
Abstract
Abstract
Introduction:
A key concern regarding laparoscopic pyloromyotomy (LP) lies with the process of learning this skill. The learning processes for open pyloromyotomy and LP appear to be different, with an earlier increased risk of perforation or incomplete pyloromyotomy (IP) for LP. Our aim was to develop a simple simulation tool to reduce these specific complications.
Materials and Methods:
A model of hypertrophic pyloric stenosis was created and inserted into a pediatric laparoscopic surgery simulator. A cohort of experts completed a six-item questionnaire, using a 4-point scale regarding the model's realistic nature and accuracy. Evaluation of the LP procedure was based on a dedicated Objective Structured Assessment of Technical Skills score. Surgical residents and students were enrolled for the final evaluation to assess the relative performance of trainees who had practiced with this model (Group 1) versus those who had observed its use (Group 2).
Results:
Reproducibility of the model construction was considered to be satisfactory. The experts agreed that the model accurately simulated essential components of LP (mean 3.03 ± 0.7). They scored significantly better than the residents (27.2 ± 1.8 versus 22.8 ± 2.9; P < .001), with a lower rate of complications. Group 1 (39 trainees) performed significantly better than Group 2 (26 trainees), with a significant decrease in the risk of an IP (P < .05).
Conclusions:
This model appears to be sufficiently accurate to teach LP. In light of this, it can be considered to be an efficient tool for LP simulation teaching in our fellows' educational program.
Introduction
A
This degree of risk is generally not acceptable to patients and their parents, whereas from a surgical point of view, the elevated risk can be a source of considerable stress. In light of this, we are proponents of early and effective simulation teaching, in addition to surgical supervision for trainees, with the aim of decreasing the rate of early complications.
Simulator teaching of LP has not been widely used to date for a variety of reasons, such as the accessibility of simulators in particular. Although our surgical task performance simulator 5 has yielded encouraging results, one of the reasons it did not undergo full development was that it was not readily reproducible. Our aim was hence to develop an efficient and reproducible simulation tool for teaching LP surgery techniques. The underlying intention was to reduce specific LP-related complications.
Materials and Methods
A reproducible model of HPS was generated using basic materials (Supplementary Data S1; Supplementary Data are available online at www.liebertpub.com/lap) that approximate the stomach and the swollen pylorus. This model was placed in a pediatric laparoscopic surgery simulator 6 so as to replicate a standardized workspace. The principle was to preferentially use readily available materials and a validated training box6,7 to make this model reproducible worldwide and at a minimal cost. Laparoscopic 3 mm instruments (i.e., forceps, knife, and spreader [ref 26180 VD and 26167 DFS, STORZ]; Gmbh&Co, Germany; and a camera (Quickcam-Logiteck; Carl Zeiss AG, Germany) were used. A short training session was devised, focusing on the three consistent steps of LP: a linear cut in the serosa, splitting of the muscle to begin the myotomy, and completion using the spreader (Supplementary Video S1. Supplementary Data are available online at www.liebertpub.com/lap). A preliminary study with 3 experts confirmed the feasibility and the overall accuracy of the model. A dedicated Objective Structured Assessment of Technical Skills (OSATS 8 ; maximal score = 35) score was used to evaluate the procedure: POSATS (Pyloromyotomy OSATS score) (Supplementary Data S2). This score focused above all on qualitative parameters, although it also took into account quantitative parameters, such as the time to completion. It aimed to differentiate the performance of experienced surgeons and residents, with attention being given to instances of MP and IP in particular. For this purpose, the model was carefully examined at the end of the procedure.
The first phase was the validation by the experts (Fig. 1). A cohort of pediatric surgeons were recruited who, given their extensive experience with LP, were considered to be referents in this area. They were asked to individually test the model at the 2016 French endoscopic surgeons' annual GECI meeting, after a standardized explanation and individual explanatory demonstrations. After having tested the model, they were asked to complete an anonymous six-item questionnaire, using a 4-point Likert scale regarding the accuracy of the model and the extent to which it reflects actual surgical conditions.
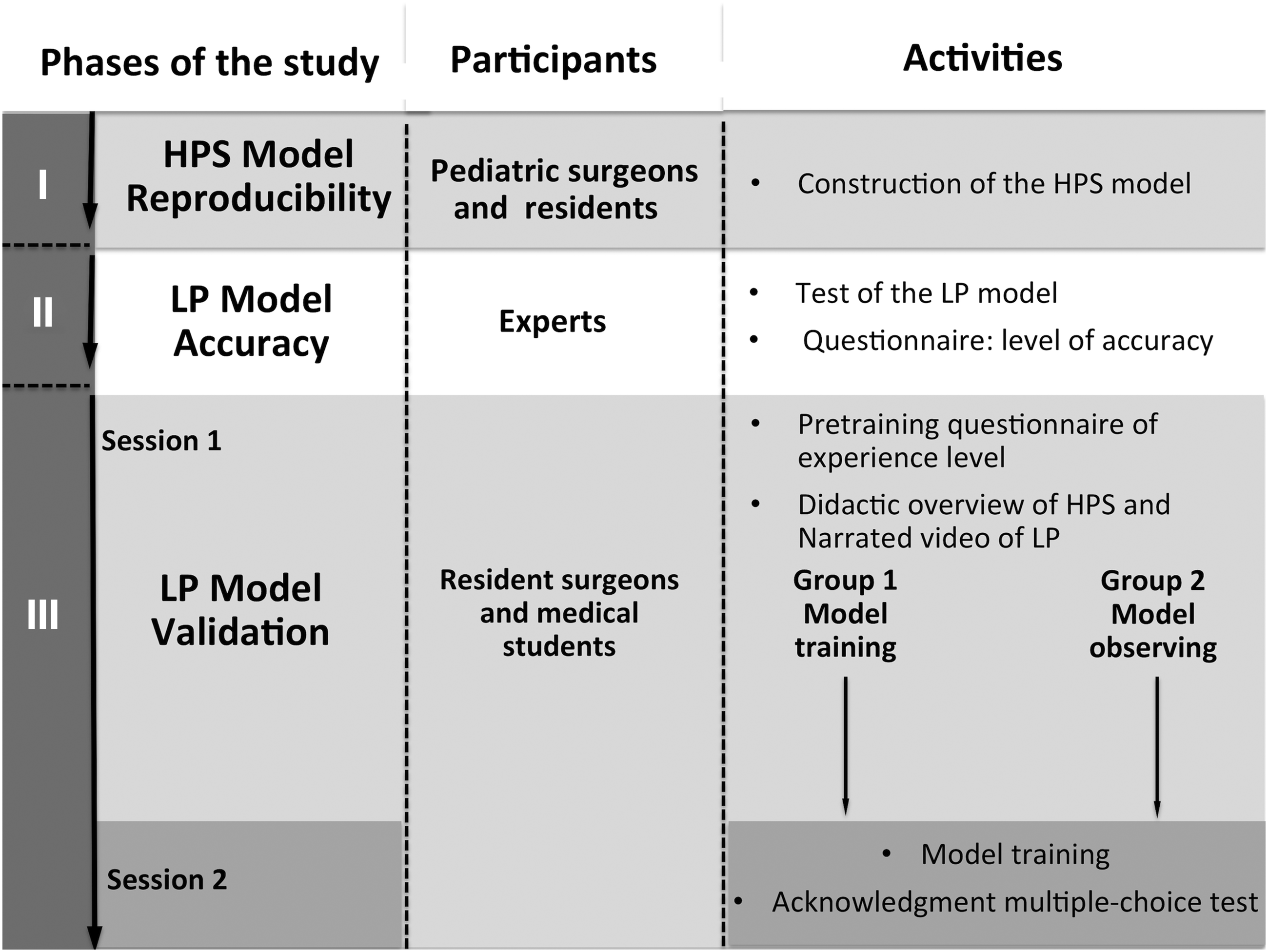
Design of the study. The model was tested with a three-phase study pattern. Models of hypertrophic pylorus stenosis were tested by pediatric surgeons as the first phase. The accuracy of the LP model was then assessed by experts before the contribution of its educational value was evaluated by comparing two groups with different levels of training with the model. HPS, hypertrophic pylorus stenosis; LP, laparoscopic pyloromyotomy.
The second phase aimed to evaluate the reproducibility of the HPS model assembly. A “do it yourself simulation kit” of HPS with associated instructions was sent to less experienced surgeons and residents of other pediatric surgical centers. It was requested that they return the results of their efforts with any eventual comments for an overall evaluation.
The last phase consisted of recruiting trainees to test the LP simulator. Participants were enrolled once they had signed consent forms and after approval was obtained from the Institutional Review Board. Two different groups were enrolled for the final testing phase of this model, comprising surgical residents from the general surgery program and fourth-year medical students. Before undertaking training, they completed a questionnaire regarding their level of experience with laparoscopy and their knowledge of LP. Preliminary standard oral explanations were provided, including a didactic overview of the HPS, an explanation of how the current model works, and narrated videos of LP. The subjects participated individually in the training.
They were divided into two groups. Group 1 performed the LP simulation using the current model immediately (session 1) and after a 3-month period of inactivity (session 2). Group 2 observed the simulation process at session 1 and performed the LP simulation at session 2.
All of the participants completed a multiple-choice test questionnaire at session 2 to assess the acquired cognitive information regarding LP. Evaluation of the LP procedure was performed by 2 independent researchers using both OSATS and POSATS scores. Data were recorded and collected by the 2 reviewers. A previous pilot study (unpublished data) had yielded a mean POSATS score of 25 for the experts (standard deviation = 2) and a score of 20 for the residents (standard deviation = 3). Using these data as a base, and seeking to demonstrate a difference of at least five points between the score for the experts and the residents, with an α-risk of 5% and a β-risk of 20%, we determined that this study would need a minimal total recruitment of 12 participants (i.e., 6 experts and 6 trainees). Statistical analyses were performed using GraphPad Prism 5.0 software (GraphPad, San Diego, CA). An unpaired t-test and Mann–Whitney test of independent samples were used to compare Group 1 and Group 2 scores and questionnaires. An ANOVA test was performed to compare the three subgroups of participants.
Results
The reproducibility of the model construction was deemed to be adequate. All of the requested centers supplied accurate reproductions of the original HPS model (Fig. 2) with adequate length and thickness of the swollen pylorus. The corresponding pediatric surgeons agreed that this homemade pylorus accurately simulated the key characteristics of the HPS and that it was easy to replicate.

Model of HPS.
A sample of 15 experts tested the current model. They agreed with the notion that the training model accurately simulated essential components of pyloromyotomy (mean score of 3.03 ± 0.7) (Table 1). In accordance with their comments regarding the strength for spreading, the type of silicone was modified for the last phase of the study. Their overall performance was 27.2 ± 1.8, the MP and IP rates were 1/15 (6%) and 0/15 (0%), respectively. The mean time for completion was 213 seconds (ranging from 125 to 742 seconds).
The 4-point Likert scale for the model's accuracy, and the extent to which it reflects actual surgical conditions.
HPS, hypertrophic pyloric stenosis.
In the last phase of the study, a total of 68 participants were enrolled, including 31 students and 37 residents. Of the 37 residents, 27 had already been exposed to LP in their clinical experience, although none of them had actually performed the procedure. None of the students had laparoscopic experience. Group 1 included 23 residents and 16 students (2 residents and 1 student were excluded from the group because they missed session 2). Group 2 included 12 residents and 14 students. No statistical difference was found between the two groups.
Experts scored significantly better than surgical residents concerning IP, MP, and POSATS scores (27.2 ± 1.8 versus 22.8 ± 2.9; P < .001), with a lower specific complications rate (Fig. 3). Similarly, resident surgeons performed significantly better than medical students, except for the MP score (Table 2).

Detailed performances by the experts and the residents. Specific POSATS score details highlighting each mean item score, with standard deviations, according to the level of expertise. Experts scored significantly better for each item. POSATS, Pyloromyotomy Objective Structured Assessment of Technical Skills.
IP, incomplete pyloromyotomy; MP, mucosal perforation; OSATS, Objective Structured Assessment of Technical Skills; POSATS, Pyloromyotomy Objective Structured Assessment of Technical Skills; SD, standard deviation.
Table 3 presents the comparison of performances for Group 1 and Group 2 in terms of surgical skills and cognitive acquired information. The knowledge-based test results were significantly better in Group 1 than in Group 2 for the students and the fellows (P < .01). Similarly, POSATS scores and complications rates were better in Group 1 than in Group 2, with a significant increase of the IP score in the fellows subgroup (3.8 ± 0.7 versus 3.1 ± 0.6; P < .05).
Mean surgical skills and acknowledgment scores 3 months after didactic information and model training (Group 1) or didactic information only (Group 2).
IP, incomplete pyloromyotomy; MP, mucosal perforation; POSATS, Pyloromyotomy Objective Structured Assessment of Technical Skills; SD, standard deviation.
Discussion
This study proposes a model to teach LP that can discriminate between surgeons and residents in terms of their level of skill with this procedure. Repeated practice with this accessible simulation tool can decrease LP-related and measured complications. It also appears to be a good support to increase the retained cognitive information.
The technical dexterity required to perform LP is greater than for its open counterpart. The initial part of the learning curve for LP was deemed to comprise ∼10 procedures, 9 with approximately a further 35 procedures being needed to reach a plateau for the surgical team. 3 The same author has confirmed that additional skills are acquired after an additional 35 procedures, thus leading to the concept of “the tail end of the learning curve.” 10 Vegunta et al. 11 reviewed their first 180 LP procedures, and they reported that the complications occurred primarily with the first 60 procedures. This indicates that a surgical team can still improve their laparoscopic technique skills after having performed a large number of procedures. Each surgeon's individual learning curve is of particular interest 4 as it focuses on specific complications and confirms that this risk is very substantial with the first 10 LP procedures. In light of these various reasons, surgical teaching for residents is highly advisable 12 and it could in fact be deemed to be crucial for safe performance of LP.
Another concern is with regard to the medical teaching for general surgical residents. Current reforms of surgical education in Europe have resulted in less exposure to operating theater procedures than has been the case for prior generations. The current implementation of a teaching program necessitates optimization of precious operating time for training. Conversely, it stresses the necessity of skills acquisition outside of the operating room, with a need for a specific curriculum to learn laparoscopic skills. This concept was largely described by the American College of Surgeons in terms of the Fundamental Laparoscopic Surgery (FLS) curriculum. 13 This FLS curriculum allows for general procedures that are common to many minimally invasive procedures to be practiced, such as cutting and sewing. The procedures involved with LP are, however, very particular as this type of surgery requires specific skills to be applied in the three previously detailed steps, which are nearly exclusive to this procedure.
Thus, the need for the development of a training model that has validity and efficacy is clear. In this case, the choice of a moderately representative model is debatable, although we chose it in light of its level of accessibility. The realistic nature and the reproducibility of the HPS model were enhanced in the first phase of the study. Credibility and realistic nature were confirmed by the group of experts before it was tested with the residents. The Likert scale used to measure the experts' agreement was the same as that proposed by Plymale et al. 5 As expected, the current level of accuracy was slightly lower than this previous model, 11 although it was still acceptable. The present tool has several limitations, as it is not a high-fidelity type of model. The main criticisms from experts were the hardness of the muscle, which sometimes led to difficulties with regard to the spreading maneuver, and the type of silicone was consequently modified. Surprisingly, the MP rate was higher for the resident group than for the student group. This observation perhaps illustrates the restraint in movements for laparoscopic-naive users, paradoxically resulting in a lower MP rate associated with a higher IP rate.
The main advantage of this model is its accessibility combined with a good educational contribution. The last phase of the study demonstrated that practicing with this simulation tool improved LP-related knowledge and the retention of specific surgical skills. The main limitation of this study is the absence of an indication that the acquired skills can be transferred to surgical practice. This will require further investigation of the model.
Conclusion
This proposed model appears to be straightforward, reproducible, and low cost, although it is also accurate enough for use as an aid to teach LP surgical techniques. In light of this, this training model has proven to be an efficient tool for early and effective LP simulation teaching in our surgical fellows teaching program. The ultimate goal for this approach would be to demonstrate that this model promotes the acquisition of LP skills that are transferable to the operating room, with a concomitant reduction in the rate of specific complications for the procedure in the learning curve for surgical fellows.
Footnotes
Acknowledgment
The authors thank R. Peymirat for his technical assistance with image editing.
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.