
Abstract
Abstract
Purpose:
The aims of this review are to determine the feasibility of near-infrared fluorescence (NIRF) angiography in anastomotic colorectal surgery and to determine the effectiveness of the technique in improving imaging and quantification of vascularization, thereby aiding in decision making as to where to establish the anastomosis.
Methods:
A systematic literature search of PubMed and EMBASE was conducted. Searching through the reference lists of selected articles identified additional studies. All English language articles presenting original patient data regarding intraoperative NIRF angiography were included without restriction of type of study, except for case reports, technical notes, and video vignettes. The intervention consisted of intraoperative NIRF angiography during anastomotic colorectal surgery to assess perfusion of the colon, sigmoid, and/or rectum. Primary outcome parameters included ease of use, added surgical time, complications related to the technique, and costs. Other relevant outcomes were whether this technique changed intraoperative decision making, whether effort was taken by the authors to quantify the signal and the incidence of postoperative complications.
Results:
Ten studies were included. Eight of these studies make a statement about the ease of use. In none of the studies complications due to the use of the technique occurred. The technique changed the resection margin in 10.8% of all NIRF cases. The anastomotic leak rate was 3.5% in the NIRF group and 7.4% in the group with conventional imaging. Two of the included studies used an objective quantification of the fluorescence signal and perfusion, using ROIs (Hamamatsu Photonics) and IC-Calc® respectively.
Conclusions:
Although the feasibility of the technique seems to be agreed on by all current research, large clinical trials are mandatory to further evaluate the added value of the technique.
Introduction
A
It is thought that a better vascularization of the anastomosis will cause less anastomotic leaks.13–16 There is a large variability of the colonic vascular anatomy and many patients suffer from arteriosclerotic disease of the mesenteric vasculature. 17 Therefore, an easy and reliable method to assess the vascularization is desirable. With near-infrared fluorescence (NIRF) imaging it is expected that real-time visualization of the vasculature can be improved and, ultimately, anastomotic leaks reduced. The use of fluorescence angiography was first described in 1976 for choroid angiography 18 and is common practice in ophthalmology. Applying the technique intraoperatively during colorectal surgery is comparable to this first application; by intravenous administration of the dye and its intravascular transportation, the vessels in the target region can be seen by illumination of the fluorescent dye.
Indocyanine green (ICG) is the most frequently used NIRF dye in humans. ICG is a sterile tricarbocyanine dye composed of N-hydro-3,3,3′,3-tetramethyl-1,1-di(4-sulfobutyl)-4,5,4′4′5-dibenzoindotricarbocyanine hydroxide sodium, and absorbs light between 790 and 805 nm and re-emits light with an excitation wavelength of 835 nm.19,20 Since a better vascularization of the bowel anastomosis is thought to result in less anastomotic leakage, identifying the degree of vascularization through fluorescence angiography might help reduce the risk of anastomotic leakage.
The first objective of the review was to determine the feasibility of NIRF angiography in anastomotic colorectal surgery, with emphasis on ease of use, added surgical time and complications related to the technique. A second objective was to determine the effectiveness of the technique in improving imaging of vascularization, thereby aiding in the decision making of where to make the anastomosis. Attention was given whether the signal was quantified or validated in an objective manner or only subjectively assessed.
Materials and Methods
This study was registered in PROSPERO under the number: CRD42015025514 (www.crd.york.ac.uk/PROSPERO/display_record.asp?ID=CRD42015025514).
Search strategy
A systematic literature search was performed in PubMed and EMBASE. The following search strategy was followed: (“Indocyanine Green” [Mesh] OR Indocyanine Green OR Infracyanine Green OR ICG OR “Fluorescent Dyes” [Mesh] OR Fluorescent Dyes OR Near-Infrared Fluorescence OR Fluorescent imaging OR Fluorescence imaging OR Near Infrared Imaging) AND (“Laparoscopy” [Mesh] OR Laparoscopy OR laparoscopic OR Robotic surgery) AND (“Anastomosis, Surgical” [Mesh] OR Bowel anastomosis OR Anastomotic bowel surgery OR “Colorectal Surgery” [Mesh] OR Colorectal Surgery).
First, titles and abstracts were screened. In case of uncertainty, full text reports were read to assess eligibility. To complete the search, references within selected articles were searched as well. The search was performed by 2 independent reviewers (J.v.d.B. and M.A.T.) who selected potentially relevant articles by title and abstract.
Inclusion and exclusion criteria
Articles had to be written in English. The aim of the literature search was to identify articles that reported on the use of intraoperative NIRF angiography during colorectal anastomotic surgery. The NIRF angiography had to be used to assess the perfusion of the exterior surface of the bowel. Studies were found eligible for inclusion when the participants were adults, aged above 17 years, in whom open, laparoscopic or robotic anastomotic bowel surgery was performed for either benign or malignant disease. The intervention had to consist of fluorescence angiography during the anastomotic bowel surgery. If a control group was present, anastomotic bowel surgery should have been performed without the use of fluorescence imaging, also for either benign or malignant disease. Studies only describing other applications of fluorescence imaging were excluded. Conference abstracts, animal studies, case reports, technical notes, and video vignettes were not included. Studies not presenting original patient data were excluded as well.
Methodological quality appraisal
The Methodological Index for Non-Randomized Studies (MINORS) was used to assess the methodological quality of the included articles. 21 This validated quality assessment system is based on 8 items for noncomparative studies and 12 for studies with a control group.
Data extraction
All the studies were analyzed by 2 independent reviewers (J.v.d.B. and M.A.T.). A standard form to extract the following data was used addressing the characteristics of the study (design, allocation concealment, blinding, method of randomization, withdrawals, or dropouts), participants (age, sex, baseline characteristics, indication for surgery), intervention (type of fluorescent dye, used dose, timing of administration during surgery, used fluorescence system), and the outcomes (influence on duration of surgery, type of outcome measuring, quantification of the signal, complications intra- and postoperatively).
Data from all included trials were extracted and presented in the appropriate paragraph. Baseline data are summarized as mean or proportion for continuous and categorical variables, respectively. Outcome variables are reported as absolute number and percentage stratified by intervention, for all studies combined and separately for only those studies with a control group. Differences in the proportion of anastomotic leaks between NIRF and control using all studies, and using only studies with a control group, were computed using a two-sample test for proportions.
Results
The search was performed by 2 independent researchers and resulted in the inclusion of 10 articles. The search of PubMed (Medline) and EMBASE resulted in 111 citations. Checking reference lists of the selected articles identified seven additional studies. After adjusting for duplicates, 60 remained. Of these, 46 were discarded after reviewing the abstracts. The full text of the remaining 14 articles was examined in more detail. It appeared that 10 of these met the inclusion criteria. Four of these contained a comparison-group and were used for further quantitative analysis. The flowchart of the performed search and inclusion are depicted in Figure 1. In total, the outcomes of 1328 patients were described: 894 operated with the use of NIRF imaging and 434 patients with conventional imaging.22–31 The study characteristics of the included studies can be found in Table 1.
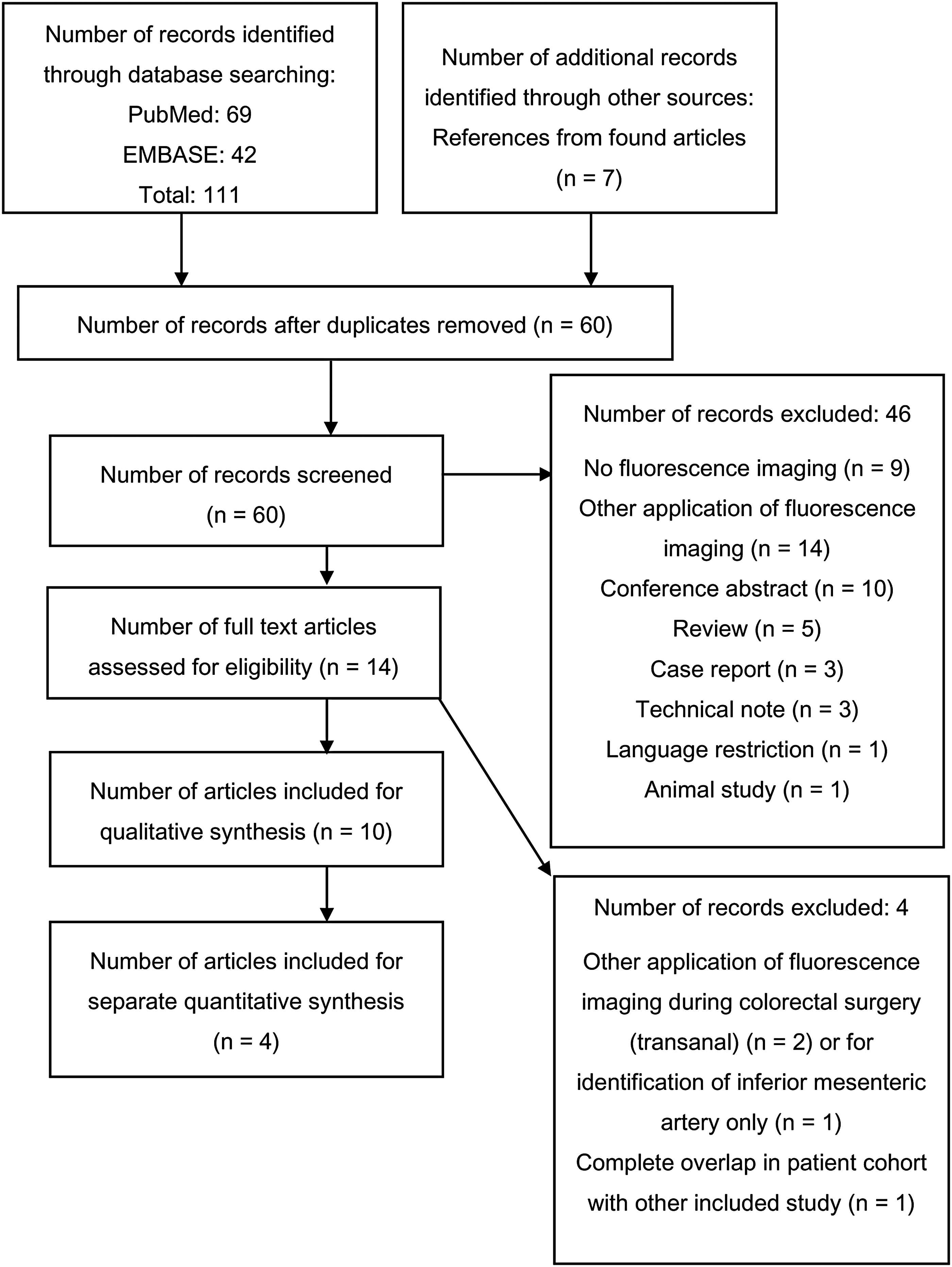
Flowchart of the performed search and inclusion.
Age expressed as mean ± SD unless otherwise indicated.
IBD, inflammatory bowel disease; ICG, indocyanine green; NIRF, near-infrared fluorescence; SD, standard deviation.
Methodological quality of studies
Since all of the included studies were nonrandomized, the risk of bias in the studies was evaluated with the MINORS methodological index. 21 For studies without a control group, the maximum possible score was 16, and 24 for the studies with a control group. The overall quality score for the assessed studies ranged between 9 and 14 (mean 10.1) for the noncomparative studies and between 12 and 20 (mean 16) for the studies with a control group (Table 2). All studies clearly stated the aim and had endpoints appropriate to this aim. Five of the studies were prospective feasibility studies, two retrospective feasibility studies, and four were retrospective matched pairs studies. The retrospective nature of most of the included studies caused an inability to control for unmeasured potential confounders between the two groups. Only three studies described loss to follow-up; the period of follow-up was unclear in most of the studies. None of the studies performed a prospective calculation of the study size. The sample size of all studies was inadequate to detect 1%–2% differences in anastomotic leakage rates at 80% power. 27 Since from Boni et al.23,25,26 and Jafari et al.24,30 more than one article is included in this review, it was checked by the authors whether those articles were based on different patient cohorts. The authors confirmed there is no cohort overlap.
Items are scored 0 (not reported), 1 (reported but inadequate) or 2 (reported and adequate). The maximum score being 16 for noncomparative studies and 24 for comparative studies.
Baseline characteristics of patients
The baseline data (number of patients, mean age, gender, and body mass index) are given in Tables 3 and 4.
Wada et al. 22 and Ris et al. 28 are not included in this number as mean ages are not mentioned. Instead, they give ages as a median of 67 and 64 respectively.
The studies of Boni et al. 25 and Wada et al. 22 and are not included in this figure. Boni et al. described no BMI in the article; Wada gives BMI as median 22.8 (range 15.8–3.43 kg/m2).
BMI, body mass index; NIRF, near-infrared fluorescence.
Kusdzus et al. described no ASA classification, smoking, and preoperative chemotherapy; these patients are therefore not included in the overview of these parameters.
Boni et al. described no ASA classification in their baseline characteristics; these are not included in the overview of this parameter.
ASA, American Society of Anesthesiologists score; BMI, body mass index; IBD, inflammatory bowel disease; NIRF, near-infrared fluorescence.
Feasibility of the technique
Factors contributing to the feasibility of the technique are considered to be the ability to obtain a signal illustrating perfusion, ease of use, complications due to the technique, and added surgical time. Eight of the 10 included studies make a statement on the feasibility of the technique and the ease of use22–29 ; NIRF imaging of colorectal anastomosis is considered “feasible” and “readily achievable.” Four of these studies illustrate this by giving the number of patients in which images that demonstrate the perfusion were successfully obtained. Jafari et al. 24 acquired NIRF images in 98.5% of the patients. The imaging was not successful in 2 patients due to equipment malfunction. Boni et al.25,26 obtain real-time images demonstrating the perfusion in all patients in both studies, as did Wada et al. 22 In the study by Ris et al. 28 the system failed to detect any visible fluorescence in 1 patient.
Complications related to the technique
In none of the articles complications attributable to the use of ICG were observed.
Added surgical time
The added surgical time is given in five articles.23,28–31 A mean added time of 4.5 minutes to the total duration of the surgical procedure is described. Ris et al. 28 noted that a shorter additional imaging time is accompanied by experience in the use of this technique. Jafari et al. 30 described a mean operation time of 4.75 h in NIRF group, compared with 4.4 h in control group. Boni et al. 23 report a 7-minute shorter mean operative time when using NIRF.
Costs
No comments about the additional costs of using the technique where made in the included articles22,23,25,27–30 except for Jafari et al. 24 who described a cost of $167,500–223,750 for the Pinpoint™ system, which resulted in cost per case of $999–1099. Boni et al. 26 state the technique seems to be cost effective. However, no cost evaluation to support this is given in the article.
Quantification or validation of the fluorescence signal and perfusion
Only Wada et al. 22 and Kudszus et al. 31 performed an objective quantification of the fluorescence signal. One of the aims of the study by Wada et al. 22 was to evaluate whether quantitative assessment of intestinal perfusion by measuring ICG signal intensity could predict postoperative outcomes such as anastomotic leakage and bowel movement recovery. For these quantitative measurements analyzing software ROIs (Hamamatsu Photonics) was used to assess the pixel intensity. A time curve of this fluorescence intensity was made and fluorescence difference between maximum and baseline was measured, as were time from first fluorescence to maximum signal, time from first fluorescence to half of the maximum signal, and the slope of this graph. For the regions of interest at the transection line, the midpoint between the mesenteric and antimesenteric sites was chosen. The maximum fluorescence intensity turned out to be lower in the 5 patients with anastomotic leakage in this study, compared to the patients in which no anastomotic leakage occurred.
Also, Kudszus et al. 31 used an objective quantification of the fluorescence signal and perfusion. For this, IC-Calc® software was used. With this software, the perfusion index is calculated (i.e., the perfusion between different sites) and curves are plotted. 32 The authors show the curves but unfortunately no cutoff value of fluorescence intensity for adequate perfusion is calculated or given, neither is the fluorescence intensity linked to the risk for anastomotic leakage. All other included studies only use a subjective assessment of the fluorescence signal. The surgeons opinion is used,23,25,27,29,30 or that of the whole surgical team (main surgeon, main assistant, fellow in minimally invasive surgery, and the assisting resident) 26 to assess whether the fluorescent signal was enough to maintain the planned resection point. In these studies, no grading was used other than “adequate/sufficient” or “inadequate/insufficient.” Jafari et al. 24 and Ris et al. 28 divided the subjective assessment in three categories, namely “optimal, adequate, or inadequate” and “good, average, and bad” respectively. Neither study describes when a revision of the surgical plan will take place based on this classification. Moreover, Ris et al. 28 graded the quality of perfusion in all patients as “Good,” while Jafari et al. 24 doesn't report the results of this grading.
Added value of the technique
The outcomes regarding perioperative decision making for all studies are summarized in Table 5, for the studies with a control group separately in Table 6.
P value: .002.
NIRF, near-infrared fluorescence.
P value: .123.
NIRF, near-infrared fluorescence.
Influence of NIRF angiography on intraoperative decision making
In total, surgical plan was changed in 97 (10.8%) cases after NIRF, of which in 90 the proximal resection margin was initially considered insufficient with NIRF. In this group, anastomotic leakage occurred in 8 patients (8.9%), compared to 23 anastomotic leakages (2.8%) in the NIRF patients with initially good fluorescent signal. In 7 NIRF patients, initial clinical impression of malperfusion was not confirmed by NIRF and resection was not extended.
In the studies with a control group, the surgical plan was changed in 47 cases (10.9%) of the NIRF group and in 1 case of the control group. Of these, in 41 patients the proximal resection margin was considered insufficiently vascularized and therefore extended to well perfused tissue. In the other 6 patients, a clinical impression of malperfusion of the resection margins was not confirmed by NIRF angiography and therefore the resection was not extended.23,27,30,31 The change of plan therefore consisted of neglecting the clinical impression and instead following the NIRF imaging. In 1 of the 41 patients of the first group, two anastomotic leakages occurred. No further information about this anastomotic leakage was provided. 27 In the second group of 6 patients, no anastomotic leakage occurred.30,31
In the studies without a control group, the surgical plan was revised in 50 patients (10.8%) after NIRF imaging. In 49 of these, a revision was performed of the proximal transection site. Six of these patients (12%) developed an anastomotic leak, at days 8, 15, 17, and 40.22,29
The other patients in whom the plan was revised, a clinically malperfused anastomosis was left unchanged because the NIRF angiography revealed good perfusion. No anastomotic leakage occurred in these patients.
Anastomotic leakage and other complications
The definition of anastomotic leakage differed between the studies. Wada et al. 22 used the following definition: “Anastomotic leakage was defined as any disruption of the anastomosis that was confirmed by digital rectal examination, sigmoidoscopy, and radiographic examination (e.g., extravasion of endoluminally administered water-soluble contrast enema, abscess at the level of anastomosis and fluid/air bubbles surrounding the anastomosis). Only symptomatic AL was included.” Kin et al. 27 used a broader definition and defined an anastomotic leak as “at least one of the following criteria: 1. An anastomotic defect noted on physical examination; 2. An anastomotic defect confirmed in the operation room; 3. An anastomotic defect seen on proctoscopy; 4. Radiologic evidence of a leak consisting of either a defect in the anastomosis and an adjacent fluid collection, or stranding or the extravasion of rectal contrast into the extraluminal space; or 5. Clinical evidence of a leak such as feculent output from a pelvic drain.” The other included articles did not give a clear definition of anastomotic leakage.23–26,28–31
Tables 5 and 6 show a summary of the occurrence of anastomotic leaks. A total of 63 anastomotic leakages occurred in the 10 included studies (NIRF group n = 31; control group n = 32). This means that 3.5% (31 out of 894) of all NIRF patients and 7.4% (32 out of 434) of all control patients developed an anastomotic leakage (P-value for difference = .002). If only considering the studies with a control group, a 4.9% (21 out of 432) leakage rate in the NIRF group was found versus 7.4% (32 out of 434) in the control group (P = .123).
Other complications that occurred were inconsistently reported in the included articles. Boni et al., 25 Kin et al., 27 and Kudszus et al. 31 reported no complications other than anastomotic leakage. Ris et al. 28 described only the grade of the occurred complications (grades I–IV Clavien-Dindo classification): all seven complications were grades 1–3. In the remaining six studies detailed information was given about the complications (Table 7). Ileus, urinary retention, urinary tract infection, pulmonary complications and wound infection were the most common complications, occurring relatively more in the control group.22,24,26,29,30
Thrombosis left renal artery, pancreatic fistula, atrial fibrillation, C difficile colitis acute renal failure, peristomal hernia, obstruction at stoma and death by suicide: all occurred once, other complications where described as “other,” without further specification.
NIRF, near-infrared fluorescence.
Discussion
The aim of this study was to investigate the feasibility of the use of NIRF angiography during anastomotic bowel surgery and determining the added value of the technique. Regarding the latter, attention was paid to whether the fluorescent signal was quantified or validated in any way.
Based on the included studies, it can be concluded that the use of fluorescence angiography in anastomotic bowel surgery is feasible. No complications attributable to the use of the technique were recorded. This makes the technique easily applicable in daily practice. Only few problems were encountered in its application, as system failure occurred only in 3 patients. This may be due to the relative inexperience of the team with this novel approach. A learning curve in the use of this technique might be present. Therefore, it can be expected that such system failure will be less frequent when this technique is used more often. It cannot be ruled out that a learning curve effect has been of influence on other observed differences between studies.
Minimal additional time is described in most articles. Jafari et al. 30 describe an average 21 minutes extra operation time in NIRF group. In these series, the decision to use NIRF angiography was at the discretion of the attending surgeon. Correspondence with the author reveals that the ICG imaging was reserved for more complex surgeries, with a longer duration for that reason. The NIRF angiography itself was thought to add maximally 10 minutes to the operation time.
Apart from safety and ease of use, the ability of the technique to change the surgical plan with positive outcome on operative results reflects the value of this technique. The overall rate of anastomotic leakages in the included studies was 4.7% (63 of 1328 patients); this percentage is comparable to what can be found in the literature.33–38 Fluorescence angiography changed the surgical plan in 10.8% of all NIRF cases. Anastomotic leakage was less prevalent in the NIRF group (3.4%) than in the control group (7.4%). This may be considered an indication of the benefit of the technique adding in improving the surgeons' ability to detect areas of poor blood supply. This consideration is supported by a pig study by Diana et al., 39 that showed that NIRF angiography allows qualitative assessment of the bowel perfusion. Yet, based on the still limited quality of the current research no solid evidence is provided to state that NIRF imaging significantly reduces the incidence of anastomotic leaks. Likewise, the studies comparing the NIRF technique with a control group of conventional imaging, still lack the strength and the evidence. Kin et al. 27 published the biggest study comparing the NIRF angiography with a control group. Their conclusion is that the benefit of NIRF angiography is equivocal. However, in this study only the proximal bowel was assessed and the perfusion of the rectal stump was not evaluated. This could explain the absence of difference between the two groups, as a malperfusion of the rectal stump may have been missed, leaving the potential advantage of the NIRF technique underestimated. This is also identified as a limitation by the authors. The same technique was used by Wada et al. 22 and Boni et al. 26
An anastomotic leak rate of 8.9% was found after revision of the surgical plan, compared to 2.8% in the patients with initial good fluorescence signal. This could mean that a good fluorescence signal is predicting a good outcome, while a lesser fluorescent signal could mean a higher risk of anastomotic leakage, whether or not the transection line is moved.
In this review, attention was given to whether the signal was quantified or validated in an objective manner or only subjectively assessed. Unfortunately, in only two studies this was attempted. As described, Kudszus et al. 31 used an objective measurement using IC-Calc. Although this method is validated in rabbits, 32 in their present study, no cutoff value was given on which revision of the resection margin was based. Wada et al. 22 used other software, namely “ROIs” (Hamamatsu Photonics K.K.) to measure the fluorescence intensity. In this study, four parameters were measured, namely difference in fluorescence between maximum signal and baseline, time from first fluorescence to maximum signal, time from first fluorescence to half of maximum signal, and the slope; fluorescence difference divided by the time until maximum fluorescence. A lower maximum fluorescence signal was observed in the patients who developed anastomotic leakage compared to the other patients. Also, a less steep slope appeared predictive for anastomotic leakage. The time until maximum fluorescence and time to half of maximum fluorescence appeared not to be predictive for anastomotic leakage.
In the other studies, the signal was subjectively assessed by the surgeon or his team. The assessment was mostly binary: considered sufficiently or not.23,25–27,29,30 Jafari et al. 24 and Ris et al. 28 divided the subjective assessment in three categories, namely “optimal, adequate, or inadequate” and “good, average, and bad” respectively. However, no specific relation of the three categories on peroperative decision making and outcome was described in their articles.
Another possible method to objectively assess the NIRF signal is ad hoc imaging software (VR-render) as described by Diana et al. 40 This software constructs a cartography of the perfused area based on the fluorescence time-to-peak and makes a real-time overlay of this cartography on the laparoscopic image. This technique has not yet been used in humans, but was validated in an animal study by Diana et al. 40 Other methods described in literature are the postoperative measurement of the Target to Background Ratio using the fluorescence intensity using OsiriX (Pixmeo, Geneva, Switzerland) 41 ; and the Signal to Noise ratio using ImageJ software (National Institutes of Health, Washington, DC). 42 Unfortunately, these techniques are used for postoperative measurement and not applicable yet in the intraoperative setting. Further studies should focus on this validation. It may be expected that this will lead to more accurate recognition of imperfect perfusion levels that will contribute to the chance of anastomotic leakage and therefore to better use of the potential of the NIRF technique.
In the control group, apart from more anastomotic leakages, also other complications occurred more often (61% in the control group as compared to 32% in the intervention group). It is unclear from the included articles whether this higher complication rate is due to the higher rate of anastomotic leakage.23,30
In the present review, no statement on the cost or savings due of the technique can be given, as this is not studied in the majority of the included articles. Yet, this is an interesting result to be included in future research. The technique has the potential to reduce anastomotic leaks. A rough estimate of its cost is between $10,000 and $50,000 more per patient with an anastomotic leak as reported in current literature.8,43,44 Any extra time still spent with its application may decrease in more routine use. And further, the fluorescence imaging mode is or will soon be commercially available in frequently used endoscopic systems, eliminating the need for obtaining a separate and therefore costly extra set of equipment. This leaves only about $80 for the required ICG as extra costs. Based on the above given estimate of cost per leak, this means that in every 125–625 (10,000/80–50,000/80) patients operated with NIRF 1 anastomotic leak should be avoided for this technique to be cost effective.
This review should be viewed with consideration based on the following. First, the included studies were all of limited quality. All the included studies were nonrandomized, and the studies with a control group were retrospective case matched studies. The case matching could prevent bias by selecting comparable groups when taking all risk factors for anastomotic leakage in account. However, in the study by Jafari et al. 30 the controls were selected from cases performed in the same period and it was not described why those patients did not undergo fluorescence imaging. This particular reason could be of influence on the outcome. Boni et al., 23 Kin et al., 27 and Kudszus et al. 31 all selected cases from the period before the introduction of the NIRF technique. Although the articles discussed the lack of difference in treatment between the two periods of time, minor changes might still be present and could therefore have had an influence on the outcome. Furthermore, the retrospective nature prohibits correction for unmeasured confounders between the two groups. Another limitation is the inclusion of mostly small studies with an unclear follow-up period and lack of prospective sample size calculation. Because of the inconsistent reporting and the small number of patients no conclusions on the occurrence of complications can be made.
In summary, fluorescent imaging for assessment of bowel perfusion in colorectal resectional surgery is feasible and easy to use and based on the reports so far, holds great potential. All authors are positive about its added value over the usual clinical assessment methods. Nevertheless, data are still limited and results on quantification and validation of the signal are scarce. Further studies are needed to validate the technique and establish its contribution to the prevention of anastomotic leakage.
Footnotes
Disclosure Statement
No competing financial interests exist.