
Abstract
Abstract
Background:
Although the role of staging laparoscopy (SL) in detecting radiologically occult M1 disease has been widely recognized, it is seldom used in China and its clinical value based on Chinese population has been rarely reported. The aim of this study is to identify the yield of SL for Chinese patients with advanced gastric cancer (AGC) and determine the proportions of patients in whom treatment plan is altered.
Materials and Methods:
The clinical data were retrospectively collected from 879 AGC patients who underwent SL without any definite signs of disseminated disease on imaging examination. The primary outcomes were the proportions of patients whose laparoscopy identified incurable factors (including M1 diseases and unresectable T4b diseases), and who had their treatment plan altered.
Results:
SL revealed incurable factors in 130 (14.8%) patients, including macroscopic peritoneal metastasis (n = 92), positive peritoneal cytology (n = 10), liver metastasis (n = 12), para-aortic lymph node metastasis (n = 1), and unresectable T4b tumor (n = 18). After SL, treatment plans were altered in 123 (14.0%) patients, among which 82 (63.1%) patients were not offered any further procedure and referred for chemotherapy. Among 749 M0 patients who immediately proceeded to radical gastrectomy after SL, new incurable factors were found at subsequent operations in 21 (2.8%) patients. Multivariate analysis showed that tumor size ≥8 cm, Borrmann type III and IV, and tumor invasion of T4a and T4b in preoperative imaging examination were the predictive factors for peritoneal metastasis.
Conclusions:
SL detects additional incurable factors in Chinese AGC patients with potentially resectable disease and optimizes their treatments. A systematic and painstaking inspection of the whole abdominal cavity, including routine entry into the bursa omentalis, is necessary for improving the yield of SL.
Introduction
T
Due to the low sensitivity of preoperative imaging for detection of peritoneal metastasis, the current National Comprehensive Cancer Network (NCCN) and European Society of Medical Oncology (ESMO) guidelines recommend laparoscopy as part of the staging workup for patients with advanced and potentially resectable gastric cancer.4,5 Staging laparoscopy (SL) can detect M1 disease that is not apparent on imaging examination and avoid unnecessary laparotomy for 30%–40% of patients with newly diagnosed gastric cancer.6–8 Unfortunately, as an invasive diagnostic approach, SL is seldom used in China and its clinical value based on Chinese population has been rarely reported.
Besides early gastric cancer, laparoscopic surgery has been widely used for the treatment of local AGC in China, although its long-term oncologic outcomes still need further investigation in large randomized clinical trials. Laparoscopic exploration before planned laparoscopic gastrectomy was performed without the purpose of staging. However, these procedures could actually obtain the similar effect with SL. This retrospective study aimed to identify the yield of SL for Chinese AGC patients and determine the proportions of patients with altered treatment plan.
Materials and Methods
Patient characteristics
This study was approved by the Institutional Review Board of the Second Affiliated Hospital of Nanchang University. A total of 1044 gastric cancer patients underwent diagnostic laparoscopy or laparoscopic surgery at the Second Affiliated Hospital of Nanchang University between September 2008 and September 2016. Patients who had early gastric cancer (n = 92), patients with recurrent gastric cancer or known metastatic diseases (n = 16), patients who had received prior chemotherapy and/or radiation therapy (n = 39), and patients whose procedures were performed with the purpose of palliative therapy (e.g., gastric bypass and palliative gastrectomy) (n = 18) were excluded from the study. As a result, 879 patients were enrolled in the analysis, among which 67 patients received diagnostic laparoscopy for determining further treatment strategies (mainly for confirming clinically suspected peritoneal metastasis), and others underwent laparoscopic exploration before planned laparoscopic radical gastrectomy. We have defined both diagnostic and exploratory laparoscopy as SL in this study. All the enrolled patients had confirmed histological diagnosis of gastric cancer before SL, without any definite signs of disseminated disease (e.g., peritoneal metastasis and liver metastasis) on computed tomography (CT), endoscopic ultrasound (EUS), or positron emission tomography, and were candidates for radical resection.
Staging laparoscopy
The patient was placed in the supine position under general anesthesia. A standard three-port technique was adopted. A small periumbilical incision was made and a 10-mm trocar was inserted. A CO2 pneumoperitoneum was established with a pressure of 10–15 mmHg and laparoscope was inserted using a 30°telescope. Two other 5-mm trocars were introduced in the left and right upper quadrant for the use of palpation and biopsy of suspicious lesions. A thorough and orderly exploration was performed. First, the entire abdominal cavity was inspected, including the primary tumor site of the stomach and the surrounding peritoneum, liver, diaphragm, omentum majus, small bowel and its mesenteries, colon and its mesenteries, adnexal (female), and pelvic floor. Then, the transverse colon and small bowel were pushed away by grasping forceps to examine the root of mesenteries. Finally, the gastrocolic ligament was opened to examine the pancreas, transverse colon, and its mesentery inside the bursa omentalis. Suspicious lesions were biopsied for histological examination. Peritoneal washing for cytological assessment was not routinely performed, except for the cases of serosal invasion (cT4a and cT4b). Peritoneal lavage sample was obtained by instilling 500 mL normal saline within the abdomen and aspirating the return and stained with Papanicolaou and Giemsa stains.
Data collection and variable definitions
Data were collected through retrospective review of electronic medical records, including age, gender, tumor location, tumor size, histologic tumor grade, macroscopic type, radiologic staging, macroscopic laparoscopic findings, and peritoneal cytology results. Preoperative radiologic stage was determined according to the Tumor-Node-Metastasis (TNM) staging of gastric cancer. 9 The laparoscopic positive findings were classified as follows: macroscopic peritoneal metastasis, positive peritoneal cytology, distant organ metastasis (e.g., liver and distant lymph node), and unresectable direct invasion of tumor into adjacent organ (T4b), which were neglected by preoperative imaging examination. The false-negative rate of SL to determine incurable factors is defined as the number of patients whose planned radical gastrectomy was not performed due to new findings of incurable factors at subsequent operation among the number of patients deemed to be suitable for radical resection at SL.
Outcome measurements
The primary outcomes were defined as the proportions of patients whose laparoscopy identified incurable factors and who had their treatment plan altered. One of the secondary outcomes was the false-negative rate of SL to determine incurable factors. The causes of incurable factors being missed were analyzed. Since SL was performed with the main purpose of ruling out peritoneal metastasis, the other secondary outcome was to identify risk factors associated with peritoneal metastasis (including positive cytology) to reasonably select patients who are more likely to benefit from SL.
Statistical analysis
The statistic software SPSS, version 22 (IBM, New York), was used to perform data analysis. A chi-square test was used to analyze the correlation between peritoneal metastasis and clinicopathologic factors. Logistic regression was used to identify risk factors for peritoneal metastasis. A two-sided P-value <.05 was considered significant.
Results
Patient characteristics
A total of 879 patients were eligible for inclusion in this analysis. There were 582 men and 297 women with a median age of 59 years (range 19–91 years). The primary tumor was poorly differentiated in 487 (55.4%) patients and Borrmann type IV in 89 (10.1%). Preoperative imaging indicated that 38.5% of patients had cT4 (including cT4a and cT4b) disease and 41.9% had lymph node metastasis (Table 1).
Yield of staging laparoscopy
Laparoscopy showed macroscopic peritoneal metastasis in 92 patients (10.5%). Among 213 patients without macroscopic peritoneal metastasis and who underwent peritoneal lavage cytology examination, 10 (4.7%) had positive cytology. Accordingly, radiologically occult peritoneal metastasis was found in 11.6% of patients. Other incurable factors identified at laparoscopy included liver metastasis in 12 patients (1.5%, including 1 with peritoneal metastasis), para-aortic lymph node in 1 patient (0.1%), and unresectable T4b tumor that was neglected by imaging examination in 18 patients (1.3%, including 2 with peritoneal metastasis). The total yield of SL was 14.8% (130/879) (Table 2).
Altered treatment plan after staging laparoscopy
M1 disease was detected at SL in 114 M1 patients. Among those, 7 underwent radical resection, 23 underwent palliative resection, 15 underwent gastric bypass, and 69 were not offered any further procedure and referred for chemotherapy. Of the 765 patients with laparoscopic stage M0, 3 underwent gastric bypass and 13 converted to chemotherapy due to findings of unresectable T4b disease, and the remaining 749 patients immediately proceeded to radical gastrectomy. Thus, the treatment plan was changed in 123 (14.0%) patients who did not undergo radical gastrectomy (Fig. 1). Notably, among 10 patients with positive peritoneal cytology, 7 patients underwent radical gastrectomy due to delayed report of peritoneal cytology results.
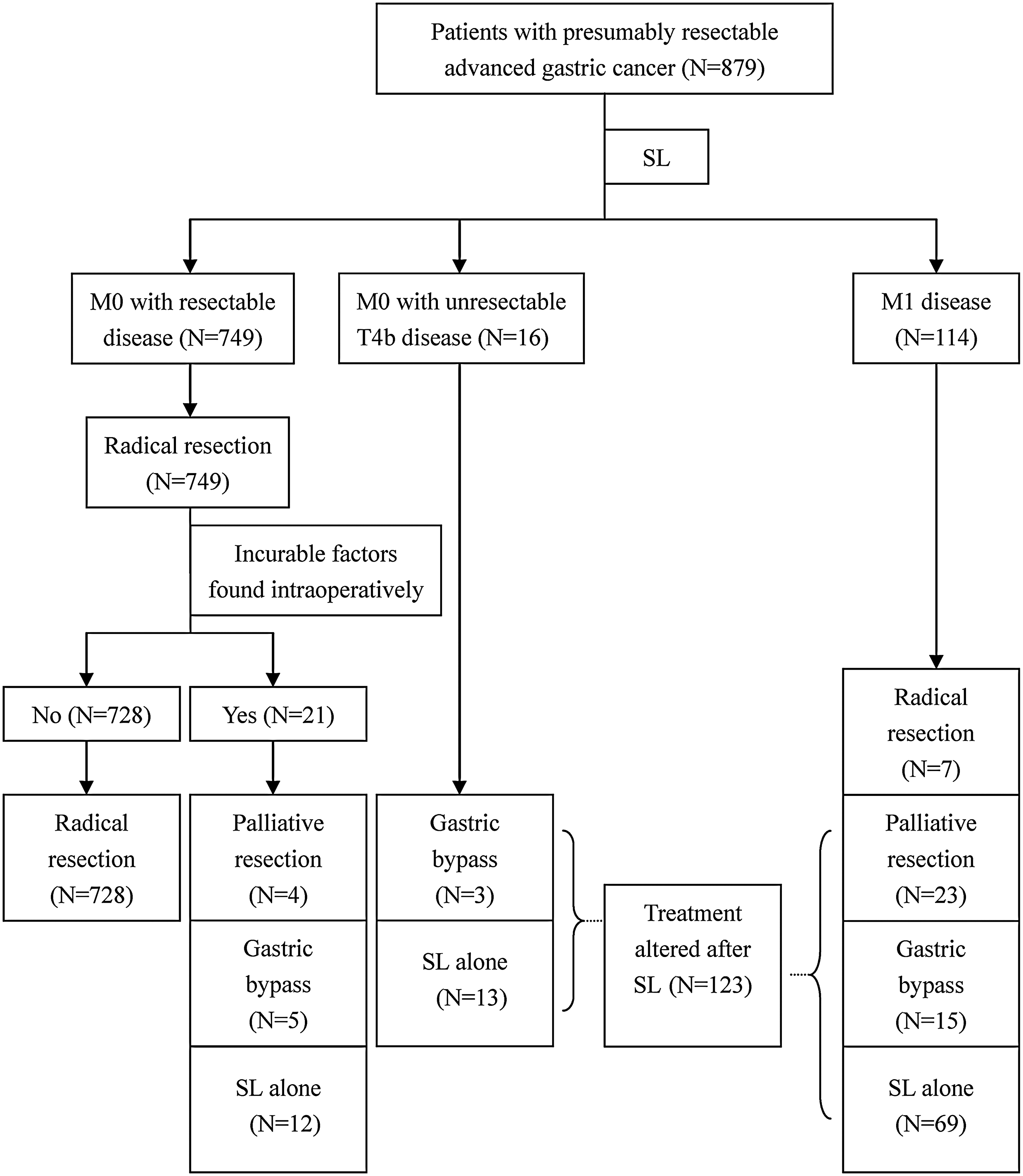
Treatment altered after staging laparoscopy. SL, staging laparoscopy.
False-negative rate of staging laparoscopy
Of the 749 patients who immediately proceeded to radical gastrectomy, 21 patients had new incurable factors at operation (Table 3), among which 4 underwent palliative resection, 5 underwent gastric bypass, and 12 were not offered further procedure and referred for chemotherapy (Fig. 1). The total false-negative rate was 2.8%.
Variables associated with peritoneal metastasis
Finally, peritoneal metastasis was verified in 110 patients (12.5%), including macroscopic peritoneal metastasis at SL (n = 92), positive peritoneal cytology (n = 10), and intraoperative findings of peritoneal metastasis (n = 8). The univariate analysis showed that the presence of peritoneal metastasis was correlated with tumor size, histological grade, Borrmann type, radiologic T stage, and radiologic N stage (Table 1). A multivariate regression analysis model was constructed to identify risk factors associated with peritoneal metastasis. We showed that tumor size ≥8 cm, Borrmann type III and IV pathology, and tumor invasion of T4a and T4b in EUS or CT scan were the predictive factors for peritoneal metastasis (Table 4).
Discussion
Despite the recent advances in imaging techniques, SL remains a useful tool for staging of AGC. It provides direct visualization of the tumor outer surface and peritoneal cavity, which is crucial in management, planning, and future treatment strategy. In previous studies, the yield of SL for AGC patients was limited to identification of M1 disease or peritoneal metastasis.6–8,10–12 However, in addition to M1 disease, SL can detect unresectable T4b disease, which also alters management, and can avoid unnecessary surgical resection. In our study, the yield of SL includes M1 and unresectable T4b diseases, which were defined as the incurable factors. To the best of our knowledge, the present study is the first to evaluate the value of SL in detecting both M1 and unresectable T4b diseases for AGC patients.
In this report, incurable factors were detected at SL in 14.8% patients. The yield in this study is much lower than that reported in previous studies (21%–36%).6,8,10,11 One putative explanation is that most patients in this study were planned to undergo laparoscopic radical resection, not a real sense of SL. Thus, many patients with a larger tumor and more advanced tumor stage received open surgery—who have a higher risk of possessing incurable factors. In our series, the proportions of patients with cT4b disease (5.2%) and a tumor size more than 8 cm (5.9%) are significantly lower compared with general AGC patients. If used for all AGC patients, SL might have a higher yield. In addition, the less aggressive pathophysiology of gastric cancer in Asian populations may be another explanation for the observed discrepancy.
The use of SL should be increased if its yield alters the treatment. In our study, the findings from SL altered management in 123 (14.0%) patients who would have otherwise undergone a radical resection for incurable disease. Early detection of peritoneal metastasis is important, in that unnecessary surgery can be avoided and systemic treatments initiated. In the present study, among the 130 patients with incurable factors identified at SL, 82 (63.1%) patients were not offered any further procedure and converted to chemotherapy. In addition to identification of incurable factors, detection of gastric outlet obstruction is another potential advantage of SL. In our series, 18 patients with incurable factors identified at SL underwent laparoscopic gastric bypass (gastrojejunostomy) due to the findings of gastric outlet obstruction.
An additional benefit of SL is that surgeons can obtain a final peritoneal cytology report before surgery by combining additional peritoneal lavage cytology. As for the incidence of peritoneal cytology, we focused on cytology results for patients with macroscopically negative peritoneal disease because these patients are the most likely to benefit from adding lavage cytology analysis to SL. Our study showed a low positive cytology rate of 4.7% (10/213), which is similar to the previous results.11–14 Notably, positive cytology did not alter the treatment plan in our study. Among the 10 patients with positive peritoneal cytology, 7 patients still underwent radical gastrectomy due to delayed report of peritoneal cytology results. The treatment of patients with positive peritoneal cytology in the absence of macroscopic metastasis has not yet been firmly established. Okabe et al. 15 reported that neoadjuvant chemotherapy was effective for patients with positive peritoneal cytology, while Kodera et al. 16 showed that adjuvant chemotherapy with S-1 after radical gastrectomy was also effective. Miki et al. 7 proposed that if macroscopic peritoneal metastasis was not detected at SL, gastrectomy should be generally performed to achieve cure, even when the result of peritoneal lavage cytology was positive. Based on the low rate of positive cytology and little effect on surgical treatment, we do not recommend peritoneal lavage cytology as a routine part of SL as we think it may not be unreasonable to conduct laparoscopic radical gastrectomy immediately after SL for patients without visible evidence of incurable factors.
At SL, we overlooked some incurable factors in 21 patients (2.8%), including infiltration of adjacent organs (n = 11), peritoneal metastasis (n = 8), and intrahepatic metastasis (n = 2). Pancreas, transverse mesocolon, and small bowel mesentery were the easily missed locations during laparoscopic exploration. In addition, peritoneal metastasis of posterior peritoneum and pelvic floor were not uncommon and should not be neglected. The false-negative rate in the present study (2.8%) was a little lower than those reported in previous studies (6.2%–17.2%).6,7,17–20 Besides the less aggressive pathophysiology of gastric cancer in Chinese populations, another possible explanation is that a systematic and painstaking inspection was introduced in our institute since 2011 and the bursa omentalis was routinely examined. Indeed, the false-negative rate was much higher before 2011 compared with after 2011 (16/204 versus 5/552). Some investigators did not recommend routine visualization of the bursa omentalis due to concerns about increased morbidity and difficulty in subsequent gastrectomy.14,21 In our series, however, we did not observe any related morbidity, and the subsequent gastrectomy did not seem to become more difficult. In light of the risks of direct invasion of pancreas and peritoneal metastasis of transverse mesocolon and omentum majus, we recommend visualization of the bursa omentalis as a routine part of laparoscopic exploration.
Although the efficacy of SL lies in detecting incurable factors in AGC patients, its indications for candidate suitability remain unclear. Western investigators are inclined to routine use of SL for all AGC patients who are candidates for surgical resection,8,14,18 while investigators from East Asia, a high prevalence region for gastric cancer, recommend SL to be selectively performed in those patients with high-risk factors of peritoneal metastasis.7,13,22 Our study showed that tumor size ≥8 cm, Borrmann type III and IV pathology, and tumor invasion of T4a and T4b in EUS or CT were significantly associated with higher rate of peritoneal metastasis, even after adjusting for potential profounding factors, which are similar to previous research findings.13,22,23 Hur et al. 22 thought that if SL was performed according to indications that were identified in their study (e.g., Borrmann type III and IV, tumor invasion depths of more than T3 according to CT scan, and tumor size of more than 4 cm), the yield of peritoneal metastasis would greatly improve from 12.2% to 24.0%. Thus, we also suggest SL to be performed in patients with high-risk factors, which can be preoperatively demonstrated by endoscopy.
The present retrospective study has several limitations. First, most laparoscopies in this study are not a typical form of SL, and some results of peritoneal cytology and biopsy from suspicious findings are reported after surgical procedure. Second, the study subjects are not all AGC patients with potentially resectable disease, but those who were about to undergo laparoscopic radical surgery. Thus, the yield of SL is underestimated. Third, preoperative radiologic staging was not uniform because of the extended study duration. Some of these patients received EUS staging, while others received CT staging.
In conclusion, SL is an effective tool in detecting additional incurable factors in AGC patients with potentially resectable disease and can alter their treatment strategy. Given that the total yield of SL is not high in our series, we recommend SL to be performed in selected patients with high-risk factors of peritoneal metastasis or equivocal imaging findings. We also recommend systematic and painstaking inspection of the whole abdominal cavity, including routine entry into the bursa omentalis, to improve the yield of SL.
Footnotes
Disclosure Statement
No competing financial interests exist.