
Abstract
Abstract
Introduction:
This systematic review and meta-analysis were designed to evaluated the efficacy and safety of stented versus stentless laparoscopic ureterolithotomy (LU).
Methods:
We conducted a systematic review and meta-analysis that included six trials that investigated the outcomes, including the rate of prolonged urine leakage, operative time, time to drain removal, and estimated blood loss, between stented versus stentless LU.
Results:
Four studies with 289 participants were included in the study. There was no significant difference between two groups in rate of prolonged urine leakage (odds ratios [OR] 0.35, 95% confidence intervals [CI] 0.09–1.46, p = 0.15). Significant longer operative time was detected in patients who underwent stented LU compared with stentless group (mean difference 11.36, 95% CI 7.53–15.20, P < .00001). There was no significant difference between two groups in day of drain removal (mean difference −1.09, 95% CI −2.33–0.15, P = .08). No significant difference in blood loss in patients who underwent stented LU compared with stentless group was detected (mean difference 7.67, 95% CI −0.29–15.64, P = .06).
Conclusion:
Our study demonstrated that the rate of prolonged urine leakage, time to drain removal, and estimated blood loss were not significantly different between stented and stentless LU.
Introduction
S
Retroperitoneal laparoscopic ureterolithotomy (LU) was first described by Wickham 3 and became a less invasive alternative to open surgery. In a review of the literature, 4 the main indication for LU indicates as a salvage procedure for failed ureteroscopy and SWL. Nevertheless, all these studies reported the use of laparoscopy as a primary procedure; even Gaur et al. 4 used it in 24 patients in the series.
Nowadays, placing a Double-J catheter after LU is still controversial. Some authors support the idea of inserting a Double-J (D-J) stent after the stone is removed to prevent urine leakage and ureteral stricture,5–7 but others oppose this idea, because D-J stenting has shown no correlation with the complication rate and increases the number of inconveniences to the patient, such as lower urinary tract symptoms, pain, and cost of cystoscopic removal of the D-J stent. 8 There are few studies9–12 that compared the efficacy and safety of stented versus stentless LU and, to our knowledge, there are no systematic reviews and meta-analysis that pooled the data and answer to this debate. Therefore, this systematic review and meta-analysis were designed to evaluate the efficacy and safety of stented versus stentless LU.
Materials and Methods
The review was conducted in accordance with the guidelines described by PRISMA. Eligibility criteria and study characteristics for studies being included were (1) patients had undergone LU for ureteral stone; (2) the study involved the comparison of a group in which DJ stent was used with a control group in which the patients had undergone stentless LU; and (3) the primary outcome was prolonged urine leakage, while the secondary outcomes were operation time, time to drain removal, and estimated blood loss.
Both English language studies and non-English language studies were included in the meta-analysis. The exclusion criteria for the study included patients with uncontrolled coagulation disorders, advanced cardiopulmonary diseases, stone associated with radiologically diagnosed ipsilateral stricture ureter, and patients with obstructed infected kidney.
Study identification and data abstraction
Two independent reviewers completed a systematic, computerized search of online databases, including PubMed, Ovid, MEDLINE, EMBASE, the Cochrane Controlled Trials Register, HealthSTAR, CINAHL, Google, and Google Scholar, for studies of safety of stented versus stentless LU in ureteral stones published in any language through October 2016. The keywords used for the search included LU, ureteral stone, Double-J, stent, and ureteral stone. Then, a MEDLINE search was refined to clinical trials. We also searched the Cochrane Database of Systematic Reviews, the Cochrane Central Register of Controlled Trials, www.Clinicaltrials.gov, Center watch (www.centerwatch.com), Trials Central www.trialscentral.org/ClinicalTrials.aspx), and The United Kingdom National Research Register (www.nrr.nhs.uk).
After reviewing the titles of the studies, we retrieved the abstracts if we felt they were appropriate for use in our study. We independently reviewed these abstracts and chose those studies that potentially were relevant to our work. We reviewed the bibliographies of all of the studies that were included to identify any additional studies that should be included.
Furthermore, we searched the archives of the meetings of The European Association of Urology, the American Urological Association, and the British Association of Urological Surgeons for other potential studies.
A data-extraction form was designed and agreed to by the authors. Initially, two authors independently extracted the data, which were later reviewed jointly to reach an agreement that the data were accurate. The data that were collected from all of the articles included the number of patients, mean age, mean follow-up, device used for incision, stone size, operative time, estimated blood loss, time to drain removal, analgesia requirements, hospital stay, and complications such as fever, ileus, and mild hematuria.
Disagreements were resolved by consensus or consultation with the senior authors. The authors of individual trials were contacted directly to provide additional information when necessary.
Statistical analysis
The Review Manager Database (Rev Man version 5.0, The Cochrane Collaboration 2008) was used to analyze the selected studies. Continuous data for each arm of a particular study were expressed as mean and standard deviation.
Dichotomous data were expressed as proportions or risks, with the treatment effect reported as a relative risk with 95% confidence intervals (95% CIs). The heterogeneity between the studies was assessed using the chi-squared test and the I2 statistic. The latter is a measure of the percentage of variation in the data that results from heterogeneity as opposed to chance. A p-value of < 0.1 and an I2 value >50% were considered suggestive of statistical heterogeneity, prompting a random-effects modeling estimate. Conversely, a nonsignificant chi-squared test result (P ≥ .1 and I2 ≤ 50%) only suggested that there was no evidence of heterogeneity; it did not necessarily imply that homogeneity existed because there may have been insufficient power to be able to detect heterogeneity. The Mantel–Haenszel method was used to combine the studies. If a significant heterogeneity was indicated (P < .1 and I2 > 50%), a random-effects model was used; if not, a fixed-effects model was used. In addition, funnel plots were constructed for the outcomes to assess publication bias, that is, the tendency not to publish studies with a negative result. The more asymmetric the funnel plot was, the more potential bias there was. Statistical significance was set at P < .05.
Results
Using our search terms, 64 references were identified. We excluded 60 of the studies after applying our eligibility criteria to their titles and/or abstracts, including exclusion of duplicates. The 4 studies left were included (Fig. 1). The eligible trials included four relevant comparisons (Table 1) involving 289 participants. We could not assess the differences in the outcomes such as costs, rate of postoperative ureteral stricture, and hospital stay, due to the lack of data.
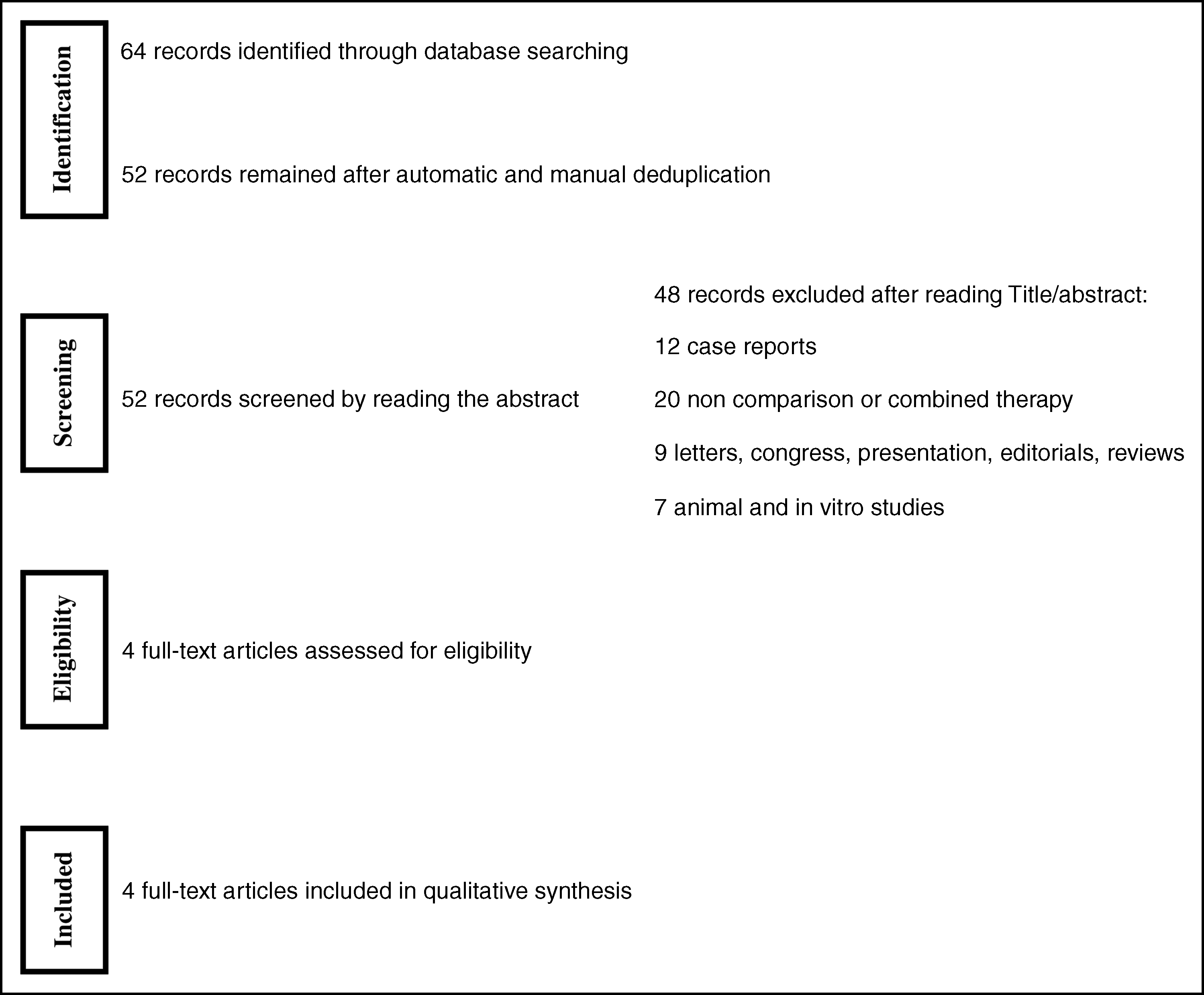
Flowchart of study selection.
group1: stented; group2: stentless.
Study presentations
Hammady et al. 9 in a randomized clinical trial, between May 2006 and May 2009, evaluated 104 LUs (with stent [n = 52] versus without stent [n = 52]), performed retroperitoneal. They incised the ureter directly over the stone longitudinally by L-hook electrode using the lowest cutting power and they closed ureterotomy by approximation of the periureteral sheath using interrupted intracorporeal laparoscopic suture with 4-0 polyglactin suture. For cases in which indwelling stent placement was planned, a 6F 26-cm polyurethane Double-J ureteral stent was inserted cystoscopically under fluoroscopy with the patient in the lithotomy position after LU. They followed up the patients for 6 months and showed that LU without stent placement for upper ureteral stones is safe, cost-effective, has less operative time, and needs no auxiliary procedures when compared with the use of stent placement after LU, which adds costs and discomfort for the patient.
Karami et al. 10 from May 2006 to November 2010 evaluated 46 patients (with stent [n = 23] versus without stent [n = 23]) who underwent transperitoneal LU. They incised the ureter directly over the stone longitudinally by L-hook electrode and they closed ureterotomy by approximation of the periureteral sheath using interrupted intracorporeal laparoscopic suture with 4-0 polyglactin suture. They followed up the patients for 12 months and concluded that placing a Double-J catheter during surgery does not increase the time of operation and may play a role in prevention of urinary extravasation after LU.
You et al. 11 retrospectively evaluated 41 patients who underwent retroperitoneal LU (with stent [n = 17] versus without stent [n = 24]) between January 2009 and January 2013. They incised the ureter directly over the stone longitudinally by cold knife and they closed ureterotomy by approximation of the periureteral sheath using interrupted intracorporeal suture by use of Vicryl 5-0. They followed the patients for 2 months and showed instead of operative time, no significant differences existed in estimated blood loss, hospital stay, and time to drain removal.
Srivastava et al. 12 evaluated 98 children who underwent transperitoneal LU (with stent [n = 50] versus without stent [n = 48]) from December 2009 to April 2012. They did not report with which device they incised the ureter, but they closed the ureterotomy with Vicryl 4–0 sutures. They followed their patients for at least a year and showed LU with stent differed from the stentless group in terms of more requirement of analgesics and the need for a second procedure for stent removal, but with no cases of urine leak in the postoperative period.
Meta-analysis
Prolonged urine leakage
We conducted fixed-effect meta-analyses because the results from studies reporting prolonged urine leakage after LU between stented and stentless groups showed no significant heterogeneity (P = .19). There was no significant difference between two groups in rate of prolonged urine leakage (odds ratios 0.35, 95% CI 0.09–1.46, P = .15) (Fig. 2).
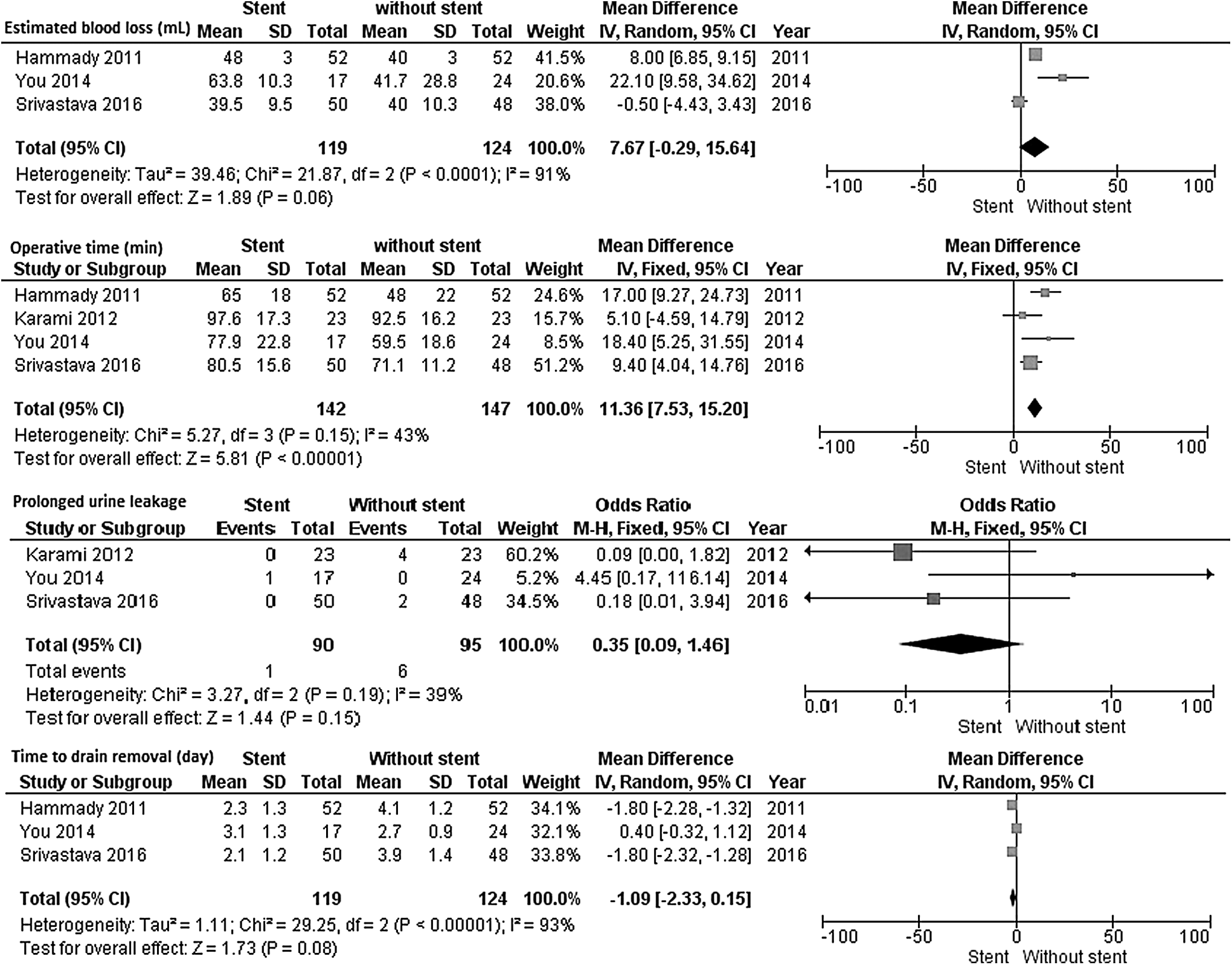
Comparison of stented versus stentless laparoscopic ureterolithotomy in estimated blood loss, operative time, prolonged urine leakage, and time to drain removal. CI, confidence interval; SD, standard deviation.
Operative time (minutes)
We conducted fixed-effect meta-analyses because the results from studies reporting operative time after LU between stented and stentless groups showed no significant heterogeneity (P = .15) (Fig. 3). A significantly longer operative time was detected in patients who underwent stented LU compared with the stentless group (mean difference 11.36, 95% CI 7.53–15.20, P < .00001) (Fig. 2).
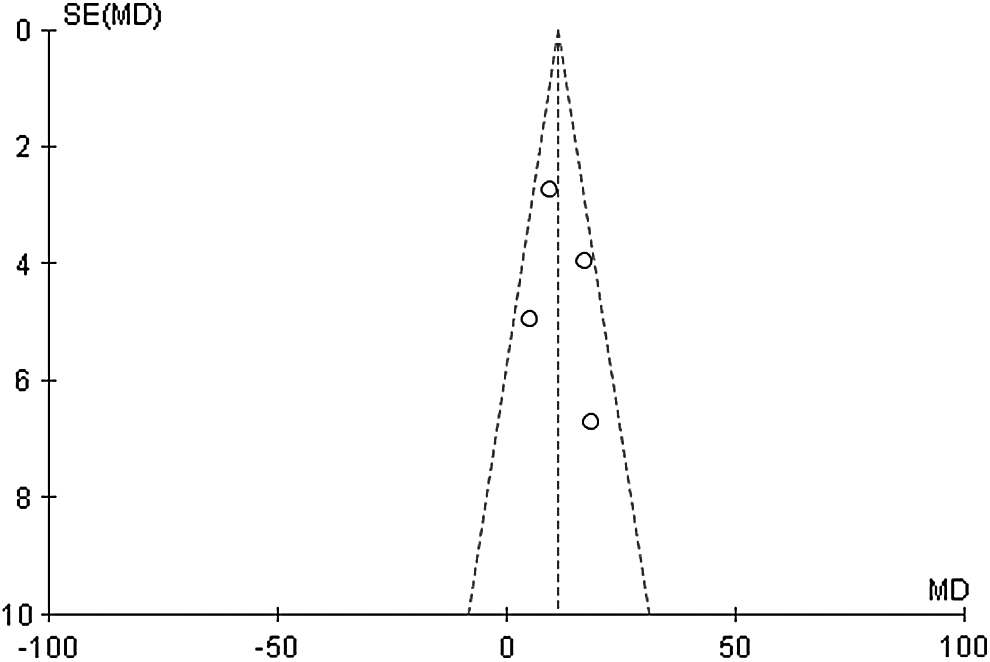
No significant heterogeneity in operative time in funnel plot.
Time to drain removal (day)
We conducted random-effect meta-analyses because the results from studies reporting time to drain removal after LU between stented and stentless groups showed significant heterogeneity (P < .001). There was no significant difference between two groups in day of drain removal (mean difference −1.09, 95% CI −2.33–0.15, P = .08).
Estimated blood loss (mL)
We conducted random-effect meta-analyses because the results from studies reporting time to drain removal after LU between stented and stentless groups showed significant heterogeneity (P < .001). There was no significant difference in blood loss in patients who underwent stented LU compared with stentless group (mean difference 7.67, 95% CI −0.29–15.64, P = .06).
Discussion
Our findings indicated that only operative time was significantly different between stented LU compared with stentless group. The rate of prolonged urine leakage, time to drain removal, and estimated blood loss were not significantly different between two groups.
With introducing modern endourology such as laparoscopic approaches, the use of open surgeries in ureteral stones is declined. However, many aspects of LU, including transperitoneal versus retroperitoneal approach and the necessity of stent insertion, are still on debate. Only few studies9–12 evaluated the efficacy and safety of stented LU compared with stentless LU and the lack of data absolutely exists; therefore, we could not assess the outcomes such as cost, rate of postoperative stricture, hospital stay, rate of conversion to open, and rate of complications such as fever, which may be related to a foreign device in the body such as Double-J.
Among included studies in this meta-analysis, two studies10,12 performed transperitoneal LU and other two studies9,11 the retroperitoneal approach. The transperitoneal approach has advantages such as wider working space, better visibility, and better identifiable anatomical landmarks. 13 Conversely, in the retroperitoneal approach, there is no need for colon mobilization and the risk for visceral organ injury is lower. In addition, the risk for contamination of the peritoneal cavity caused by postoperative urinary leakage and the rate of postoperative ileus are lower in this approach. 14 It might be because two included studies performed a transperitoneal approach that had a higher rate of prolonged urine leakage in the stentless group. However, this outcome was not significantly different between the two groups. Our result supported previous published studies.10–12
In our meta-analysis, operative time was significantly longer in stented LU compared with stentless. Our results supported previous findings.9,11,12 Hammady et al. 9 reported that the patients who underwent stented LU had 17 minutes of longer operative time versus stentless LU. In contrast, Karami et al. 10 found no significant longer operative time in stented compared with stentless LU. The reason might be extra time was used for repositioning of the patient and insertion of a Double J intraoperatively.
Time to drain removal is another important outcome. In our analysis, there is no significant difference between groups. However, significant heterogeneity exists among the included studies. It might be because of different guidelines in each center to remove the drain. In the study by Hammady et al., 9 they removed the drain and the drainage amount reached < 20 mL, but in another study, 10 this amount is < 50 mL per day.
In this meta-analysis, the estimated blood loss was not significantly different between stented versus stentless LU. This result is in agreement with previous findings.9,11,12 Significant heterogeneity existed between the included studies. It could be because of the difference in the method of estimation. No study reported how they assessed the estimated blood loss.
To our knowledge, our study is the first systematic review and meta-analysis that compared the safety and efficacy of the stented LU with stentless LU. Our study had some limitations: because of the lack of data we could not evaluate the outcomes such as cost, rate of postoperative stricture, hospital stay, rate of conversion to open, and rate of complications such as fever, ileus, and microscopic hematuria. The included study, instead of one of them that was a randomized clinical trial (RCT), 9 had no high-quality methodology, and therefore, there are many heterogeneities among the results. Studies by Srivastava et al. 12 and Karami et al. 10 included patients with stone burden >1.5 cm, but studies by Hammady et al. 9 and You et al. 11 included patients with stone burden >1 cm. These differences might make a bias in our results, and therefore, the results should be mentioned with caution.
Conclusion
Our study demonstrated that the rate of prolonged urine leakage, time to drain removal, and estimated blood loss were not significantly different between stented and stentless LU. In the future, more studies with high-quality methodology are warranted.
Footnotes
Disclosure Statement
No competing financial interests exist.