
Abstract
Abstract
Background:
About 20% of the population has cholelithiasis and this is the main abdominal cause of hospitalization in developed countries. Considering that only in the United States about 700,000 cholecystectomies are done each year, it is possible to estimate the importance of the problem for public health.
Objective:
To describe a two-incision laparoscopic cholecystectomy (TILC) technique using only conventional material, without increasing complications or operative time.
Materials and Methods:
A consecutive and prospective case series compared to another historical operated by conventional laparoscopic cholecystectomy (LC). The TILC was performed with three trocars in two incisions, two trocars in umbilical incision, and one in epigastrium.
Results:
A total of 72 patients were operated on by the same surgeon (36 in each group). There were no significant differences between groups for gender, mean age, body mass index, or length of hospital stay. The procedures were classified by the surgeon according to surgical difficulty and 58.3% (n = 42) were considered low grade, 9.7% (n = 7) difficult, and the other were intermediaries, with no difference between the series (P < .05). There were minor complications in 6.94% (n = 5) procedures. There were no differences between mean operative time (P = .989), which was 49 (95% confidence interval [CI] 42–56) minutes in LC and 40 (95% CI 35–44) min in TILC. There was no need for additional trocars in any case or for conversion to open surgery.
Conclusions:
TILC is feasible, safe, and with good aesthetic result, using the same instruments of LC, without increasing operative time.
Introduction
F
One alternative that has been developed is single-incision laparoscopic surgery (SILS). Theoretically, all instruments are used through a single incision of up to 30 mm in the umbilical scar.10–14 The incision can cross the borders of the navel to hold the laparoscope besides two or three forceps, making the aesthetic results questionable. Studies have demonstrated longer operative time and suggested higher costs in single-incision laparoscopic cholecystectomy (SILC) compared to LC.15–19 In addition, there is a potential increase in the risk of incisional hernia by using a larger incision than in LC20–23 and the risk of iatrogenic lesions may be higher due to the use of instruments in parallel alignment.10,24–32 The narrow space to manipulate instruments generates collision and makes triangulation difficult, increasing the technical difficulty. 33 To minimize the difficulties encountered in SILS, it is common to associate a second incision for an auxiliary instrument.8,11,14,17,21,34–38 This second incision has been used to elevate the gallbladder and expose the Calot's triangle, but not for dissection. Despite the second incision, retaining three instruments at the same incision could result in collision and increase damage to the abdominal wall. However, by decreasing the number of instruments to two in the same incision, collision and abdominal wall injury are reduced. Also, if a second incision is added in a suitable place, the incisions can be reduced, operating with triangulation of forceps and free movements.
In accordance with safety standards and with the intention of reducing scars, it was proposed to perform the two-incision simplified laparoscopic cholecystectomy (TILC), using a hybrid technique with an incision inside the umbilicus and another in the epigastrium to operate similarly to standard LC.39–41 The objective of this study is to test the hypothesis that it is possible to reduce incisions safely and using only conventional material. The parameters commonly used to test these outcomes are operative time and incidence of complications and were used for comparison between the groups.
Materials and Methods
The study was carried out at the Santa Cruz Hospital of the University of Santa Cruz do Sul, and was submitted and approved by the local research ethics committee (447,342/2013). Written and informed consent was obtained from all patients.
A case series of 40 consecutive patients who had indication for cholecystectomy and who were treated in the period between January 2014 and October 2016 were included. Another historical series of 36 patients operated with the LC technique was used as a control group. All cases with indication of cholecystectomy were included in the study, regardless of whether the intervention was elective or in an emergency. Exclusion criteria were as follows: clinical contraindication for laparoscopic surgery or for general anesthesia, age younger than 16 years, American Society of Anesthesiologists (ASA) classification higher than III, and cases requiring concomitant procedures such as exploration of biliary tract, correction of hernias, or extensive lysis of adhesions due to previous surgeries. The variables gender, age, body mass index (BMI), operative time, length of hospital stay, and complications were collected. Intraoperative cholangiogram was performed selectively. 7 The procedures were classified in levels of difficulty by the surgeon. The procedures were classified as low grade (easily identifiable anatomy without distortions, no inflammatory process, adhesions easily removable), intermediate (mild to moderate inflammatory process, and/or liver hypertrophy hindering the visualization of the Calot's triangle, and/or firm adhesions), or difficult (anatomy difficult to identify, and/or intense inflammatory process, and/or need for suturing). Immediately after the end of procedure, the surgeon classified the perception of physical exertion according to the modified Borg scale, 42 ranging from zero, in the absence of perceived exertion, to 10, in the maximum perception of effort or discomfort.
The procedure was performed under general anesthesia and the patient was placed in the dorsal decubitus position. The surgeon and assistant were positioned on the left side of the patient. A longitudinal incision of about 15 mm was made within the umbilical scar. Pneumoperitoneum was created in the same manner as LC and the first 10-mm trocar (T1) was inserted into the umbilical incision. The second 10-mm trocar (T2) was introduced into the epigastrium, just below the xiphoid appendix, in the second incision. With optical viewing through the epigastric trocar (T2), a 5-mm trocar (T3) was introduced in the umbilical incision, puncturing the aponeurosis lateral to T1. A 10-mm rigid laparoscope was placed on T1, a grasping clamp on T3, and dissection forceps on T2. A straight needle suture was introduced into the abdominal cavity about 10–20 mm below the right costal margin, close to the anterior axillary line, through the extramucosal layer of the body of the gallbladder and returning outside near the site of entrance, favoring exposure of the Calot's triangle. The T3 forceps manipulated the infundibulum of the gallbladder working as an “X” with the laparoscope in the umbilical incision (Fig. 1). The Maryland forceps, hook, and clip applier were freely used in T2 as in the LC technique. The patient was only positioned in slight reverse Trendelenburg in cases where the omentum covered the vision of the surgical field. The cystic artery and duct were clipped and sectioned as in LC. After dissection, the gallbladder was removed from the abdominal cavity inside a bag through T2. The aponeurosis of the umbilical incision was sutured taking care to close both trocar openings (10 mm and 5 mm). In cases where cholangiogram was required, a 16G catheter (Intracath central venous catheter) was used just below the right costal margin. A 10 cases pilot project was carried out to standardize the technique. 39

Arrangement of instruments in TILC. TILC, two-incision laparoscopic cholecystectomy.
Data were analyzed in the Stata 9.2 program. Central tendency tests were used for the statistical calculations. Fisher's exact test was used to verify associations. For evaluations of mean differences, the Student's t test was used for normal continuous distribution variables and Mann–Whitney for the asymmetrically distributed variables.
Results
Forty patients were operated on. Four were excluded from the study. One due to hemodynamic instability (ASA IV) and another three due to the need for additional procedures (two cases for exploration of the biliary ducts and another for extensive lysis of adhesions due to previous surgery). Another 36 sequential cases previously operated with the LC technique were used as control group. The final sample included 72 cases, 36 in conventional approach and 36 in the two-incision technique. All patients were operated on by the same surgeon. The majority of the patients were female (77.8%), the mean age was 48.5 years (standard deviation [SD] = 15.6), and the BMI was on average 28.4 kg/m2 (SD = 4.0). Regarding the procedure, mean operative time was 44 minutes (SD = 17) and the patients were hospitalized for 31 hours (SD = 28.6) on average. Intraoperative cholangiogram was performed in 12 (17%) patients with selective indication. Regarding the degree of difficulty, 58.3% (n = 42) were considered easy and 9.7% (n = 7) were difficult. The analysis of difficulty levels between the groups did not show any significant difference (P = .05). Classification by the modified Borg scale showed that the surgeon's perception of exertion was at maximum light (Borg 2) in 73.6% (n = 53) of the procedures.
Table 1 shows the comparisons between groups. There was no difference between the variables: sex, mean age, BMI, operative time, and length of hospital stay.
LC, laparoscopic cholecystectomy; TILC, two-incision laparoscopic cholecystectomy; CI, confidence interval; BMI, body mass index.
There was no need for additional trocars or conversion to open surgery in any case. The prevalence of complications in the TILC-operated group was 5.6% (n = 2) and 8.3% (n = 3) in the control group (P = 1.00). There were only minor complications. There was no statistically significant difference in the mean operative time for surgery with the conventional technique or with the TILC technique (49 [95% (confidence interval [CI]) 42–56] × 40 [95% CI 35–44] min, P = .989, respectively). The perception of physical effort was classified by the surgeon through the modified Borg scale and showed difference between groups. The ergonomic effort from moderate to intense (Borg 3, 4, 5, or 6) occurred in 53% (n = 19) of LC procedures, versus none of the TILC technique (P < .001). In most cases operated with two incisions (69%), the surgeon did not perceive any type of discomfort during the procedure (Borg 0). The TILC technique reduced the number of incisions in half, compared to the conventional technique (Fig. 2). The use of two trocars in the same incision allowed to keep the surgical scar within the limits of the umbilicus.

Final result after TILC. TILC, two-incision laparoscopic cholecystectomy.
Discussion
Cholecystectomy could be performed in all cases without the need for additional incisions or trocars. Only conventional instruments were used. All patients were operated with a 10-mm laparoscope, positioned in the same place as the LC, providing visual field and image exactly the same as the standard technique. The positioning of one forceps in the epigastrium and another in the umbilical scar allowed triangulation by 90° (Fig. 3). Dissection forceps, electrocautery, and clip applier were used freely in the epigastrium in the same manner as in LC. The use of two instruments working as “X” in the same incision creates only one axis of rotation between them resulting in very little collision. The grasper handled in the umbilical incision allowed for easy opening of the triangle of Calot with adequate presentation of the cystic duct. Without a traction grasper at the fundus, the elevation of the gallbladder depended on the use of transparietal traction wire. However, it is possible to operate even without using it as in the three-incision technique.16,43–45 The suture should be applied superficially to the wall of the gallbladder to avoid bile overflow. It is suggested to empty the gallbladder before applying suture if there is difficulty. Although it requires skill not used for LC, traction suture does not require knot tying, just needle handling. It can be done in a simple way with instruments working in 90° angle and with the right hand totally free. This task can be used to exercise suture skill in a low-complexity procedure when performed by residents or junior surgeons.
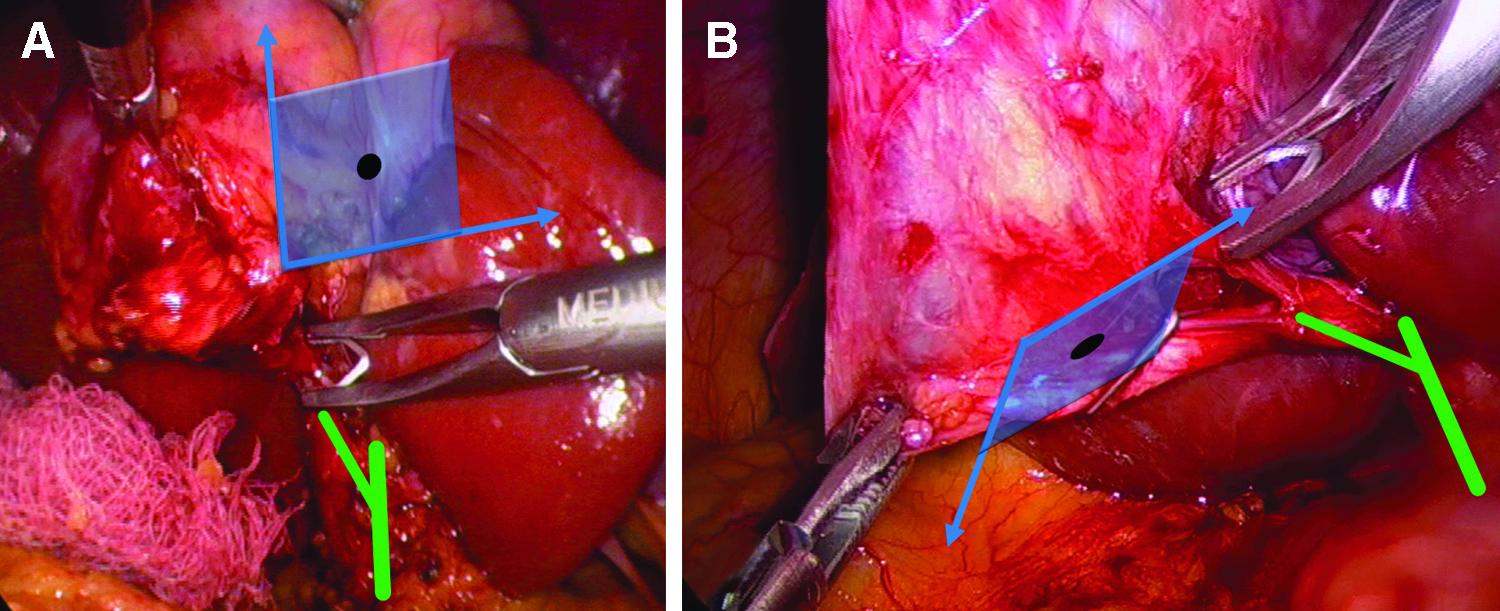
Triangulation of instruments in LC
Regarding complications, the prevalence was 6.94%, being only minor and comparable to rates of the LC,9,46–48 suggesting that TILC is safe.
The concept of aesthetics involves subjectivity. From the patient's point of view, there are greater concerns about safety and pain, 49 with aesthetics remaining in the background. Another difficulty for analysis of this variable is that the patient does not have objective parameters for comparison. Even so, it can be assumed that the TILC offers a superior cosmetic result than LC, since the number of incisions decreased by half.
Few studies have investigated the ergonomics of surgeons in LC,50–54 but it has been observed that it is common to adopt inappropriate postures during the performance of surgical procedures. Changes in operative techniques may help prevent injuries.52,53 Studies comparing surgeon ergonomics during LC and SILC conclude that operating through a single incision is even more stressful and more physically demanding.54,55 In the TILC, the surgeon operates with two incisions in the patient's midline, being able to work with shoulders and elbows aligned, as in “French” positioning, but without requiring trunk flexion, maintaining an ergonomic position (Fig. 4). In this research, when the surgeon performed LC, he perceived a moderate to intense effort in more than half of the cases. However, in TILC, he did not perceive any discomfort in more than two-thirds of the cases (P < .001). The study demonstrated that the greater the degree of difficulty of the procedure, the greater the physical effort used by the surgeon (P = .002). This suggests possibility of association between the ergonomics and the incidence of complications, because stress could influence the decision-making of the surgeon, especially in more complex cases. In this study, the researcher was the only measurer, which prevents the conclusion of the ergonomics response due to the risk of measurement bias.

Positioning of the surgeon in TILC. With two incisions aligned in the patient's midline, the surgeon operates with shoulders and elbows also aligned. TILC, two-incision laparoscopic cholecystectomy.
For the research, a standardization of TILC technique was adopted, in which the second incision enables instruments of 10 mm, allowing the use of clip applier. In such a way, the surgeon works in a very similar manner to the LC and, consequently, with the same safety care. However, the TILC technique can be improved with superior aesthetic results. One can replace the 10-mm epigastric incision by 5 mm and manage cystic duct with 5-mm clip applier or with knot tying. It is also possible to use 3-mm instruments in the epigastrium, making ligation of the cystic duct with wire and cauterizing the cystic artery. Alternatively, it is possible to use a 5-mm laparoscope, enabling the 10-mm trocar for the 10-mm clip applier use, through the umbilical incision.
The two-incision simplified laparoscopic cholecystectomy technique (TILC) is feasible, safe, and with good aesthetic result. It allows to use only the same instruments of standard laparoscopic cholecystectomy (LC), without increasing the operative time.
Footnotes
Disclosure Statement
No competing financial interests exist.