strain during 3D surgical procedures. 11
Discussion
Although 3D vision technology for laparoscopy has substantially improved, thus providing new and better visualization possibilities for the surgeon, it is still not the common standard for laparoscopy. 3 During the systematic search performed through the literature, we encountered some experimental studies that have reported the 3D systems improve task efficiency in laparoscopic manipulations, whereas other reports found no significant difference between 3D and 2D systems. The synthetic phantom task setup used and the involvement of medical students during experimental studies simulate only partial surgical procedures, do not reflect the complexity of clinical conditions, and could lead to unreal results. 11 These studies have been excluded in our study respecting the preset exclusion criteria. All five studies included the operative time as a measured outcome. Sixty percent (three out of five) of studies showed a statistically significant reduction in operative time as an advantage of 3D visual systems compared to 2D. If 3D equipment reduces operating or training time for new surgeons, the equipment may be a worthwhile investment. 3D technology is still more expensive than standard 2D equipment.12,13 Nevertheless, 3D laparoscopy is more affordable than robotic systems, which also provide 3D vision. However, robotic systems also have the advantage of articulated instruments.12,13 Robotic systems may not be necessary for many routine procedures with benign conditions, for which 3D laparoscopy vision systems may be a more relevant option. Five studies reported the differences in depth perception and image quality between 3D and 2D laparoscopic cholecystectomy procedures. All the five studies5,8–11 demonstrated better depth perception and image quality in 3D imaging systems in contrast to 2D ones. Rate of conversion to open cholecystectomy and error rate is not significantly different between 2D and 3D imaging systems. Surgeon's discomfort seems to be more pronounced in 3D visual systems compared to 2D. The limitation of our study was the small number of studies, different 3D visual systems utilized, and lack of focus on common outcomes. Further studies on larger cohorts are warranted to determine whether the complications and risk of conversion to open surgery will decrease with the use of these systems in laparoscopic cholecystectomy.
Footnotes
Disclosure Statement
No competing financial interests exist.