
Abstract
Abstract
Background:
Patients with prior Roux-en-Y gastric bypass (RYGB) operations for weight loss present reconstruction challenges during a pancreaticoduodenectomy (PD). With over 60,000 RYGB performed annually, the increasing odds of encountering such patients during a PD make it imperative to understand the RYGB anatomy and anticipate reconstruction options. This article describes the possible reconstruction options and their rationale.
Methods:
We reviewed our PD reconstruction options, compared them to what have been described in the literature, and derived a consensus from internal conferences comprising bariatric and hepatopancreatobiliary surgeons to describe known reconstruction options.
Results:
In general, reconstruction options can include one of three options: (1) remnant gastrectomy, (2) preservation of gastric remnant, or (3) reversal of gastric bypass.
Conclusion:
This article describes individualized reconstruction options for RYGB patients undergoing PD. The reconstruction options can be tailored to the needs of the patient.
Introduction
O
It has also been estimated that one-third of all cancers in high-income countries may be attributable to factors related to obesity. 5 It has also been estimated that for every 5 kg/m2 increase in body mass index (BMI), the relative risk of pancreatic cancer increases by ∼10% or greater, and the relative increased risk of pancreatic cancer in obese patients (BMI >30) compared to normal BMI is 20%–50% higher. 6
Pancreaticoduodenectomy (PD) is performed for benign and malignant diseases of the pancreatic head. With the growing population of patients who have had RYGB, it is anticipated that a surgeon who performs the PD operation will at some point encounter this altered anatomy. The literature on patients undergoing PD after RYGB is limited. The goal of this article is to illustrate available options for reconstruction during PD after RYGB with their attendant risks and benefits.
Methods
We reviewed our PD reconstruction options after RYGB, compared them with what is known in the literature, and discussed these options (including their advantages and disadvantages) in multiple internal conferences consisting of bariatric and hepatopancreatobiliary surgeons. We generally grouped them into two reconstruction types: PD with remnant gastrectomy and PD without remnant gastrectomy. A final option is reversing the RYGB completely as part of re-establishing intestinal continuity after a PD.
Results
Reconstruction options
The available options for reconstruction can generally be with and without remnant gastrectomy, and there are circumstances in which these reconstruction options would be apt. The pertinent anatomy of an RYGB includes a small 20–30 cc gastric pouch, a Roux-limb of 75 to 200 cm in length, and a biliopancreatic (BP) limb that can be 20–50 cm from the ligament of Treitz (Fig. 1). The Roux-limb can be found in the retrocolic-retrogastric, retrocolic-antegastric, or antecolic-antegastric positions. The common mesenteric blood supply for the Roux-limb and the BP limb is the superior mesenteric artery.

Roux-en-Y gastric bypass anatomy. BP, biliopancreatic. © 2017 Emory University. Used with permission.
The pertinent steps of a PD include duodenal mobilization (Kocher maneuver), standard antrectomy (classic PD), dividing the duodenum at the ligament of Treitz, dividing the neck of the pancreas, resection of the common bile duct, and cholecystectomy. Re-establishing gastrointestinal continuity usually takes a variant of pancreaticojejunostomy (PJ), hepaticojejunostomy (HJ), and gastrojejunostomy, either as one continuous limb, or a BP limb that is separate from the gastrojejunostomy.
Reconstruction options with remnant gastrectomy
Along with the PD, a remnant gastrectomy avoids a new gastrointestinal anastomosis (Fig. 2a). The BP limb is used to create the PJ and the HJ. The goal is to ascertain adequate BP limb length to pass the limb through the retrocolic tunnel for the PJ and the HJ. This is also facilitated by the mobility of the jejunojejunostomy (JJ) and the common channel (CC). An advantage to this approach is earlier alimentary nutrient intake since the gastric pouch and the Roux-limb are never disrupted. A disadvantage would be difficulty in accessing the PJ or the HJ by percutaneous techniques through the gastric remnant, if there should ever be a need. This is our preferred approach, and in our experience (n = 3), these patients are able to begin alimentary intake sooner due to the lack of a recent enteroenterostomy and gastroenterostomy.
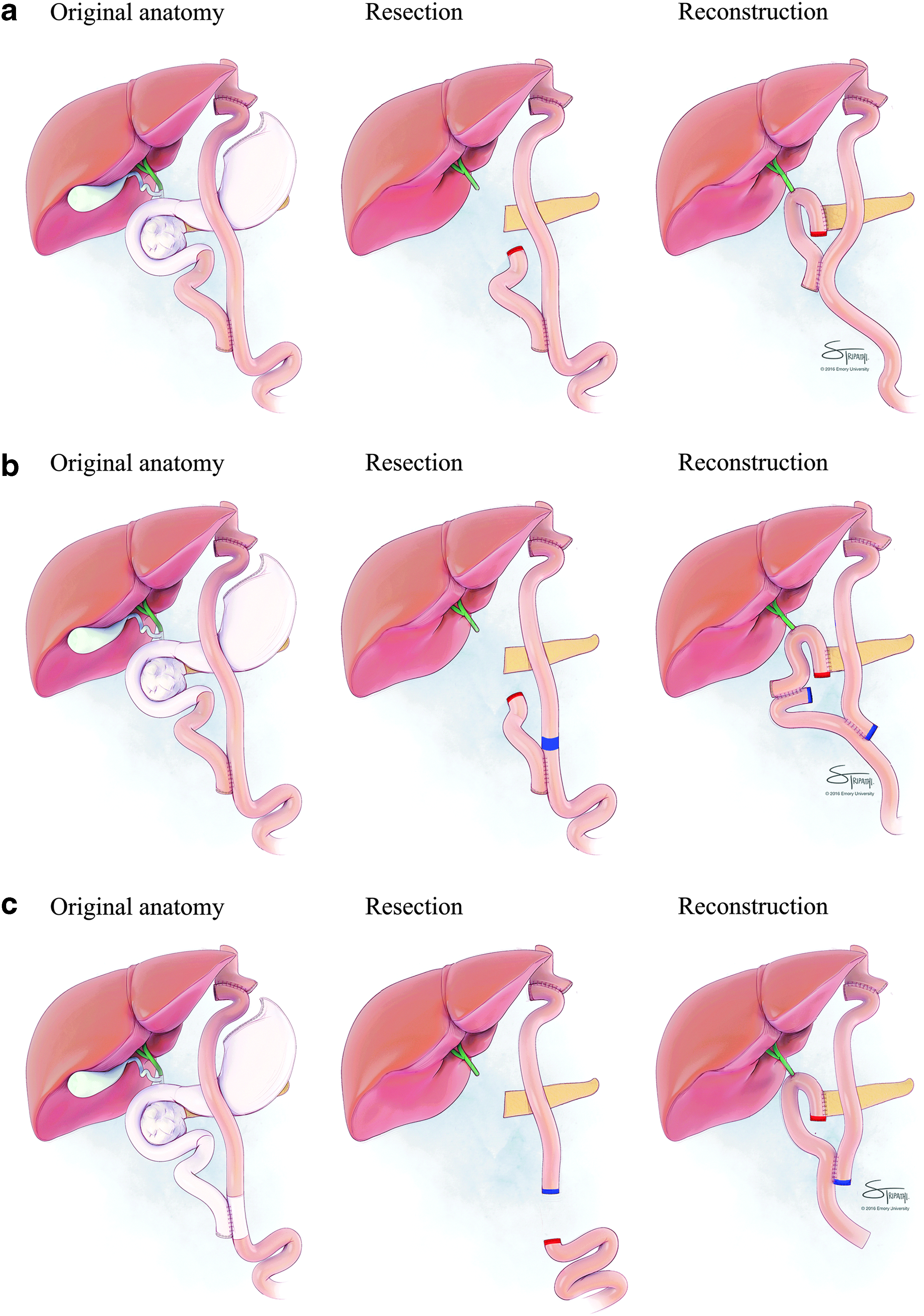
Reconstruction options with remnant gastrectomy.
If the BP limb is not long enough for passage through the retrocolic window to form the PJ and the HJ in a tension-free manner, the Roux-limb can be divided immediately proximal to the JJ (Fig. 2b). Division of the mesentery may be necessary to increase the mobility of the JJ and the distal small bowel. If necessary, it is important to err on the side of the Roux-limb while dividing the mesentery, to preserve the blood supply to the JJ. This will allow sufficient length for the BP limb to create a tension-free PJ and HJ. The transected end of the Roux-limb will be reanastomosed distally to form a new JJ and CC.
If the entire BP limb is insufficient in length or becomes unusable for some reason (e.g., ischemia), it is reasonable to resect the BP limb and the JJ along with the PD specimen (Fig. 2c). The divided bowel (immediately distal to the prior JJ) is passed through the retrocolic tunnel to form the PJ and the HJ. The distal end of the Roux-limb is then anastomosed to the small bowel further distally to form a new JJ and CC.
Reconstruction options without remnant gastrectomy
If the gastric remnant is to be preserved, it can be anastomosed to the BP limb as well (Fig. 3a). A gastrostomy tube (G-tube) in this setting can be placed for decompression and future access to the BP anastomoses, rather than for nutritional support due to the proximity of partially digested nutrients to the HJ anastomosis.
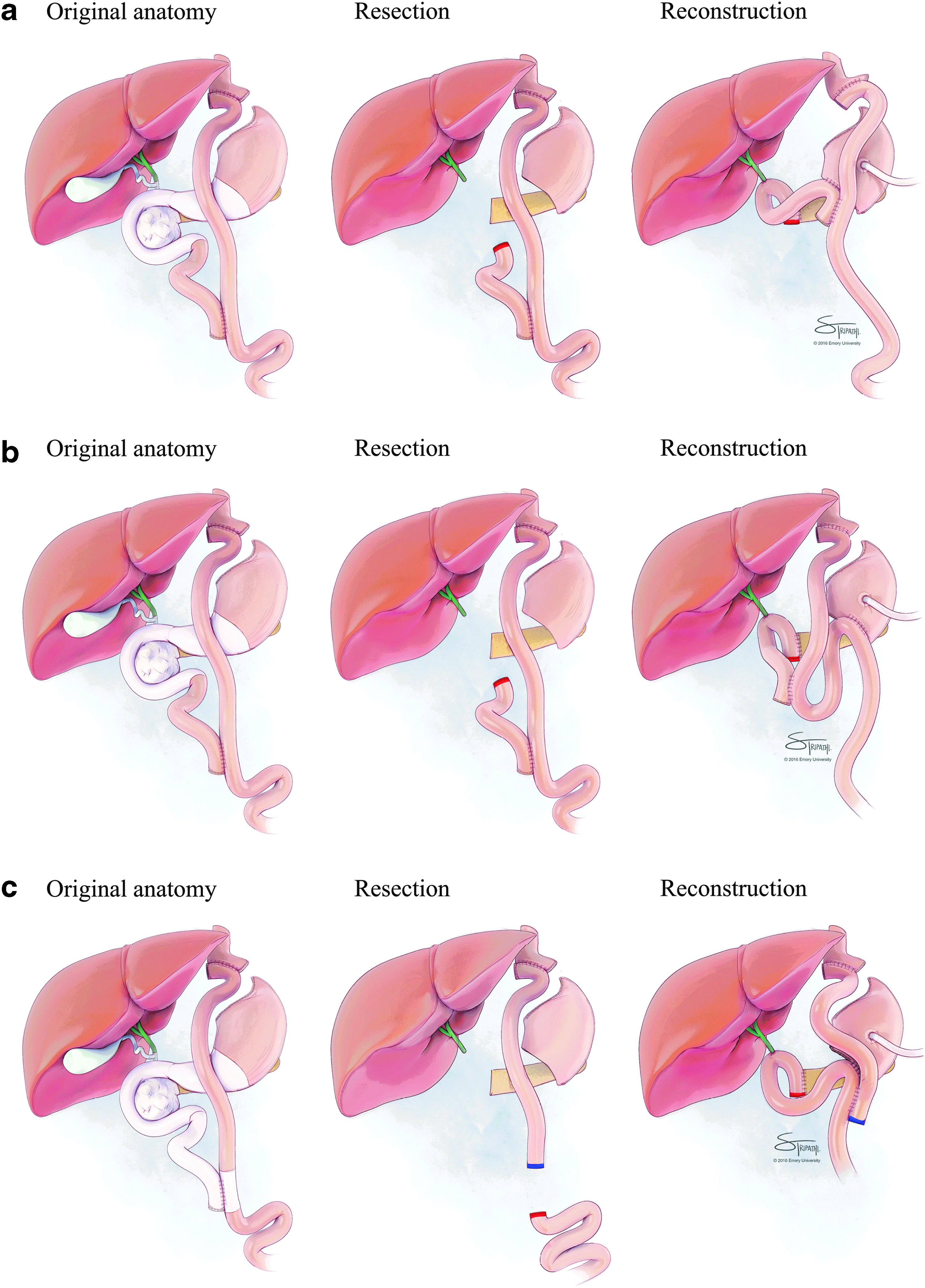
Reconstruction options without remnant gastrectomy.
Drainage of the gastric remnant may be accomplished by anastomosis to the CC instead of the BP limb (Fig. 3b). In this study, the G-tube may be used more liberally for enteral nutrition because the alimentary limb is separate from the BP anastomoses.
A variation of the PD includes resection of the BP limb and the JJ (Fig. 3c). The divided bowel (immediately distal to the prior JJ) is used for the PJ, the HJ and the gastrojejunostomy to drain the gastric remnant. The end of the Roux-limb is anastomosed to this limb of the small bowel to form a new JJ and CC. This is a configuration, similar to what was described earlier (Fig. 2c), with the addition of an anastomosis to drain the remnant. Also, this reconstruction is a great option if the BP limb becomes unusable during the reconstruction (Fig. 3a,b).
Reconstruction options with reversal of gastric bypass
Reversal of the gastric bypass is an option. Reversal of gastric bypass does add significant complexity to the case. However, it may be an occasional consideration. Placement of a G-tube is potentially a very helpful low-risk measure in such patients, and can be used for multiple reasons including nutrition.
In reversing the gastric bypass, the Roux-limb is disconnected from the gastrojejunostomy and the gastric pouch is anastomosed to the gastric remnant (Fig. 4a). The gastrogastrostomy is performed using a linear stapler, handsewn anastomosis, or circular end-to-end anastomosis. The Roux-limb is used for the PJ and the HJ, and also to drain the gastric remnant (now anastomosed to the gastric pouch) with a new gastrojejunostomy. This reconstruction functionally results in a configuration similar to a patient with no history of RYGB. This more complex option may be considered for those who may need a larger volume gastric reservoir for oral intake, although there is no guarantee that the stomach will be physiologically functional (e.g., acid production, grinding, and breakdown of nutrients).

Reconstruction options with reversal of gastric bypass.
If the BP limb is preserved during the PD with intent to reverse the gastric bypass, the Roux-limb is disconnected at the gastrojejunostomy, and the gastric pouch is anastomosed to the gastric remnant (Fig. 4b). The BP limb is used for the PJ and the HJ, and the Roux-limb is used to drain the gastric remnant (now anastomosed to the gastric pouch). This configuration also separates the alimentary tract from the BP anastomoses.
Discussion
In RYGB patients undergoing a PD, we prefer reconstruction that includes remnant gastrectomy because it avoids the morbidity of an additional gastrointestinal anastomosis (such as bleeding, leak, ulceration). In theory, the anastomosis is constantly being exposed to the acid-producing gastric remnant, but this occurs in standard PD reconstructions as well, and is mitigated by the addition of proton pump inhibitors. Furthermore, there is literature showing the gastric remnant being a potential source of increased morbidity. 7 With remnant gastrectomy, there is no possibility of postoperative delayed gastric emptying, which can be as high as 18% after PD. 8 If enteral nutrition is ever required after a remnant gastrectomy, a percutaneous jejunostomy tube can be placed in the Roux-limb or the CC. A potential disadvantage of a remnant gastrectomy is a lack of endoscopic gastric access to the HJ and PJ if the need should ever arise.
There are certain situations where it may be exceedingly difficult to perform the remnant gastrectomy. Examples are in patients who have had a prior anastomotic leak or abscess after RYGB, if the patient has had revisional or reoperative surgery after RYGB, or if the patient has undergone preoperative radiation therapy. In such situations, it is reasonable to leave the gastric remnant and drain it with an additional anastomosis (Figs. 3, 4). Routine placement of a G-tube in the remnant is probably a wise decision with any revision or reoperation after RYGB as it may facilitate decompression in the early postoperative period in a nonfunctional gastric remnant. It also allows easier access to the remnant and the anastomoses (gastrointestinal, PJ and HJ). In addition, the gastrojejunostomy can be imaged with contrast through the G-tube, and also facilitates future radiologic placement of a G-tube.
Rutkoski et al. described a case report where the remnant gastrectomy was not performed. 9 The BP limb was anastomosed to the gastric remnant, and a second Roux-limb was created from the CC (distal to the JJ) that formed the PJ and the HJ. The gastric remnant was preserved for potential future nutritional access by G-tube. The possible drawbacks include additional anastomosis and slight risk of marginal ulceration, which are valid concerns due to anastomosis being a part of the acid producing gastric remnant. We would like to underscore that this reconstruction has the disadvantage of two additional anastomoses (gastrojejunostomy and the new JJ) and an additional staple line (new Roux-limb). Furthermore, the gastric remnant is essentially nonfunctional with no direct endoscopic access to the gastrojejunostomy or the gastric remnant.
Khithani et al. and Nikfarjam et al. each reported two such patients who underwent reconstruction during PD similar to our preferred approach (Fig. 2a), with excellent postoperative outcomes.10,11 De la Cruz-Munoz et al. reported a case of such a patient who underwent laparoscopic PD after LRYGB. 12 Swain et al. describes four such patients, of whom three underwent reconstruction during PD that mirrors our desired approach. 13 They describe two options that are not depicted in our illustrations:
One option of reconstruction described in the article by Swain et al. is using the Roux-limb, which is the alimentary limb, for the HJ and the PJ. In our opinion, this form of reconstruction predisposes to recurrent cholangitis and pancreatitis due to the passage of partially digested nutrients through these anastomoses, which we have observed in the past in some patients with choledochoduodenostomy. Moreover, if this reconstruction was complicated by a leak from the HJ or the PJ, the patient's alimentary limb would essentially be nonfunctional compelling the patient to be NPO until resolution or intervention. Finally, the patient with such a reconstruction is at risk for significant bile reflux. Theoretically, using the Roux-limb for these deep anastomoses may result in kinking of the alimentary limb due to its position relative to the colon and stomach (i.e., in front or behind).
The other option, where the Roux-limb is transected proximal to the prior JJ and a new Roux-limb is created for the PJ and the HJ anastomoses with creation of a new enteroenterostomy proximal to the prior JJ, is more convoluted in the setting where remnant gastrectomy is performed. We say that because it not only adds an extra staple line (prior JJ) but also creates at least one potential site of internal hernia.
Theodoropoulos et al. reported a case, where remnant gastrectomy could not be performed due to prior open RYGB followed by another laparotomy for revision due to marginal ulceration, perforation of the gastric pouch, and gastrogastric fistula. 14 After the PD, the BP limb required resection due to ischemia. The reconstruction performed by the authors involved using the existing Roux-limb to form the gastrojejunostomy (with the gastric remnant), the PJ, and the HJ. In our opinion, this is not an optimal form of reconstruction because it predisposes to recurrent cholangitis or pancreatitis, and results in a nonfunctional alimentary tract in the case of a leak. The configuration may also result in kinking of the small bowel. Also, the nonfunctional gastric remnant may act as a diverticulum.
Helmick et al. reported two such patients where the gastric remnant was preserved. 15 Reconstruction was similar to Figure 3a, and appropriate emphasis was made on placement of a venting G-tube. It appears that remnant gastrectomy was not performed for potential enteral nutrition access. We wish to highlight that the G-tube should not be used for nutritional support as it would potentially result in recurrent cholangitis and pancreatitis, owing to the close proximity of the passage of partially digested nutrients to the bilioenteric anastomosis and PJ. Hatzaras et al. reported two options of reconstruction with remnant gastrectomy and one option of reconstruction without remnant gastrectomy (similar to the case report by Rutkoski et al.) appropriately conveying the message to drain the gastric remnant. 16
Barbour et al. reported a series of five patients who underwent pancreatic resection in the form of distal pancreatectomy or duodenal preserving pancreatic head resection (DPPHR), but not PD, after RYGB. 17 To discuss the reconstruction options after DPPHR is beyond the scope of our article. However, the illustrations and concepts detailed in the current article are valuable in planning for reconstruction after DPPHR.
In summary, of the 13 patients that have been described in the literature who underwent PD after RYGB, 7 (54%) of these patients underwent reconstruction, similar to our preferred approach (Fig. 2), which involved remnant gastrectomy with the BP limb forming the BP anastomoses. Overall, 8 (61.5%) of the 13 patients had remnant gastrectomy. Five patients did not have a remnant gastrectomy. There are 10 patients in the literature where the surgeon attempted resecting the gastric remnant, and 8 (80%) of these patients had successful remnant gastrectomy. However, based on the published literature, this is clearly a small sampling of what might have actually been performed. We have had three such patients where we performed PD in patients with prior RYGB (similar to Fig. 2a). In all patients, we had adequate BP limb length for the anastomoses. The patients had early recovery of bowel function and were discharged from the hospital on or before postoperative day 5 without any significant complications.
Conclusion
This article, with its accompanying review of the existing literature, offers individualized reconstruction options for RYGB patients undergoing PD. The availability of bariatric surgeons who are familiar with the anatomy, and their experience with revisional and reoperative bariatric surgery can also be resources for decision-making.
Footnotes
Acknowledgment
M.M.S. and B.M.M. were supported, in part, by the Foundation for Surgical Fellowships.
Authorship Contribution
Each author has significantly contributed to the article as follows:
• Substantial contributions to the conception or design of the work • Drafting the work and revising it critically for important intellectual content • Final approval of the version to be published • Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Disclosure Statement
No competing financial interests exist.