
Abstract
Abstract
Objective:
Laparoscopy-assisted cutaneous ureterostomy (LA-CU) is a minimally invasive approach for temporary urinary diversion in children. We describe the technique, its feasibility, potential advantages, and outcomes in 12 children treated for a variety of conditions.
Methods:
Three trocars were used transperitoneally, one transumbilical, and another placed at the later stoma site. In the semilateral position, with a panoramic view, the ureter of interest is easily identified, mobilized, and exteriorized for stoma creation. We retrospectively reviewed our experience at two tertiary-care centers and included both refluxing and end ureterostomies. The study period was between October 2014 and February 2017. Renal function and growth curves were noted at follow-up.
Results:
Twelve children underwent LA-CU: 3 end and 9 refluxing ureterostomy. Mean age was 18.75 ± 17.60 months. Mean operating time was 94.44 ± 34.86 minutes. Follow-up ranged from 10 to 38 months. No major postoperative complications occurred. Renal function and growth curves improved in the majority of children.
Conclusions:
Primary surgical correction of obstructive or refluxing uropathy is the gold standard; however, temporary urinary diversion is useful in specific scenarios. In these patients, laparoscopic assistance may offer better and direct visualization, achieves accurate and rapid identification of ureter, and provides adequate mobilization, tension-free exteriorization, and excision of redundant ureter in some to optimize drainage. One trocar at the eventual stoma site minimizes scarring.
Introduction
D
The refluxing CU may be the favored option in case of impaired bladder function and because of its refluxing nature acts as a pop-off mechanism and maintains bladder cycling as opposed to a vesicostomy. 6 Refluxing ureterostomies can be a loop or divided (double-barrel) conduit. The open approach is the gold standard and the laparoscopic approach is fairly a recent development. 7 Laparoscopic assistance provides a great opportunity to simplify the procedure by easy and quick identification of the ureter, adequate or extensive mobilization of a redundant ureter if necessary along with the advantages of a minimally invasive approach. In this article we present a series of 12 children treated with unilateral refluxing or end laparoscopy-assisted CU (LA-CU) for a variety of conditions.
Patients and Methods
Between October 2014 and February 2017, retrospective case note review included a total of 12 patients who underwent LA-CU. A summary of this cohort is given in Table 1. Demographics, clinical diagnoses, indications for intervention, ureterostomy type, operating time, complications, follow-up, and outcomes such as incidence of urinary tract infection, growth, and renal function are reported.
bUTI, (breakthrough) urinary tract infection(s); GCI, growth curve improvement; HUN, hydroureteronephrosis; IKF, improvement of kidney function; LA-CU, laparoscopy-assisted cutaneous ureterostomy; NFP, need for antibiotic prophylaxis; PUV, posterior urethral valves; VUR, vesicoureteric reflux.
Technique
The stoma site is planned and marked as low as possible to facilitate easy urinary drainage into the diaper. The procedure is performed under general anesthesia with the patient lying in the lateral decubitus position. Using a transumbilical cut-down approach, a 5 mm Hasson port is placed. Pneumoperitoneum is created with a pressure of 8–10 mmHg and a flow of 2–3 L/minute. A 5 mm 30° telescope is introduced and abdominal cavity inspected and ureter identified. Two more 3 mm working ports are placed in the ipsilateral paraumbilical region and another at the expected CU site (Fig. 1). The ureter is mobilized by careful dissection of the overlying peritoneum and surrounding tissue. In duplex systems, the common ureteric sheath is opened. When adequate mobilization is performed proximally and distally, a loop of the ureter is exteriorized through the overlying port site by widening the wound including the fascial layer (Fig. 2). The stoma is then fashioned without any tension. In the case of an end ureterostomy the ureter is disconnected from the bladder, exteriorized, if needed the redundant part is excised and stoma formed (Fig. 3). The distal divided end at the bladder level is suture ligated or an endoloop is applied.
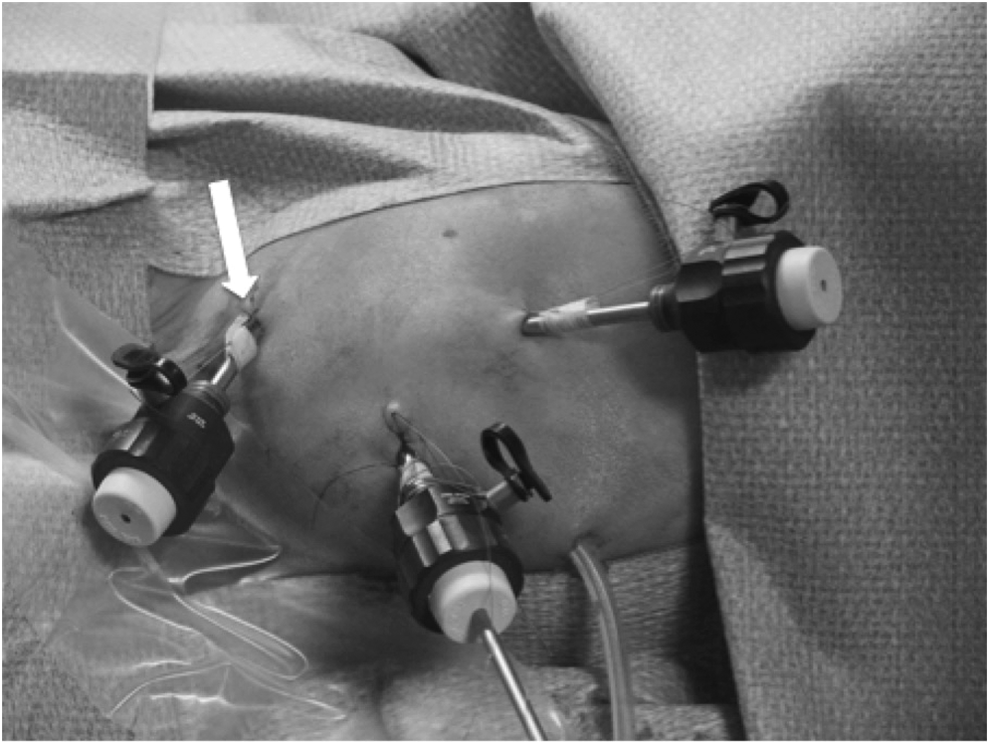
Peroperative image of Case 4: three trocars are in place. In this case the peritoneal dialysis catheter was used for carbon dioxide insufflation. The later stoma site at the iliac port is depicted with a white arrow.

Peroperative image of Case 7: after placement of a support suture in the distal part of the ureter, it can be exteriorized through the iliac port.

Peroperative image of a laparoscopy-assisted end ureterostomy with a tape measure.
Results
Between October 2014 and February 2017, we have used the laparoscopic approach to perform 12 ureterostomies: 3 end and 9 refluxing CUs. There were no intraoperative complications. Mean age was 18.75 ± 17.60 months (range: 24 days to 4 years and 6 months) and mean operating time was 94.44 ± 34.86 minutes (range: 60–180 minutes). Case 12 showed extended operating time (180 minutes) because of various difficulties: extensive inflammation, pus, and a duplex system with both ureters of the upper and lower moiety lying in a common inflamed sheet.
There were no major postoperative complications, except for transient peristomal excoriation in one (Case 5) and the need for temporary catheterization of the stoma because of edema in another. The excoriation resolved after minimal dermatological management. All patients were discharged by 48 hours and all parents were trained for stoma care. Urinary infections did not recur except for 2 and growth curves improved in all 12 cases (Fig. 4). Renal function also improved with a mean preoperative creatinine level of 1.09 ± 0.90 mg/dL (range: 0.23–2.57), and postoperative level of 0.71 ± 0.53 mg/dL (range: 0.21–1.66). Follow-up ranged from 10 to 38 months.
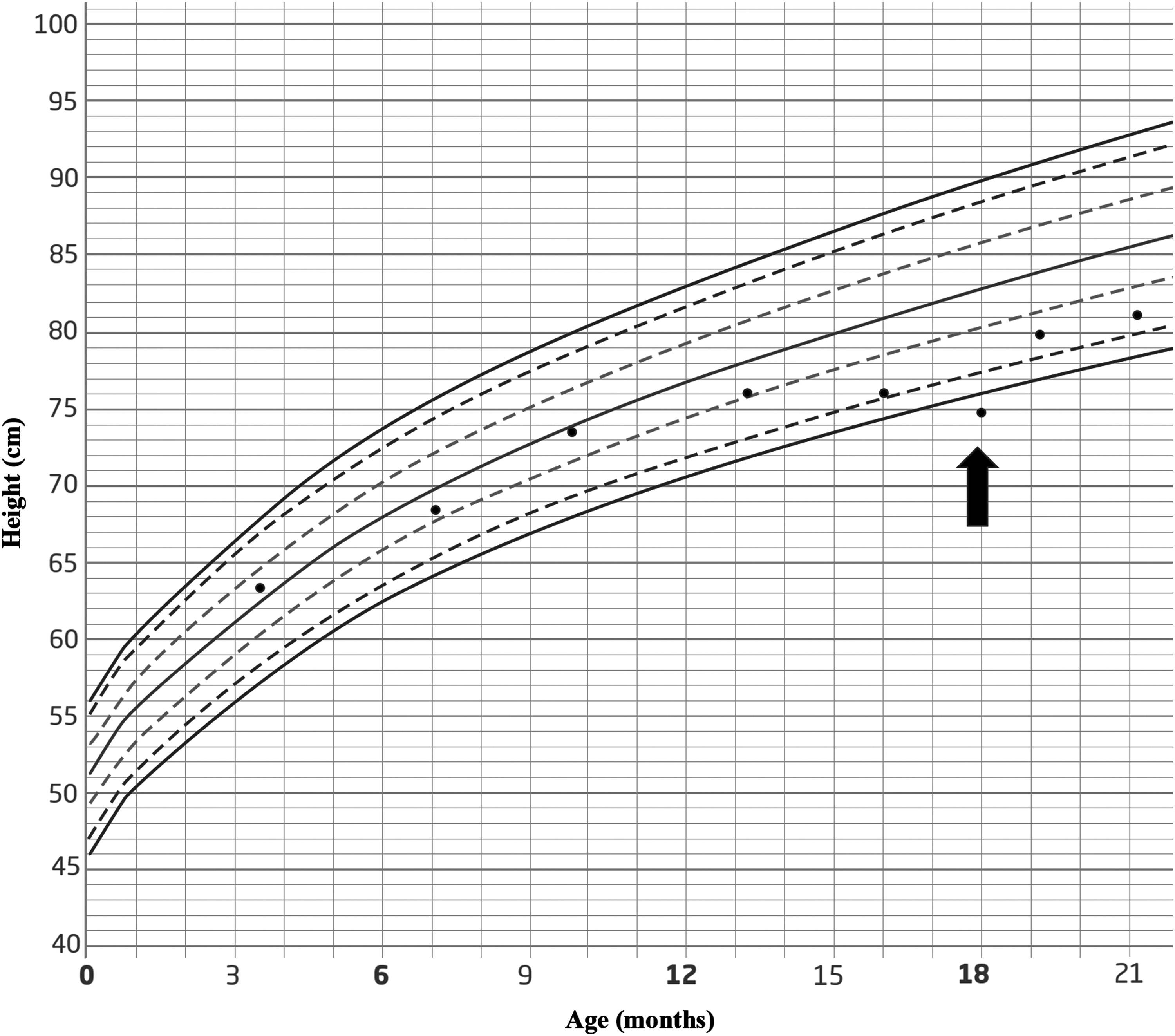
Growth curve of Case 6 showing important augmentation of the curve immediately after urinary diversion. The time of operation is pointed out by the black arrow.
Discussion
Temporary urinary diversion in children with obstructive or refluxing uropathy is an uncommon necessity in current practice. The preferred approach is primary surgical reimplantation or correction of the underlying pathology.2,8–10 In some, primary reconstruction or corrective surgery needs to be delayed in certain clinical scenarios such as in the very young with deteriorating renal function or breakthrough urinary infections.1–3 The open approach is well established and the gold standard. In the open approach a 2 cm incision is made, just above the inguinal ligament. The retroperitoneal space is reached by use of the muscle-splitting technique. Bowel structures with overlying intact peritoneum are retracted medially, so the ureter of interest can be found laterally. This surgical step can be difficult in the case of a dilated ureter resembling adjoining structures like for instance the bowel, or in the case of a deflated ureter for example after placement of a nephrostomy. Often, the incision has to be widened, if the ureter of interest is not directly in view. After identification and mobilization, the ureter needs to be brought to the surface with minimal tension. This may not be easy to achieve because of limited overview through the small incision. On the contrary laparoscopic assistance may offer several advantages.7,11,12 First, as mentioned before, it can be challenging to identify the ureter through a small inguinal incision. Better visualization can simplify this surgical step. Better overview also improves adequate ureteric mobilization and tension-free exteriorization, facilitates the excision of redundant ureter in some cases to optimize drainage, and decreases the size of incision needed at the stoma site. By preoperative localization of the eventual stoma site, it is possible to simply place one of the trocar incisions at the same point. This facilitates exteriorization of the ureter through the same port site and minimizes the size and number of incisions necessary. The laparoscopic technique, by the benefits of overview, makes it possible to obtain a CU for urinary diversion even in the smallest children. It also assures the shortest distance from stoma to bladder to facilitate easy and prompt drainage from the bladder in a refluxing CU. With the benefit of the internal view, kinks and torsion of the ureter are avoided. Finally, laparoscopy has the proven benefits of its minimal invasiveness: less postoperative pain, scarring, and infections. These smaller incisions are esthetically important, especially in the light of delayed reconstruction. Although very small incisions were used in the creation of the ureterostomy, no stenosis was noted on follow-up. In the approach we have used, the primary 5 mm port is transumbilical and therefore through a natural scar. One of the working ports (3 mm) is at the ureterostomy site and only the third 3 mm port is at a separate site, which is the only additional scar caused; therefore, cosmetic outcome is extremely good. So although three incisions are made, only one is actually additional and visible. The refluxing LA-CU has additional benefits when compared with a vesicostomy namely, potential improvement of bladder function, the possibility of bladder cycling and functional preservation of the ipsilateral kidney. 6 By preserving the refluxing lower ureteral stump it has the potential to also improve the function of the contralateral kidney.13,14 A duplex collecting system is a specific scenario in which the use of laparoscopy for temporary urinary diversion might be beneficial in comparison with the open technique and has not been reported so far. Our last case (Case 12; Table 1) is an 8-month-old infant with a left duplex collecting system in whom the upper moiety drained ectopically into the vagina. She presented acutely with pyrexia and purulent discharge from the vagina. Initially the upper moiety was drained through a nephrostomy. After a brief period of improvement the situation deteriorated again and LA-CU of the dilated ectopic ureter was necessary. Preoperative stenting of the orthotopic ureter was carried out. By laparoscopic approach we could safely dissect the inflamed common sheet of the duplex ureters more easily, identify the ureter of the upper moiety, and mobilize the correct ureter for tension-free exteriorization. A possible disadvantage of LA-CU is its transperitoneal approach. This may result in intra-abdominal adhesions compared with the possible retroperitoneoscopic or open retroperitoneal approach,2,15 but this is an extremely rare phenomenon in the light of many other transperitoneal urological interventions. The other drawbacks of this study are that it involves a small cohort of patients and that it is retrospective. Also of benefit would have been a comparison with a group in whom the technique was used in an open approach. A prospective comparative study would be of benefit to conclusively prove the benefits of the laparoscopic technique.
Conclusions
We may conclude that the laparoscopic approach for cutaneous ureterostomy even in very small children is feasible, safe, and has several potential benefits compared with the open approach; however, this needs a comparative prospective study.
Footnotes
Disclosure Statement
No competing financial interests exist.