
Abstract
Abstract
Background:
To date, there are no published studies focusing on the benefits of minimally invasive esophagectomy (MIE) versus open esophagectomy at a Veterans Affairs Medical Center (VAMC). Our primary outcome was the incidence of esophageal malignancy in the veteran population and the postoperative morbidity following traditional and MIE for malignancy.
Design:
Retrospective analysis of the incidence of esophageal malignancy at a Veteran Integrated Service Network (VISN) 5 VAMC reported to the VAMC Esophageal Tumor Registry between 2003 and 2016 and outcomes of the veterans who received esophagectomy for malignancy. Patients were followed for 5 years following diagnosis of esophageal malignancy.
Results:
The Washington DC VAMC Tumor Registry recorded over 130 individuals with a new diagnosis of esophageal cancer between 2003 and 2016; 18 patients underwent an open transhiatal or Ivor Lewis esophagectomy and nine underwent an Ivor Lewis MIE. Surgical candidates had an average stage less than two (T1-3, N0-1, M0) and nonsurgical candidates had an average stage greater than three. Age, body mass index, smoking status, or renal function at time of surgery was similar between the two surgical groups. Patients who underwent an MIE had less blood loss (222 cc versus 822 cc, P < .001), fewer transfusions (11% versus 56%, P = .027), and more nodes harvested (10.33 versus 2.72, P < .001) with no change in leak rate (11% versus 17%, P = .703) or postoperative mortality (0% versus 6%, P = .490) compared to traditional esophagectomy.
Conclusions:
This report supports the migration toward MIE for malignancy and reemphasizes that veterans present with advanced disease.
Introduction
R
Due to the aggressive nature of esophageal cancer, only 20% of patients with a new diagnosis present with localized disease, with another 31% of patients harboring regional lymph node invasion. 5 Despite access to medical screening, outreach programs, and excellent follow-up, veterans are no exception and usually present with nonoperable disease. Currently, there are few articles that focus on outcomes of veterans undergoing surgical resection for esophageal cancer using MIE techniques.6–8 This article describes the treatment of veterans with esophageal cancer and reports a single institution's initial pilot study using MIE techniques.
Materials and Methods
Data acquisition
The Institutional Review Board at the Veterans Affairs Medical Center (VAMC) in Washington, DC, approved this retrospective review (#111327). The Veterans Affairs Esophageal Tumor Registry was queried for veterans with a new diagnosis of esophageal cancer treated at the Washington DC VAMC between 2003 and 2016. These results were cross-referenced with the Computerized Patient Record System (CPRS) and Veterans Information Systems and Technology Architecture (VISTA) network between 2003 and 2016 for “esophageal” and “esophagus” within the thoracic surgery specialty.
Surgical candidates underwent staging with positron emission–computed tomography (PET/CT) of the chest, abdomen, and pelvis. Preoperative staging included a preoperative endoscopic ultrasound (EUS). Lesions relegated to T1 disease without nodal involvement underwent surgery without neoadjuvant therapy. Patients with nodal disease and lesions greater than T1 underwent neoadjuvant chemotherapy and radiation consisting of five-fluorouracil, leucovorin, and oxaliplatin and 4500 cGy.
Following neoadjuvant treatment, a subsequent EUS and PET/CT was performed and all patients with resectable esophageal malignancy were separated into those who underwent traditional esophagectomy (posterolateral thoracotomy with midline or subcostal laparotomy) versus MIE ILE. Patients with metastatic esophageal cancer and patients unable to tolerate general anesthesia were excluded from surgical resection.
Statistical analysis
Clinical and pathological data were reviewed retrospectively and analysis was performed using univariate analysis and Cox regression modeling with P < .05 holding significance. IBM SPSS version 24 statistics software was used for analysis.
Surgical technique
Diagnostic laparoscopy is performed to rule out carcinomatosis or hepatic lesions. Two 5 mm ports are placed in the left anterior axillary and two 5 mm ports are placed in the right abdomen in approximately the right anterior axillary line. A final 5 mm port is placed in the subxiphoid region and replaced with a self-retaining laparoscopic liver retractor. Upper endoscopy is performed to identify the location of the cancer, unless it was previously marked with an endoscopic tattoo. The endoscopic location is correlated with the external location of the tumor. A point ∼6 cm distal to the tumor is marked with cautery or a stitch.
The gastrohepatic ligament is divided, and the right crus of the diaphragm is exposed using ultrasonic shears. The crural dissection is carried anteriorly along the phrenoesophageal ligament and toward the left side of the crural mechanism. A circumferential dissection of the esophagus is performed and extends into the mediastinum to release the esophageal attachments to the aorta and bilateral pleural spaces. Superiorly, the dissection extends to the level of the inferior pulmonary vein. The left crus is incised in a full-thickness manner utilizing the ultrasonic shears at the 2 o'clock position to widen the hiatus and prevent any compression of the gastric conduit.
The left gastric artery is divided with a laparoscopic stapler at its junction with the celiac axis. The nodal basin associated with the left gastric artery is resected en bloc with the artery. Lymph nodes in the retrocardiac region are also resected along with lymph nodes within the lesser sac. The left and right epiploic vessels are identified along the greater curve of the stomach. The greater curve of the stomach is dissected by starting ∼2 cm caudal to the right gastroepiploic artery. The dissection extends superiorly toward the angle of His. The short gastric vessels are divided, but a large swath of fat is left intact along the greater curve to ensure preservation of the gastroepiploic arcade. The dissection proceeds inferiorly toward the junction of the right gastric artery and gastroduodenal artery. The gastroduodenal artery is left intact and the dissection extends behind the stomach toward the head of the pancreas. Any associated lymph node is resected and sent as a separate specimen. The gastrocolic ligament is divided with the ultrasonic shears and the omentum and hepatic flexure are dissected in an avascular plane to expose the duodenum. The duodenum is kocherized and a pyloroplasty is performed by making a longitudinal enterotomy 1 cm proximal to the pylorus in the distal antrum. The enterotomy is extended 1 cm across the pylorus onto the duodenal bulb. Three 2-0 silk sutures are used to approximate the edges of the enterotomy in a transverse manner. A laparoscopic stapler is placed below the full-thickness sutures to close the enterotomy. The pyloroplasty is completed by securing a piece of omentum on top of the stapled pyloroplasty with 2-0 silk sutures.
The previously placed cautery or suture is identified again to clearly mark the gastric resection line. A series of laparoscopic staplers are then used to divide the stomach 1 cm distal to this mark. A second series of laparoscopic staples is placed parallel to the original staple line to obtain a 1 cm resection margin. This piece of tissue is placed in a specimen bag, extracted from the abdominal cavity, and sent for frozen section to evaluate the distal margin status. The proximal segment of the gastric conduit is secured to the distal gastric specimen using 0-silk sutures. A 2-0 silk suture is placed on the anterior body of the gastric conduit 1 cm from the staple line to ensure proper orientation of the gastric conduit.
Before closure of the abdominal cavity, a feeding jejunostomy is placed. The ligament of Treitz is identified and a point 50 cm from the ligament of Treitz is grasped. This portion of bowel is elevated to the abdominal wall at the level of the left lateral trocar and four full-length 2-0 silk sutures are utilized to secure the anti-mesenteric border of the jejunum to the abdominal wall. These four sutures are placed circumferentially around the jejunostomy site, while a fifth suture is placed distally to prevent torsion of the small intestine. Electrocautery is used to make an enterotomy and a 16-Fr feeding jejunostomy is inserted. The 12 mm port in the midline is then closed with fascial sutures and then, all ports are removed and closed with skin sutures.
The patient is then repositioned in the left lateral decubitus position. A 5 cm modified muscle sparing right thoracotomy is created at the fifth or sixth intercostal rib space. The pleural cavity is entered and the ribs are spread to facilitate instrumentation, while the anesthesiologist begins single-lung ventilation of the patient's left lung. The inferior pulmonary ligament is divided and the lung is retracted medially and cephalad. A circumferential dissection is performed around the esophagus. Periesophageal lymphatic tissue is harvested and sent to pathology as a separate specimen. The dissection extends inferiorly to the level of the hiatus. The abdominal cavity is entered from the superior aspect of the mediastinum and the specimen and gastric conduit are brought into the thoracic cavity.
Typically, the azygos vein is divided with either heavy silk ties or a laparoscopic stapler. Once the azygos vein is divided, the esophageal dissection extends superiorly to obtain at least a 10 cm margin above the tumor. A laparoscopic stapler is used to divide the proximal esophagus and a frozen section is obtained on the proximal margin.
The esophageal staple line is placed anterior to the gastric conduit and an enterotomy is made at a corner of the esophageal staple line. An enterotomy is made on the anterior aspect of gastric conduit. An incision is made overlying the seventh intercostal space to insert a laparoscopic stapler. The esophagogastrostomy is then performed with a 60 mm laparoscopic stapler. The common enterostomy is then closed in two layers. The first layer is a full-thickness running closure with 2-0 Polydioxanone Suture (PDS), and the second layer is performed with interrupted seromuscular sutures using 2-0 silk. The anastomosis is then tested with air insufflation under water. A 28-Fr straight chest tube and a 19- or 24-Fr Blake drain are secured into the right chest and the modified thoracotomy incision is closed in layers.
Results
Between 2003 and 2016, the Washington DC VAMC Esophageal Tumor Registry recorded 137 new diagnoses of esophageal cancer. This cohort was predominantly males (98%) with an average age of 67 years at the time of diagnosis. Most veterans were diagnosed with stage III (35%) and stage IV (33%) disease. Veterans with stage I (14%) and stage II (18%) disease were offered surgical resection in 44% and 36% of cases, respectively. In addition to surgical resection, patients with resectable disease underwent neoadjuvant chemotherapy and radiation in 39% and 39% of cases for stage I and 55% and 77% of cases for stage II, respectively (Table 1). Only 9% of veterans presenting with stage III disease qualified for surgical resection, and all veterans with stage IV disease were treated with chemoradiation or palliative procedures. Cox regression analysis indicated that veterans who underwent surgical resection for esophageal cancer had a higher 5-year survival (Fig. 1, 33% versus 10%, P = .002) and longer lifespan (26.2 versus 9.4 months, P = .001) compared to nonoperative treatment only (Table 1).
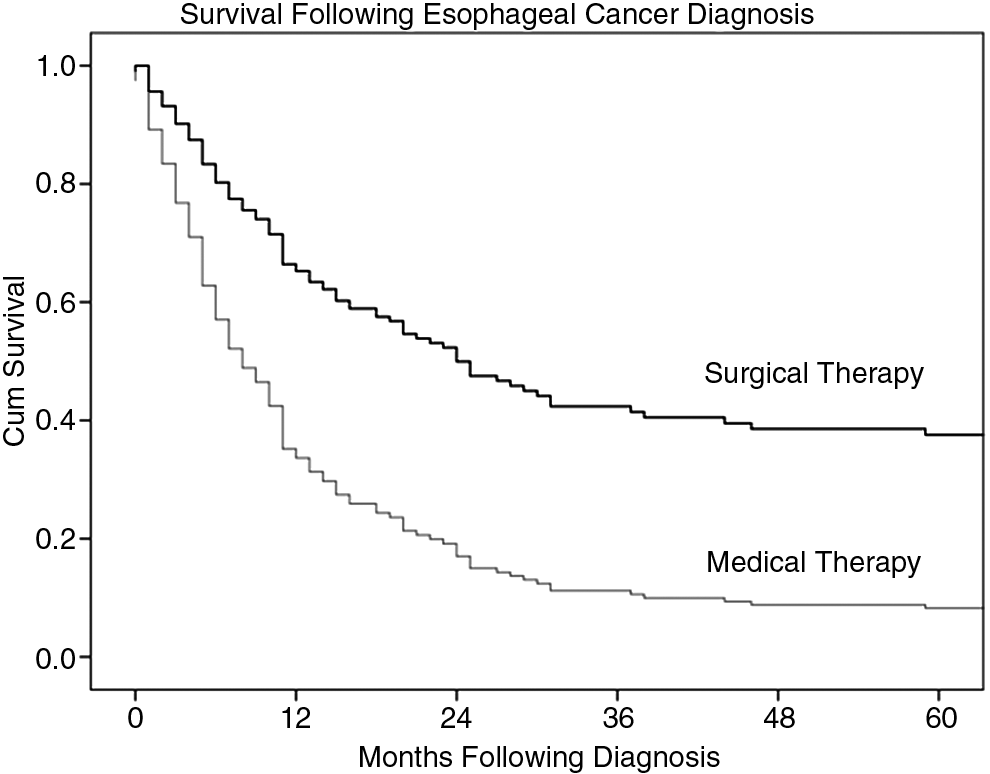
Cox regression curve of 5-year survival following diagnosis of esophageal malignancy at a VAMC between 2003 and 2016, between surgical and medical treatment arms (33% versus 10%, P = .002), respectively.
Note the profound difference in survival following diagnosis for veterans with esophageal malignancy who qualified for surgical therapy versus medical therapy.
CI, confidence interval; VAMC, Veterans Affairs Medical Center.
Cross-referencing the CPRS and VISTA network between 2003 and 2016 for “esophageal” and “esophagus” within the thoracic surgery specialty yielded 27 independent esophageal resections for malignancy. Within this cohort, 18 were performed with traditional laparotomy with or without thoracotomy (7 Ivor Lewis and 11 transhiatal) and 9 were performed with a laparoscopic dissection with or without mini-thoracotomy (8 Ivor Lewis and 1 transhiatal). Within both surgical groups, preoperative pathology obtained by EUS with biopsy identified adenocarcinoma in 67% of cases and squamous cell carcinoma in 33% of cases with one case of signet cell carcinoma in the traditional cohort. In general, patients were well matched between traditional and MIE arms (Table 2), except for preoperative serum albumin, which was higher in the MIE group (3.95 versus 3.51, P = .031). Operative time was similar for both groups; however, MIE had significantly less blood loss (222 cc versus 822 cc, P = .001) and a higher nodal yield (10.33 versus 3.72, P < .001) with a lower transfusion burden (11% versus 56%, P = .027) (Table 3). There was no statistically significant difference in postoperative length of stay, anastomotic leak rate, reoperation, or 30-day mortality, but there was a higher rate of pathologic upstaging in the MIE group (33% versus 0%, P = .016) compared to traditional esophagectomy (Table 4).
Preoperative serum albumin was statistically higher in the MIE group compared to the traditional group.
BMI, body mass index; MIE, minimally invasive esophagectomy.
Operative blood loss, transfusion requirement, and nodal harvest were improved in the MIE group compared to traditional esophagectomy.
MIE, minimally invasive esophagectomy.
Pathological upstaging following MIE was more common compared to traditional esophagectomy.
MIE, minimally invasive esophagectomy.
The patient with an anastomotic leak in the MIE group occurred within the first 24 hours and was promptly taken back to the operating room and explored. The pinpoint leak was attributed to technical error as there was no tension on the anastomosis and the blood supply was adequate. The leak was repaired with a primary closure and pleural flap buttress. This patient did not develop a stricture subsequently. Following their resection, 2 patients required a single dilatation and 1 patient developed delayed gastric emptying that resolved at 6 months. Presently, only 1 patient has an intact jejunostomy feeding tube for intermittent bolus feedings.
Three patients in the traditional esophagectomy group required reoperation for leak during the initial hospitalization. The first underwent an exploratory thoracotomy for concern of a tracheoesophageal fistula after ILE following successful CPR for an unwitnessed cardiopulmonary event. The planned thoracotomy was aborted when the patient became hemodynamically unstable in the operating room following intubation. The patient was taken back to the intensive care unit for supportive care, but expired shortly after. The cause of the initial cardiopulmonary incident was attributed to a pulmonary embolus. The second patient developed a leak at the cervical anastomosis following transhiatal esophagectomy. The cervical leak was managed with local wound management and subsequent closure, but the patient developed dysphagia to solids. Esophageal dilation was performed and was successful. The third patient developed a leak following ILE at the proximal end of the gastric conduit at the vertical staple line secondary to ischemia. The ischemic area was debrided and primary repair was performed. The existing anastomosis was interrogated and found patent. There was no additional postoperative complication following repair of the leak.
Discussion
Current literature supports hybrid or totally endoscopic MIE for esophageal malignancy in a non-Veterans Affairs academic sector. Within the veteran population, little information with regard to surgical modalities in treating esophageal cancer exists. This report expands on the diagnosis and treatment of esophageal cancer in the veteran population with a comparative analysis of hybrid MIE to traditional esophagectomy at a single VAMC.
The decision to begin with laparoscopic abdominal mobilization was based on a desire to reduce morbidity and enhance recovery from ILE. Our laparoscopic dissection incorporates every aspect of an open technique, including a pyloroplasty, kocher maneuver, and a feeding jejunostomy. The hiatal dissection extends superiorly toward the pulmonary vein under direct vision and facilitates the mediastinal dissection through a small thoracotomy. Consideration was also given to offering a transhiatal esophagectomy. The transhiatal option with a cervical anastomosis was abandoned to maximize visualization during the dissection and anastomosis and increase nodal yield. Recently published data support the decision for a hybrid ILE versus other techniques based on the fact that esophagectomy with an intrathoracic anastomosis outperformed esophagectomy with a cervical anastomosis (Orringer or McKeown) in terms of a higher nodal yield and lower anastomotic leak rates. Furthermore, the data showed fewer pulmonary events with a laparoscopic component and a mini-access thoracic approach. 9 Given our success and experience with a hybrid MIE, future efforts will focus on migrating toward a totally endoscopic esophagectomy as described by others. 10
This initial data from our VAMC reflects mirror the clinical outcomes in the non-Veterans Affairs sector and encompasses all stages of disease where surgical therapy is appropriate. Most importantly, when the hybrid MIE is performed by experienced surgeons it is less morbid than traditional esophagectomy. 6,11 Due to clinical stage, patient desires, and comorbid conditions, only 30% of veterans diagnosed with esophageal cancer were deemed surgical candidates. As a result, our study lacked the power to demonstrate statistically significant changes in 30-day mortality, leak, and reduced length of stay for the MIE versus the traditional group. Despite this, combined postoperative mortality rates between MIE and traditional esophagectomy are similar to larger studies that average 3.8%. 11 Our total postoperative leak rate was slightly higher than published data. However, since transitioning to an MIE approach, we have not encountered an anastomotic leak in the last 2 years. Our postoperative length of stay was also slightly higher than data from high-volume centers, 11 but mirrors length of stay from low- and medium-volume centers.12,13 Pathologic upstaging for the MIE group was also higher due to the improved nodal dissection along the left gastric artery and retrocardia, which is performed under magnification versus laparotomy.
The limitations of this analysis stem from the lower operative rates of esophagectomy for malignancy at a single VAMC. While some surgeons wish to centralize esophageal surgery at high-volume centers,14,15 others argue that surgeon experience, not hospital volume, is essential for decreasing early mortality.16,17 Our analysis supports the latter theory that surgeon experience, not hospital volume, is the true determining factor of patient outcomes. Overall, our postoperative mortality for the MIE group is lower than that reported by larger studies, despite being at a VAMC that would be classified as a “low-volume center.” The low morbidity is more than likely secondary to the general and thoracic surgeons who perform MIE at our VAMC. Both surgeons have performed esophagectomies as a team for over 10 years and both have ∼20 years of experience with esophagectomy for malignancy. 18
Conclusions
This report bolsters current trends in esophageal surgery and supports migration toward minimally invasive surgical options for veterans with esophageal malignancy seeking treatment at the VAMC. The results also indicate that, although the demographics within the veteran population have changed and screening measures are more standardized, veterans present with advanced esophageal cancer. Furthermore, analysis of the Veterans Affairs Esophageal Tumor Registry confirms the nefarious nature of esophageal cancer and reaffirms that veterans with resectable disease have longer survival. These facts reiterate the urgency of early diagnosis of esophageal cancer and the relationship between early diagnosis and prolonged survival. For these reasons, we hope to disseminate this information to the VA community to facilitate the institution of advanced screening programs for veterans at risk of developing esophageal malignancy. Concurrently, these programs should encourage veterans to seek treatment for early symptoms and streamline access to diagnostic testing.
Footnotes
Disclosure Statement
No competing financial interests exist.