
Abstract
Abstract
Background:
Video assessment is an emerging tool for understanding variation in surgical technique.
Methods:
Representative videos of laparoscopic sleeve gastrectomy (LSG) were voluntarily submitted by 20 surgeons who participated in a statewide quality improvement collaborative. The amount of time required to complete the salient steps of the operation was measured and variations in the tasks performed during each step were captured.
Results:
Twenty-two videos of LSG were submitted and 11 videos included concurrent hiatal hernia repair. Data obtained from video analysis identified variation in time to complete each step of the procedure: prestapling dissection of stomach (5–25 minutes), gastric stapling (8–20 minutes), and management of the staple line (1–25 minutes). Time required to perform a hiatal hernia repair also varied (1–26 minutes), as did the type of repair: 55% were performed with a posterior cruropexy, 27% were performed with an anterior cruropexy, and 18% were performed with both. Ten different permutations of staple heights and buttressing material were used during division of the stomach with a gastric stapler. Management of the staple line included use of buttressing (64%), fibrin sealant (36%), oversewing (9%), surgical clips (18%), imbrication of the staple line (36%), and omentoplasty (55%).
Conclusions:
LSG technique is not uniform. Video analysis identified variation in (1) time to complete each step of the procedure, (2) hiatal hernia repair technique, (3) stapling technique, and (4) post-transection staple line management. Future efforts linking video analysis with clinical outcomes can provide objective evidence to support best practices.
Introduction
L
Assessing surgical videos has become an emerging tool for gathering empirical data on the technical aspects of a procedure. Data can be captured from video with more granularity and accuracy that surgeon surveys or operative reports because they do not rely on surgeon recall. Videos can also be reviewed in a blinded manner, which can eliminate bias. Birkmeyer et al. demonstrated that video-based peer-reviewed rating of skill while performing gastric bypass surgery correlated directly with complication, readmission, and reoperation rates. 9 However, their study did not take into account variations in technique, which represents the specific steps and the sequence of steps that take place during a procedure. This is an important distinction to make, given “how” you do an operation (i.e., operative technique) can affect “how well” you perform the procedure (i.e., surgical skill). A notable example of this concept is how a surgeon performs a bowel anastomosis. A laparoscopic hand-sewn anastomosis requires a different set of skills than using a circular stapler.
In this context, we aim to evaluate variation in sleeve gastrectomy technique by analyzing surgical videos from surgeons participating in a state-wide quality improvement collaborative. The goal of this study was to catalog details of the salient steps of an operation and determine whether a standard approach has been employed across a range of surgical practices.
Materials and Methods
Study population
In this study, 20 surgeons who participated in the Michigan Bariatric Surgery Collaborative (MBSC) voluntarily submitted a video of a typical LSG. The MBSC is a statewide consortium that includes 38 surgical programs and 70 surgeons. Participating programs submitted data to a clinical data registry (> 60,000 cases to date) and participated in quality improvement initiatives as well as quarterly meetings. The choice of video submitted was left entirely to surgeons and any patient identifiers were removed before submission. Video collection began in January 2015. The study was approved by the institutional review board of the University of Michigan and surgeons signed consent before participation.
Study design and data collected
Unedited videos were reviewed by a single surgeon (O.A.V.) who was blinded to the surgeon performing the procedure. The amount of time required to complete major steps of the operation was recorded. Major steps included (1) prestapling—all maneuvers involved in dividing the vasculature along the greater curve of the stomach and mobilization of the fundus; (2) stapling—all maneuvers involved in dividing the stomach; (3) poststapling—all maneuvers involved in managing the staple line after division of the stomach; and (4) hiatal hernia repair—all maneuvers involved during suture repair of the hiatal hernia (if present). To minimize the burden of video review, port placement, extraction of specimen, and port/skin closure were not included. Variation in the tasks performed during each step was also evaluated. These included use of buttressing material, fibrin sealant, oversewing, endoclips, imbrication of the staple line, leak test, placement of drains, and upper endoscopy. Timing of the hiatal hernia repair in relation to performing the gastrectomy (before versus after) was noted, as was the type of hiatal hernia repair (anterior repair, posterior repair, or both). Finally, stapler vendor (Covidien, Mansfield, MA and Ethicon Endo-Surgery, Cincinnati, OH), type of stapler cartridge (black, purple, or tan for Covidien; green, blue, or gold for Ethicon), and number of cartridges used were also recorded.
Analysis
The goal of this study was to evaluate the variation in time to complete the major steps of sleeve gastrectomy (prestapling, stapling, poststapling, and ±hiatal hernia repair). Mean time and ranges (minimum and maximum times) were calculated for each case. Descriptive statistics on variation in technique were provided for staple line management and hiatal hernia repair.
Results
Surgeon characteristics
Mean number of total sleeve gastrectomies per surgeon was 504 cases and ranged from 44 to 1722 cases during the study period. Mean age for surgeons participating in the study was 48 years (range 36–63 years) and 70% of surgeons practiced at a teaching hospital.
Operative technique
Time analysis
Mean total operative time for these cases was 85 minutes and ranged from 43 to 118 minutes. Individual time analysis for all surgical videos is presented in Figure 1. Mean time to complete major steps for all cases (n = 22) was 15 minutes (range 5–25 minutes) for prestapling steps, 13 minutes (range 8–20 minutes) for gastric stapling, 8 minutes (range 1–25 minutes) for poststapling steps, and 8 minutes (1–26 minutes) for suture repair of a hiatal hernia.

Hiatal hernia repair
Among cases involving hiatal hernia repair (n = 11), 55% were performed with a posterior cruropexy, 27% were performed with an anterior cruropexy, and 18% were performed with both. The majority of repairs occurred before gastric resection (64%; Fig. 2). Surgeons performing an anterior repair had a mean operative time of 3.3 minutes, whereas surgeons who performed a posterior repair or both an anterior and posterior repair had a mean operative time of 9 minutes. When compared with times for cases with no hiatal hernia, mean prestapling times were longer when a hiatal hernia repair was involved (17 minutes versus 14 minutes, respectively).
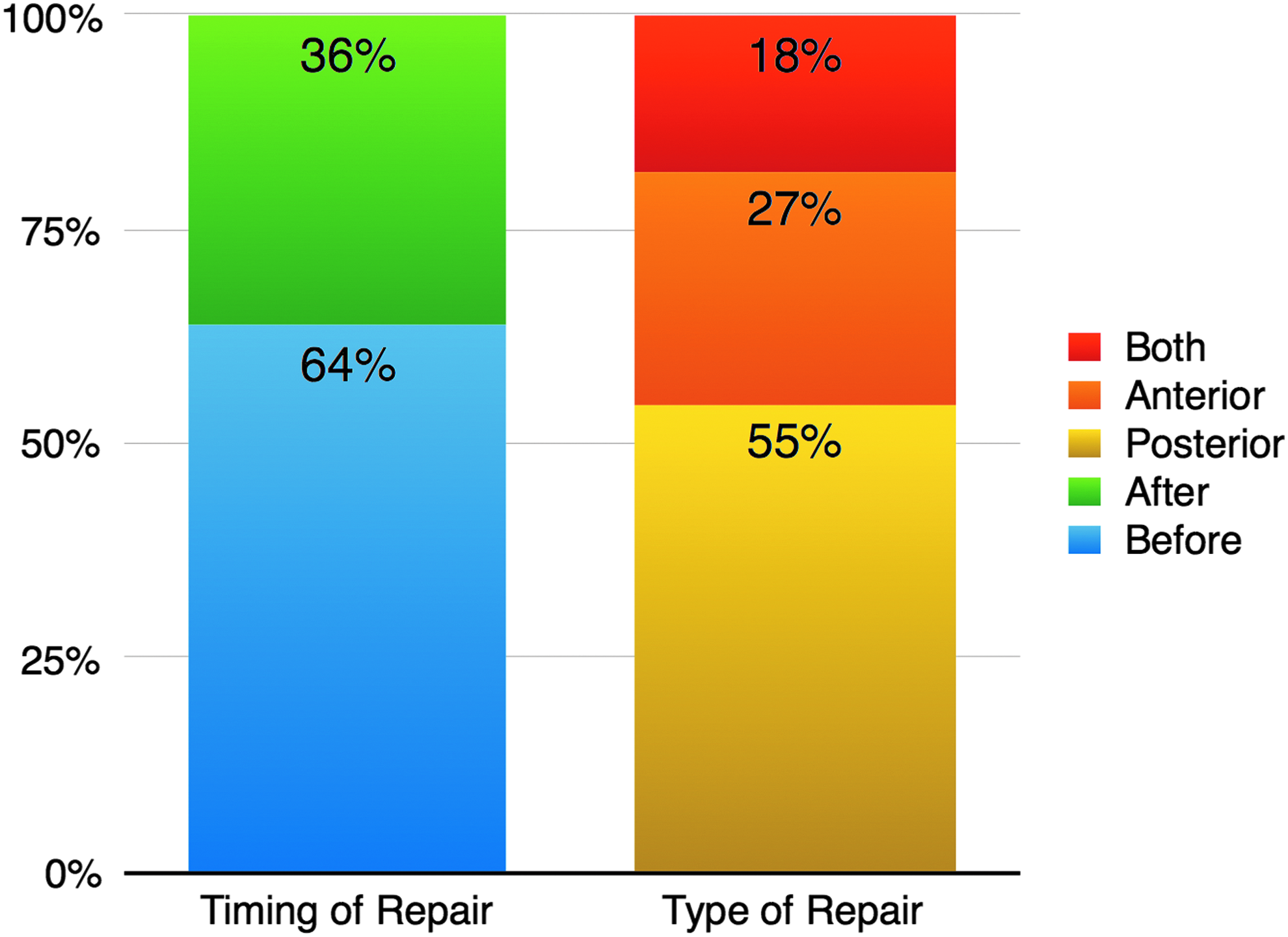
Timing and type of hiatal hernia repair.
Gastric stapling
Two different vendors (Covidien and Eithicon) were used for gastric stapling. Variation in staple cartridge and buttressing material used is presented in Figure 3. The median number of staple cartridges used was 6 (range 4–7). The most common staple load used overall was a green load with buttressing material (32%). The most common staple load for the first transgastric fire (closest to the pylorus) was also a green load with buttressing material (32%). The most common staple load for the final transgastric fire (closest to the gastroesophageal junction) was a purple load with no buttressing material (36%). Both the longest (20 minutes) and shortest (8 minutes) stapling times involved performing at least six staple fires and using buttressing material.

Variation in staple cartridge use and buttressing. *Covidien, ‡Ethicon.
Staple line management
Management of the staple line after gastric resection included use of buttressing (64%), fibrin sealant (36%), oversewing (9%), use of surgical clips (18%), imbrication of the staple line (36%), and omentoplasty (55%) (Table 1). The surgeons with the fastest poststapling operating time (1 minute) did not perform any additional maneuvers such as oversewing, leak test, endoscopy, or drain placement. The surgeon with the longest poststapling time (25 minutes) imbricated the staple line using an endostitch device, performed an omentoplasty, and left a drain but did not perform a leak test or endoscopy. Surgeons who performed free-hand suturing had a similar mean poststapling time when compared with surgeons who sutured with an endostitch device (5 minutes versus 4.7 minutes, respectively).
Discussion
Using surgical videos, our study identified significant variation in operative technique for sleeve gastrectomy. Variation was best demonstrated by identifying differences in (1) time to complete each step of the operation, (2) sequence in which the steps are completed, and (3) devices used to perform each step. Furthermore, comparing the shortest and longest operative times also revealed significant differences in technique. This is the first study to evaluate surgical videos of sleeve gastrectomy as part of a state-wide quality improvement initiative. Surgeons that submitted videos also varied in age, experience, and type of practice, thus offering a more robust evaluation of technique than a single-center study.
Operative time is often utilized as a proxy for surgical skill and has been associated with complication rates in several surgical disciplines.10–15 A common notion is that a shorter operation implies better skill and thus better outcomes. In a prior study conducted by the MBSC, Reames et al. demonstrated that median surgeon operative duration is independently associated with adjusted rates of adverse outcomes after laparoscopic gastric bypass. 16 However, it is unclear whether faster operative times represent better skill or a different technique (i.e., hand sewn versus circular stapled anastomosis). Interestingly, by using surgical videos, our study allowed us to identify technique-specific moments in which operative time was affected. The most notable example was during the poststapling step of the procedure, in which operative time ranged between 1 and 25 minutes. Shorter times often involved omission of certain steps (i.e., oversewing, leak test, and endoscopy) and were not necessarily performed with more efficiency or skill. Likewise, it is also possible that a surgeon with similar technique may have performed the steps of the operation in a shorter time but inadequately. For instance, surgeons may differ in their perception of “adequate” mobilization of the fundus before gastric transection and less mobilization may lead to a shorter operative time. Further evaluation of surgical video can shed light on this concept and will be vital before recommending best practices.
Variation in sleeve gastrectomy technique was most evident for steps of the procedure that are the most controversial. For example, choice of staple height and use of staple line reinforcement were highly variable in our study. Prior studies evaluating the use of buttressing material or oversewing of the staple line have been conflicting and are often mired by industry sponsorship or simply represent the technique of a single surgeon or institution.6,17–19 In a study evaluating the practices of an international panel of surgeons performing at least 500 sleeve gastrectomies each, the majority of surgeons agreed that it is not appropriate to use staples with closed height less than that of a blue load (1.5 mm) on any part of the sleeve gastrectomy and that of a green load (2.0 mm) when resecting the antrum. 4 Despite expert agreement, our study reveals that a wide range of staple heights (i.e., black to tan cartridges) were used along the stomach during transection. Although more data are necessary to resolve the issue, we agree with Huang et al. in that a single staple height cannot be used to appose the length of the gastric transection because of the variation in gastric wall thickness. 20 Other technical questions posed by the international consensus panel included location of the first and last staple fire (in relation to the pylorus and gastroesophageal junction), bougie size, mobilization of the fundus, and aggressive identification of a hiatal hernia. 4 Although our study was not designed to provide definitive answers for these questions, it does highlight the importance of using surgical videos to identify whether certain steps of a procedure are appropriate or even necessary to perform a sleeve gastrectomy safely. This concept is also imperative before recommending a “standard” approach to sleeve gastrectomy.
Video assessment of surgery has several limitations. First, obtaining and editing surgical videos are time and resource intensive. Videos must be captured in the operating room, placed on secure media devoid of patient metadata, converted to a specific file format, and then edited on separate software. Future studies utilizing video assessment of surgical videos will benefit from an integrated and possibly automated system. Evaluating laparoscopic videos also fails to measure communication and interactions among the surgical staff in the operating room, which may play a role in the outcome of a procedure.21–24 Nevertheless, examining time to complete various steps of an operation does provide insight into the cohesiveness of a surgical team. For example, we noted in our study that the fastest and slowest times for gastric stapling involved surgeons who used a similar technique (i.e., use of at least six staple fires with buttressing material). However, after reviewing the surgical video, it was evident that the surgeon with the longest stapling time was waiting much longer for the stapler to be reloaded than the surgeon with the shortest stapling time. This indicates a potential difference in the interaction between surgeon and assistant during the case. Finally, the videos submitted by surgeons only capture their operative technique and set of skills at that time, and do not account for evolution in their technique, improvements in the devices they use, or their learning curve. However, these data can be obtained easily by evaluating the variation between two separate videos from the same surgeon over a specific time period. These data can be invaluable when assessing the effect of surgical volume or a specific intervention, such as surgical coaching on technique, skill, and patient outcomes.
Surgical video has emerged as an effective tool to accelerate the learning curve among surgeons while minimizing harm to patients. It has been used in innovative ways to improve surgical skill as well as adopt new techniques. 25 In addition, videos can be used to establish a qualification system for assessment and accreditation. For example, Japan Society for Endoscopic Surgery has established the Endoscopic Surgical Skill Qualification System, which was designed to evaluate nonedited video of surgery by 2 judges in a double-blinded manner.26–28 Criteria for evaluation included setup, autonomy of operator, display of surgical field, recognition of surgical anatomy, co-operation of the surgical team, and procedure-specific criteria made to assess the operation in a step-by-step manner. Surgeons who were considered qualified by this video-based assessment experienced lower complication rates than those who failed, resulting in improvement of laparoscopic surgery through standardization. Given the variation in technique and complication rates for sleeve gastrectomy, our study suggests that a similar accreditation process is possible and has the potential to improve outcomes. Video-based data of technique can be further augmented with peer-reviewed assessment of skill and combined with a clinical outcomes registry such as the MBSC for a robust comparative analysis on the effect of operative techniques and surgical skill on outcomes, cost, and quality.
Conclusion
Video analysis of LSG identified considerable variation in operative technique. Videos provided a unique combination of time-based data as well as granular descriptive data, which demonstrated that common maneuvers such as gastric stapling, hiatal hernia repair, and staple line reinforcement are not performed uniformly. Further studies correlating technique and skill to clinical outcomes will be necessary to identify best practices.
Footnotes
Acknowledgment
This work was supported by Blue Cross Blue Shield of Michigan/Blue Care Network. The funding source had no involvement in collection, analysis, and interpretation of data; writing of the report; or in the decision to submit the article for publication.
Disclosure Statement
O.A.V., A.A.G., J.F.F., and J.B.D. receive salary support from Blue Cross Blue Shield of Michigan for participation in quality improvement initiatives within the Michigan Bariatric Surgery Collaborative.