
Abstract
Abstract
Aim:
This meta-analysis aims to compare hand-assisted laparoscopic surgery (HALS) with conventional laparoscopic surgery (LAS) for colorectal cancer (CRC) in terms of intraoperative, postoperative, and survival outcomes.
Materials and Methods:
A systematic literature search with no limits was performed in PubMed, Embase, and Medline. The last search was performed on March 31, 2017. The outcomes of interests included intraoperative outcomes (operative time, blood loss, length of incision, transfusion, conversion, and lymph nodes harvested), postoperative outcomes (length of hospital stay, time to first flatus, time to first bowel movement, postoperative complications, mortality, reoperation, ileus, anastomotic leakage, postoperative bleeding, wound infection, intra-abdominal abscess, urinary complication, cardiopulmonary complication, and readmission), and 5-year survival outcomes.
Results:
Nine articles published between 2007 and 2016 with a total of 1307 patients were enrolled in this meta-analysis. HALS was associated with longer length of incision. No differences were found for operative time, blood loss, transfusion, conversion, lymph nodes harvested, length of hospital stay, time to first flatus, time to first bowel movement, postoperative complications, mortality, reoperation, ileus, anastomotic leakage, postoperative bleeding, wound infection, intra-abdominal abscess, urinary complication, cardiopulmonary complication, readmission, or 5-year survival outcomes.
Conclusion:
Our meta-analysis demonstrated that HALS is similar to LAS for CRC surgery in terms of intraoperative, postoperative, and survival outcomes except for the longer length of incision.
Introduction
C
However, laparoscopic surgery also has disadvantages and limitations in colectomy and rectectomy such as longer operative time, steep learning curve, and risk of recurrence at the port site. 13 Besides, it is not easy to dissect when it comes to bulky or complex tumors especially in pelvic cavity for the lack of tactile feedback, normal stereoscopic vision, and enough exposure. 13 Those conditions have promoted the proposition and development of hand-assisted laparoscopic surgery (HALS) for CRC. 13
HALS for CRC was first reported in 1994. 14 When performing HALS for CRC, surgeons can place a hand into the abdomen through a hand access device to help visualization, retraction, and dissection without disturbing the pneumoperitoneum.7,13,15,16 It is a novel and efficient technique which combines the advantages of conventional laparoscopic and open surgery. 17 Some articles revealed that HALS was superior to LAS in terms of intraoperative or postoperative outcomes of CRC,18,19 while some other studies suggested they were similar7,20,21 although HALS was safe and feasible. 13 There still lacks sufficient evidence to evaluate which technique is more beneficial to patients with CRC. Therefore, we conducted a meta-analysis to compare HALS and LAS in terms of intraoperative, postoperative, and survival outcomes.
Materials and Methods
Study selection
We performed a literature search in PubMed, Embase, and Medline for studies comparing HALS and LAS in CRC surgery. The search terms included “hand-assisted laparoscopic surgery or hand-assisted laparoscopy” and “laparoscopies, laparoscopic, or laparoscopy” and “colon cancer, rectal cancer, or colorectal cancer.” The last search was performed on March 31, 2017. We also performed a manual search of references of articles and reviews for additional potentially eligible studies.
Inclusion and exclusion criteria
The inclusion criteria for this meta-analysis were as follows: (1) Case–control study (HALS versus LAP), (2) CRC, (3) Studies with total sample size more than 20, and (4) Intraoperative and/or postoperative outcomes were reported. The exclusion criteria studies were as follows: (1) review articles, (2) correspondences, (3) studies, including benign diseases such as colorectal polyps, (4) animal studies, (5) single-arm studies, (6) studies not in English, and (7) any study comparing hand assist for diagnosis other than CRC.
Data extraction
Two authors (X.Z. and Q.W.) reviewed all the identified articles independently. They would solve the discrepancies by discussion first and a third reviewer (Z.W.) would be required if necessary. We extracted the following items from each study: correspondence author's name, year of publication, country, publication type, study type, bowel preparation, location of disease, number of patients in each arm, gender, age, body mass index (BMI), previous abdominal surgery (PAS), and outcomes of interests.
Outcomes of interests
Intraoperative outcomes: operative time, blood loss, length of incision, transfusion, conversion, and lymph nodes harvested.
Postoperative outcomes: length of hospital stay, time to first flatus, time to first bowel movement, postoperative complications, mortality, reoperation, ileus, anastomotic leakage, postoperative bleeding, wound infection, intra-abdominal abscess, urinary complication, cardiopulmonary complication, and readmission.
Survival outcomes: 5-year disease-free survival and 5-year overall survival.
Quality assessment
The methodological quality of the enrolled retrospective studies was assessed using the revised and modified grading system of the Scottish Intercollegiate Guidelines Network. 22 Articles achieving < 8 scores, 8–14 scores, and more than 14 scores (total score, 20) were defined as poor quality, fair quality, and good quality, respectively. And the methodological quality of the randomized controlled trials was assessed by modified Jadad score system (total score, 5; 1–2, low quality; 3–5, high quality). 23
Statistical analysis
All data analyses were conducted using the Review Manager version 5.0 (The Cochrane Collaboration, Software Update, Oxford), and P < .05 was considered statistically significant. Weighted mean difference (WMD) was calculated for the continuous outcomes, and pooled odds ratios (ORs) or risk ratios were calculated for the dichotomous outcomes. For continuous outcomes, if the study only provided means and range values or median and range values, the means and standard deviations were calculated using methods described by Hozo et al. 24 Chi-squared test and Higgins I-squared test were used for heterogeneity test. A value of P < .05 and I2 > 50% was regarded as existing heterogeneity. If I2 > 50% and P < .05, a random-effects model was applied. Correspondingly, if I2 < 50% and P > .05, a fixed-effects model was applied. Begg's funnel plot was used to evaluate publication bias. The survival curves in articles were obtained by Engauge Digitizer version 4.1.
Results
The process and result of literature searching are shown in Figure 1. The initial search algorithm retrieved a total of 897 studies. There remained 368 studies after removing the duplications. After reviewing titles and abstracts, only 22 relevant studies were kept for further evaluation. Besides, no additional record was identified through manual search. Among these studies, 13 literatures were excluded due to following reasons: 1 study was not in English, 9 studies included benign diseases, 2 studies compared HALS and open surgery, and 1 study's sample size was too small. Finally, 9 articles25–33 published between 2007 and 2016 were included in our meta-analysis. One of 9 articles was randomized controlled trial. 28 The characteristics of the included studies are summarized in Table 1. A total of 1307 patients (672 by HALS and 635 by LAS) were enrolled.
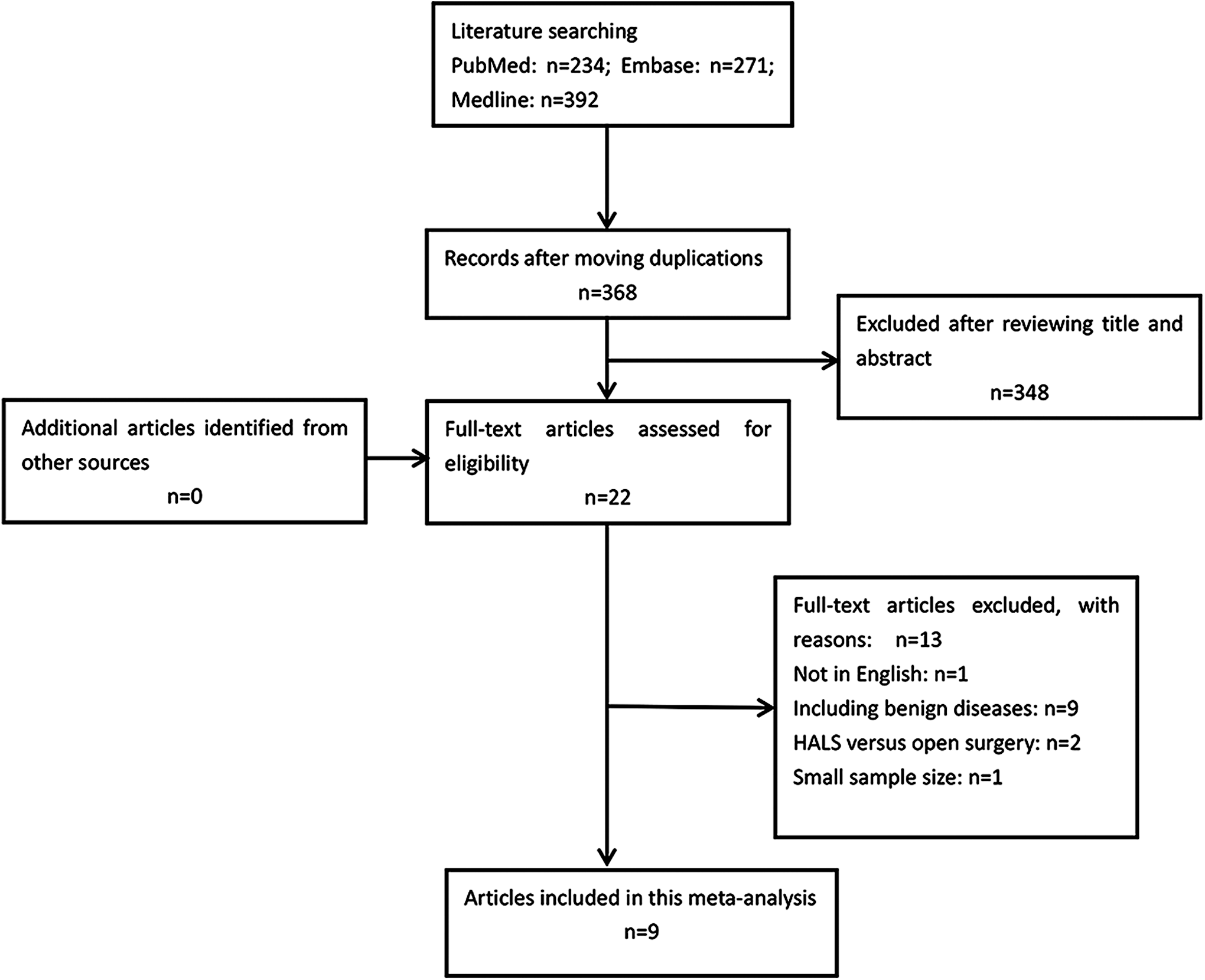
Prisma diagram. HALS, hand-assisted laparoscopic surgery.
APR, abdominoperineal resection; AR, anterior resection; BMI, body mass index; HALS, hand-assisted laparoscopic surgery; HO, Hartmann's operation; IR, intersphincteric resection; LAR, low anterior resection; LAS, laparoscopic surgery; LC, left colectomy; NR, not reported; PAS, previous abdominal surgery; PNCT, prospective nonrandomized controlled trials; PRCT, prospective randomized controlled trials; RC, right colectomy; RCCS, retrospective case–control study.
Patient demographics
There was no significant difference between two groups in age (P = .82, WMD = −0.14, 95% confidence interval [CI] [−1.30 to 1.03], I2 = 0%), male gender (P = .60, WMD = 1.13, 95% CI [0.73 to 1.75], I2 = 56%), BMI (P = .80, WMD = 0.11, 95% CI [−0.74 to 0.96], I2 = 67%), or PAS (P = .06, OR = 1.42, 95% CI [0.99 to 2.03], I2 = 0%). In addition, surgical procedures and tumor stage were similar in both groups.
Quality of included studies
The scores of methodological quality assessment of the enrolled retrospective studies and randomized controlled trial are shown in Tables 2 and 3. Of those 9 articles, 7 retrospective studies had fair quality (11–13 scores)25–27, 29–32 and one randomized controlled trial had low quality (2 scores). 28 What's more, Chan's study 33 was prospective but not randomized so we didn't assess the quality.
Total scores, 20; <8, poor quality; 8–14, fair quality; >14, good quality. HALS, hand-assisted laparoscopic surgery.
A total modified Jadad score of 1–2, low quality trial; 3–5, high quality trial.
1, reported; 0, not reported.
Meta-analysis of intraoperative outcomes
The analytic results demonstrated that there were no statistically significant differences between HALS and LAS in terms of operative time (P = .19, WMD = −7.90, 95% CI [−19.58 to 3.78], I2 = 77%), lymph node harvested (P = .42, WMD = 1.00, 95% CI [−1.45 to 3.45], I2 = 74%), conversion (P = .56, OR = 0.68, 95% CI [0.18 to 2.51], I2 = 59%), blood loss (P = .88, WMD = 4.82, 95% CI [−56.23 to 65.87], I2 = 83%), or blood transfusion (P = .85, OR = 0.93, 95% CI [0.44 to 1.94], I2 = 0%). However, we observed a significant longer length of incision (P < .001, WMD = 2.32, 95% CI [1.06 to 3.58], I2 = 96%) in HALS group although there existed heterogeneity (Fig. 2).
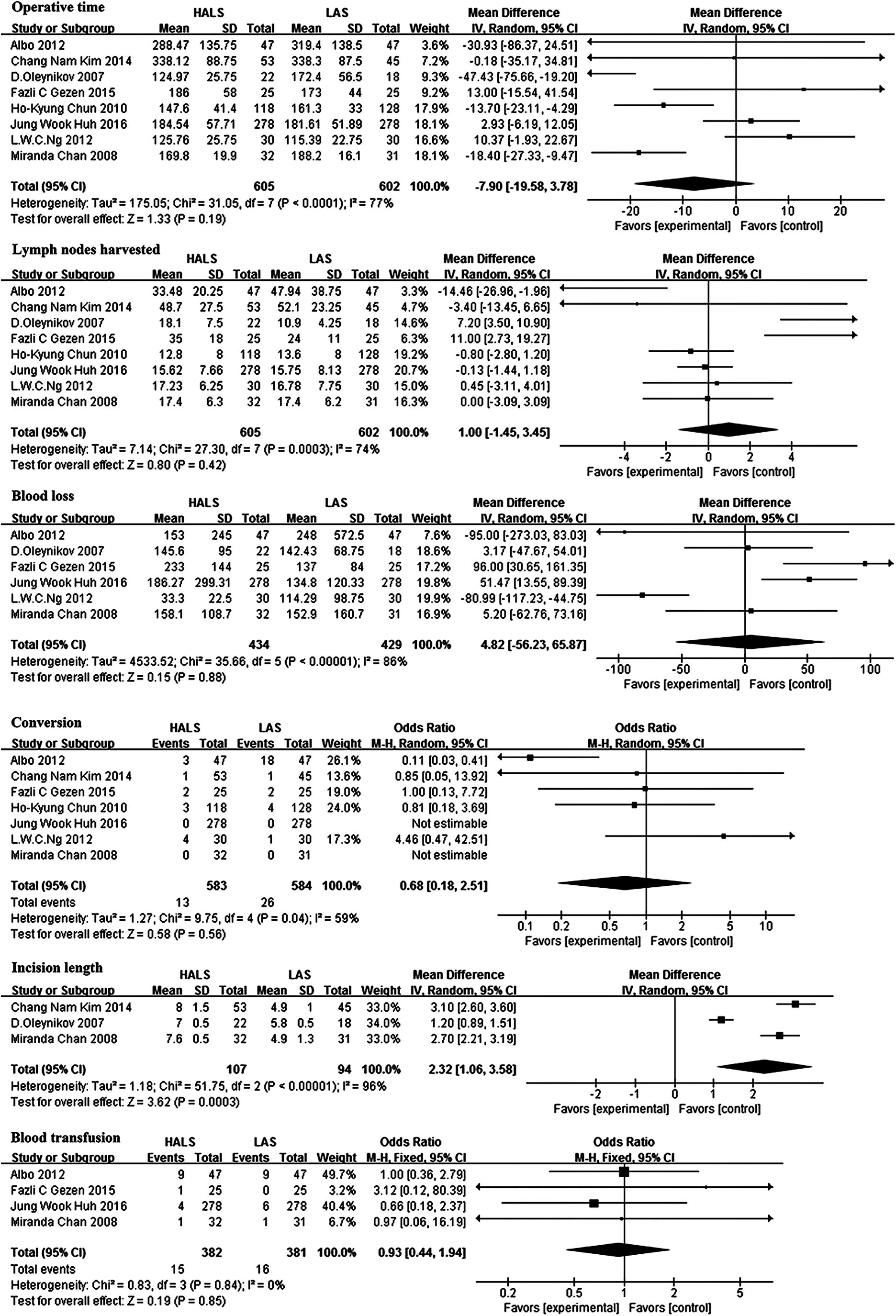
Meta-analysis of intraoperative outcomes. CI, confidence interval; HALS, hand-assisted laparoscopic surgery; IV, inverse-variance; LAS, conventional laparoscopic surgery; M-H, Mantel-Haenszel; SD, standard deviation.
Meta-analysis of postoperative outcomes
The meta-analysis demonstrated no significant differences in terms of length of hospital stay (P = .80, WMD = −0.11, 95% CI [−0.96 to 0.73], I2 = 82%), reoperation (P = .60, OR = 1.32, 95% CI [0.47 to 3.73]), time to first flatus (P = .87, WMD = 0.10, 95% CI [−1.10 to −1.29], I2 = 91%), time to first bowel movement (P = .15, WMD = −0.12, 95% CI [−0.28 to 0.04], I2 = 68%), postoperative complication (P = .24, OR = 1.31, 95% CI [0.83 to 2.07], I2 = 0%), readmission (P = .78, OR = 1.13, 95% CI [0.49 to 2.60], I2 = 0%, I2 = 25%), or mortality (not applicable). In addition, we observed no differences for complications particularly associated with surgery, including ileus (P = .20, OR = 1.60, 95% CI [0.78 to 3.26], I2 = 0%), postoperative bleeding (P = .39, OR = 1.64, 95% CI [0.53 to 5.06], I2 = 0%), anastomotic leakage (P = .98, OR = 0.98, 95% CI [0.54 to 1.81], I2 = 0%), wound infection (P = .09, OR = 1.63, 95% CI [0.92 to 2.89], I2 = 0%), intra-abdominal abscess (P = .76, OR = 0.83, 95% CI [0.25 to 2.75], I2 = 20%), urinary complication (P = .77, OR = 1.09, 95% CI [0.61 to 1.96], I2 = 0%), or cardiopulmonary complication (P = .11, OR = 0.44, 95% CI [0.16 to 1.19], I2 = 0%) (Fig. 3).
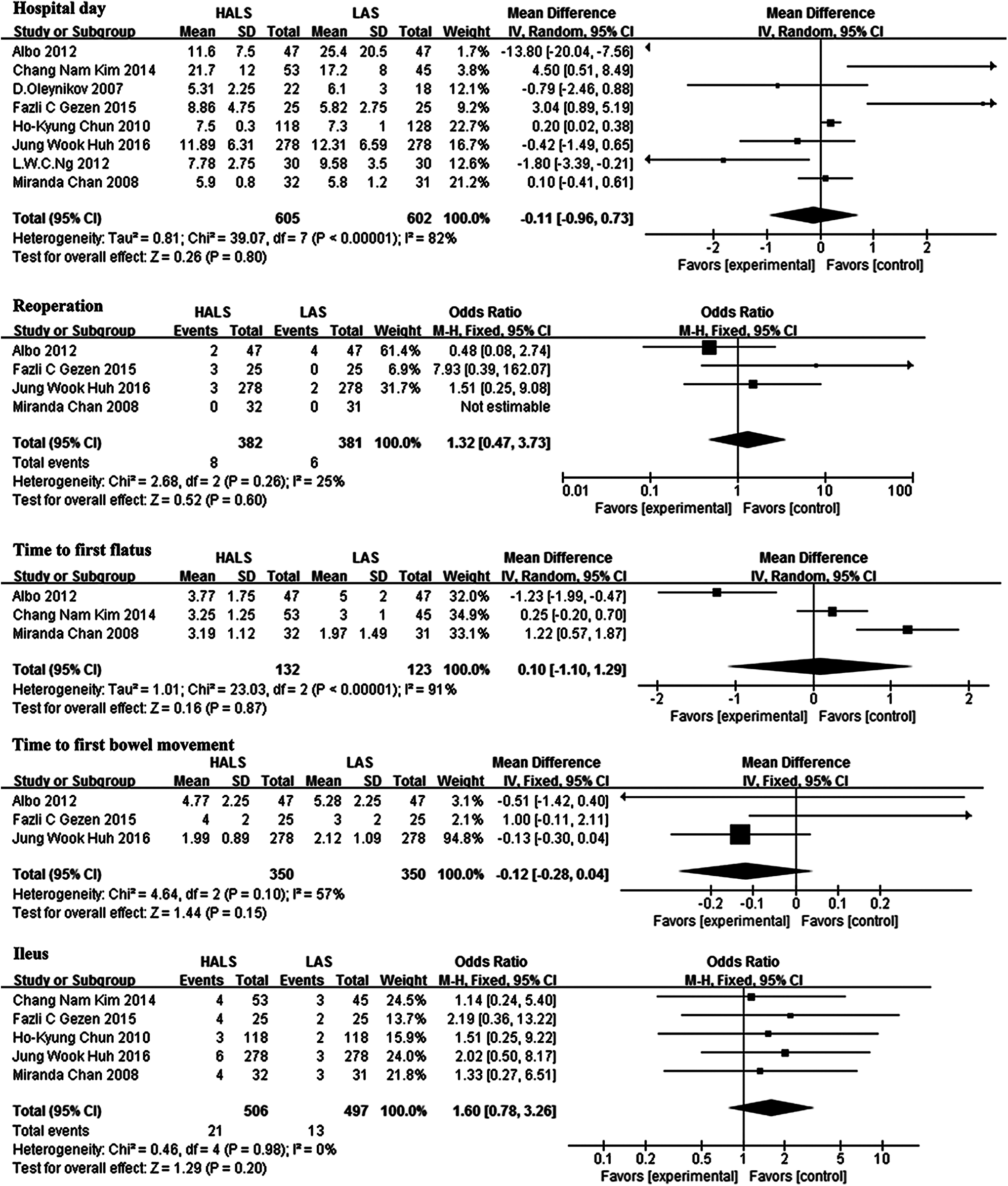
Meta-analysis of postoperative outcomes. CI, confidence interval; HALS, hand-assisted laparoscopic surgery; IV, inverse-variance; LAS, conventional laparoscopic surgery; M-H, Mantel-Haenszel; SD, standard deviation.
Meta-analysis of survival outcomes
The results showed that there were no significant differences on 5-year disease-free survival (P = .77, hazard ratio [HR] = 0.95, 95% CI [0.66 to 1.36], I2 = 0%) and overall survival (P = .81, HR = 1.10, 95% CI [0.50 to 2.39], I2 = 0%) (Table 4).
CI, confidence interval; DFS, disease-free survival; HALS, hand-assisted laparoscopic surgery; HR, hazard ratio; LAS, laparoscopic surgery; OS, overall survival.
Subgroup analysis of HALS and LAS for colon cancer and rectal cancer
We conducted subgroup analysis to compare the result of HALS and LAS for patients with colon cancer. Four studies were enrolled (223 HALS and 221 LAS). We observed that HALS group had a longer length of incision (P = .02, WMD = 2.14, 95% CI [0.28 to 4.00], I2 = 98%) (Table 5). Besides, we also designed a subgroup analysis to compare the results of HALS and LAS for patients with rectal cancer. Three studies were enrolled (310 HALS and 309 LAS), and no significant differences were observed (Table 6).
OR.
WMD.
Bold values signify when P value <.05.
CI, confidence interval; HALS, hand-assisted laparoscopic surgery; LAS, laparoscopic surgery; LN, lymph node; OR, odds ratio; WMD, weighted mean difference.
OR.
WMD.
CI, confidence interval; HALS, hand-assisted laparoscopic surgery; LAS, laparoscopic surgery; NA, not applicable; OR, odds ratio; WMD, weighted mean difference.
Publication bias
A funnel plot of the studies reporting on wound infection shows that there was no obvious publication bias among the studies (Fig. 4).
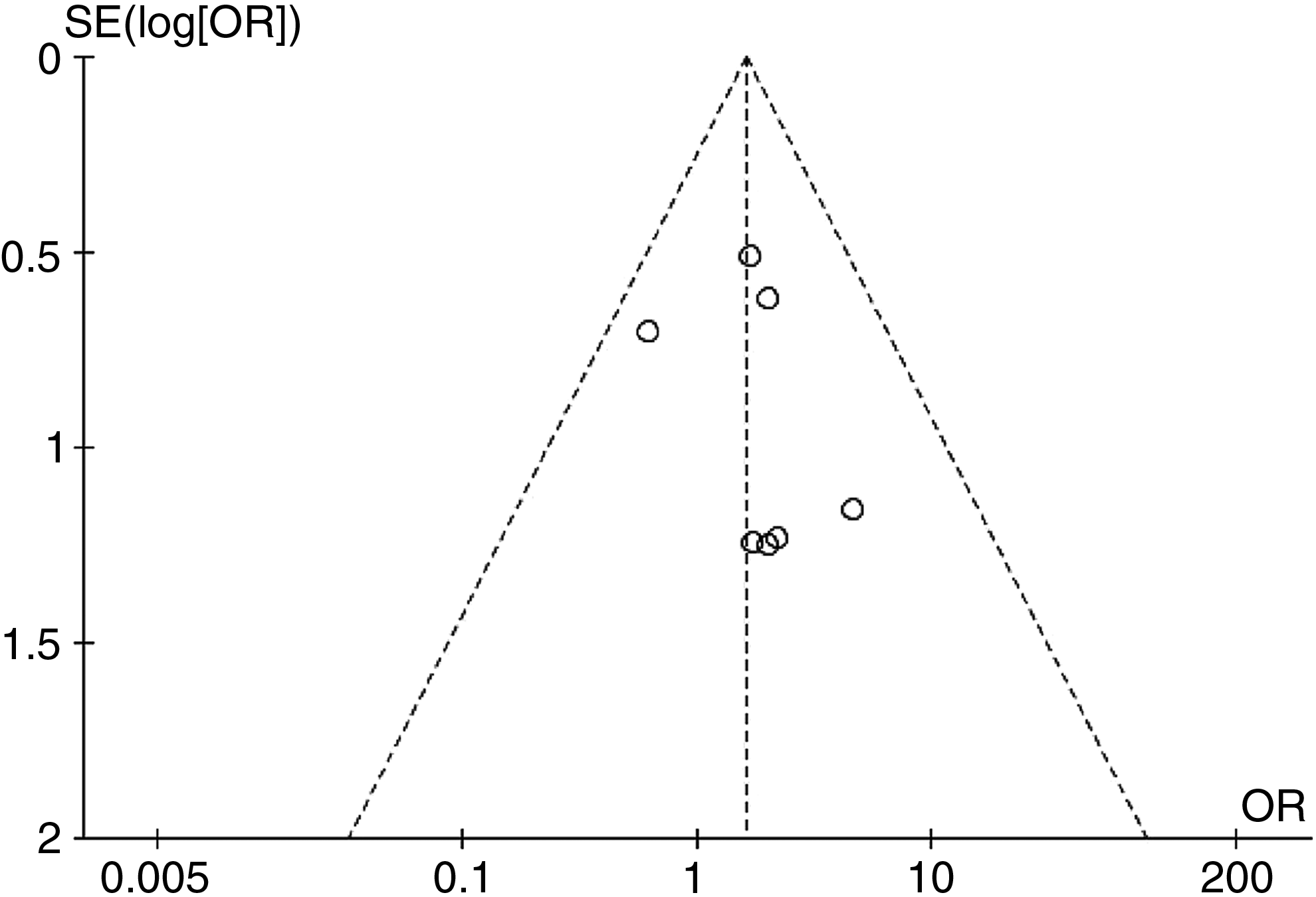
Funnel plots of the studies reporting on wound infection. SE, standard error; OR, odds ratio.
Discussion
Since the first report of hand-assisted laparoscopic technique for colorectal surgery, a large number of studies have been conducted to compare the benefits of HALS and LAS, including short-term and long-term outcomes.14,18,20,34 However, this is still a controversial issue especially for CRC because different studies may have different outcomes. 13 So it is difficult to tell which of those two surgical techniques is better. Thus, we performed this meta-analysis to compare HALS with LAS for CRC.
In our meta-analysis, we included nine studies with 1307 patients; HALS group showed a significant longer length of incision, which is controversial in previous reviews. 35 The possible reason is that a 7- to 8-cm incision is needed for hand-access device and specimen extraction in HALS. 35 This incision is generally longer compared with LAS although the length of incision may also depend on the size of surgeon's hand and location of specimen extraction. 36
As for operative time, it is generally thought that HALS should have a shorter operative time with the help of hand-access device.17,37 However, our results suggested that there was no significant difference between the two groups. Our explanation is that both groups need to create an additional incision for specimen extraction although that is at the beginning part of HALS and final part of LAS. Surgeon's learning curve and experience also play an important role in the surgery. 17 Besides, the condition of abdominal adhesions should be taken into account and our result revealed that there was no significant difference in PAS (P = .06). Additional advantages of HALS in operative time may be more obvious for bulky and complex tumors which are just very few parts in this meta-analysis.13,18 Thus, the total operative time had no difference between two groups.
Although HALS has a superior intra-abdominal visualization and exposure which may reduce the risk of vascular injury, we found no significant difference of blood loss between two groups. This result is in line with the previous meta-analysis and review.35,38 This may account for the wide use of electric surgical instruments such as monopolar electrotome, ultrasonic scalpel, and so on. Besides, surgeon's experience also plays an important role in this part.
Interestingly, different from previously published meta-analysis, 38 no significant difference was observed on conversion rate although HALS has better visualization and more flexibility for dissection. According to previous studies, the most common reason for conversion was unsatisfactory pneumoperitoneum.13,14,20,34 We think that several factors can contribute to conversion rate, including PAS, 13 BMI, 39 complex pelvic masses, and surgeon's experience. In our meta-analysis, most patients had no PAS, and most BMI were in the normal range. Besides, most tumor stages were before stage III although we didn't compare tumor size. There was no significant difference in PAS, BMI, tumor stage, and surgical procedure between the two groups. Thus, the total conversion rate had no difference between two groups. This may be also associated with surgeon's experience although we couldn't get surgeon's learning curve in this meta-analysis.
Particularly, our results revealed no significant difference in time to first flatus or bowel movement between two groups. The possible reason may be that both surgeries have similar bowel mobilization. Although HALS had a longer length of incision, there existed no significantly more incisional problem in HALS group. The rational explanation may be that the hand port device has the effect of wound protection 13 and the high nursing level also contributes to this result.
In addition, in line with previous meta-analysis and review,35,38 our results demonstrated that there was no difference in other intraoperative or postoperative complications, including reoperation rate, transfusion, ileus, postoperative bleeding, anastomotic leakage, wound infection, intra-abdominal abscess, urinary complication, cardiopulmonary complication, mortality, and readmission. Our explanation is that the two techniques are minimally invasive, and the nursing level is high. These factors reduce the risk of complications.
When it comes to survival outcomes, we found no differences between two groups on disease-free survival or overall survival. It might be due to that both techniques obey the oncological principles, which can also account for the similar lymph node harvested in two groups. Besides, the similar surgical procedures and tumor stage in both groups may contribute to this result.
In the subgroup analysis, it also showed a significant longer length of incision in HALS group for colon cancer, while it was not compared in rectal cancer. We found no other significant difference in compared items for colon or rectal cancer.
The strength of this meta-analysis is as follows: (1) our meta-analysis included more articles and more patients than previous studies, (2) we analyzed the survival outcomes, (3) we also conducted subgroup analysis of HALS versus LAS for colon cancer and rectal cancer, and (4) our meta-analysis only included malignant diseases.
Some limitations of this study have to be highlighted. First, there existed high heterogeneity in some analyses. Second, although the sensitivity analysis was conducted by removing one study each time, the outcomes remained unchanged. We thought it might be influenced by many factors, such as the learning curve of surgeon, bowel preparation, tumor stage and size, PAS, and so on. Third, most of the enrolled articles were retrospective studies. This might induce patient selection bias although there was one randomized controlled trial.
In conclusion, our meta-analysis suggests that HALS is similar to LAS for CRC surgery in terms of intraoperative, postoperative, and survival outcomes except for a longer length of incision which is created for the hand access device.
Footnotes
Acknowledgment
This work was supported by the Science and Technology Support Program of the Science and Technology Department of Sichuan Province (Grant No. 2016SZ0043).
Disclosure Statement
No competing financial interests exist.