
Abstract
Abstract
Background:
Experience of peroral endoscopic myotomy (POEM) for treatment of achalasia in pediatric population is limited with varying techniques in different centers. The accurate extent of submucosal tunneling into the gastric cardia and the adequacy of myotomy are the important determining factors to success of POEM. A majority of studies in pediatric population have described using submucosal dye injection for assessing the adequacy of myotomy, however, this is a rather crude and inaccurate method. We herein describe the first case of pediatric achalasia managed with POEM incorporated with novel combined techniques using EndoFLIP® (Endoluminal Functional Lumen Imaging Probe) and double endoscope.
Methods:
Esophagogastric junction (EGJ) was identified with a gastroscope. Before POEM, EndoFLIP showed EGJ distensibility index of 1.7 mm2/mmHg. Submucosal tunnel was created from the mucosal entry site at midesophagus down and ∼3 cm beyond the EGJ. Anterior myotomy cutting the circular muscle layer while preserving the longitudinal muscle was performed for 8 cm. Double-endoscope technique was used to confirm the adequacy of myotomy by inserting a smaller endoscope through nostril into stomach and observing the transillumination of the first endoscope at the end of submucosal tunnel. After POEM, repeat EndoFLIP measurements revealed increased distensibility index to 6.0 mm2/mmHg. Endoscopic examination at the end of the procedure showed widely patent EGJ.
Results:
Eckardt symptoms score improved from 9 to 0. At 7 month after POEM, esophagoscopy showed widely open EGJ with no esophagitis, and high-resolution esophageal manometry revealed normalized lower esophageal sphincter pressure and resting tone.
Conclusions:
We introduced the intraoperative use of EndoFLIP system that allows real-time assessment of EGJ distensibility and immediate treatment effect evaluation. Incorporation of double-endoscope POEM was also first described in our pediatric patient for ensuring complete gastric myotomy. From our experiences, POEM for achalasia in pediatric population appears to have encouraging results similar to adult patients.
Introduction
A
Patient Presentation
A 11-year-old boy, who enjoyed good past health, presented with 4-month history of progressive dysphagia, repeated vomiting of undigested food, and weight loss. Regurgitation occurred shortly after ingestion and he developed progressive intolerance to both solid and liquid food with holdup sensation at retrosternal level and sometimes heartburn. He experienced marked weight loss of 9 kg in 4 months time. Physical examination was unremarkable except both the weight-for-height and body mass index-for-age dropped from 50th percentile to below 3rd percentile in months.
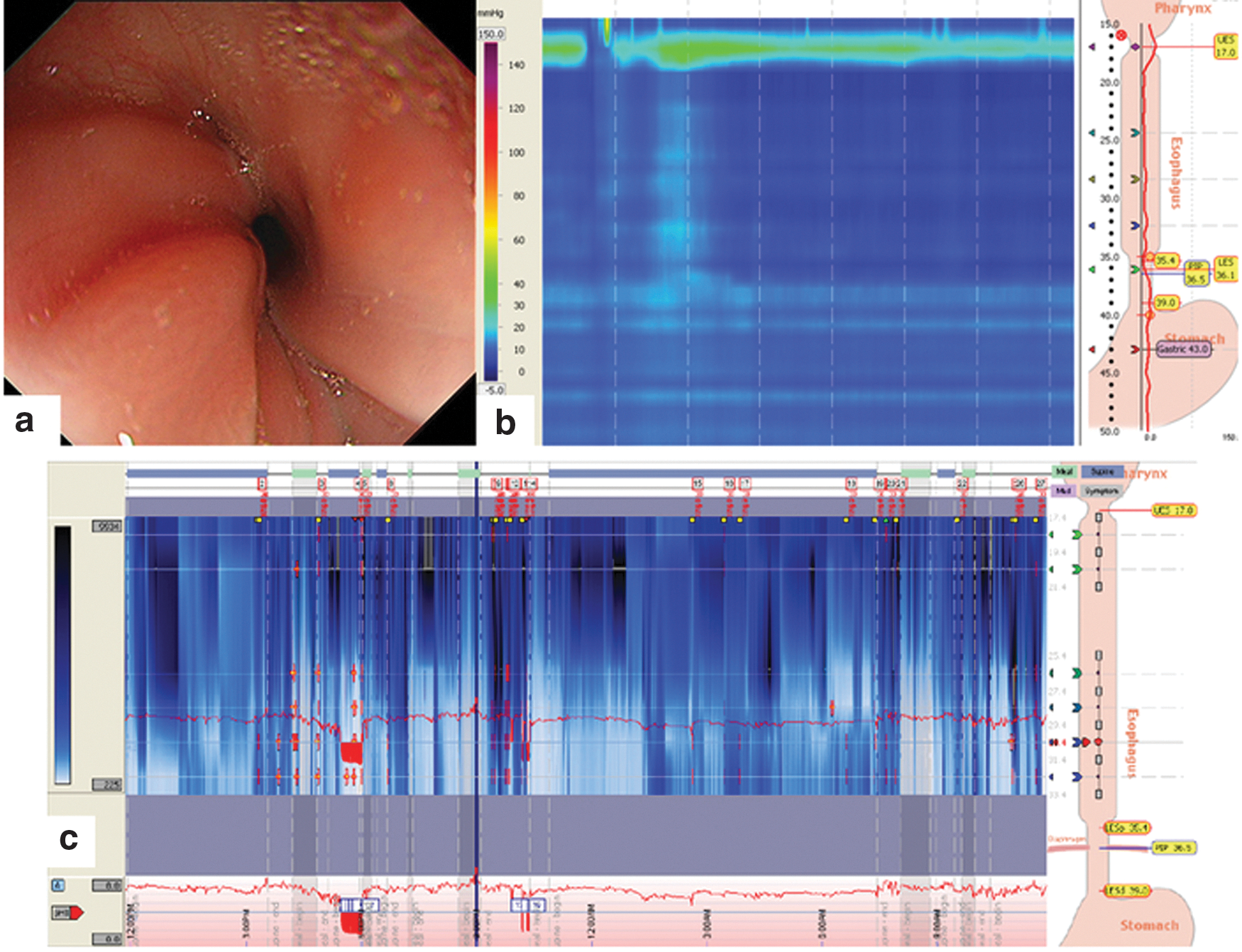
Esophagogastroscopy showed dilated esophagus with retained saliva and food residue (Fig. 1a) and tapered narrowing at EGJ (Fig. 1b). There was no mechanical obstruction. Barium swallow revealed dilated lower esophagus with decreased primary peristalsis but preserved tertiary contractions. Characteristic bird beak sign with pooling and stasis of barium was noted (Fig. 1c). Esophageal high-resolution manometry (HRM) revealed impaired EGJ relaxation with median integrated relaxation pressure of 31.5 mmHg for 10 test swallows and panesophageal pressurization representative of achalasia type II pattern according to Chicago classification (Fig. 1d). 7 Eckardt symptoms score was 9 (2 for weight loss; 3 for both dysphagia and regurgitation; 1 for retrosternal pain). 8

Operative technique
POEM was performed under general anesthesia. A 9.9-mm-diameter forward-viewing gastroscope (Olympus GIF-HQ190) was used. EGJ was identified at 36 cm from incisor. EndoFLIP was used intraoperatively before and after POEM. EndoFLIP involved a balloon catheter containing an array of electrodes and pressure transducers that measured impedance at different levels, which was inversely proportional to the cross-sectional area at that locus. The balloon was inflated to 30 mL to hourglass shape with the narrowest cross-sectional area at the level of EGJ. EGJ distensibility could, therefore, be calculated with this impedance planimetry technique by using the formula of narrowest cross-sectional area in mm2/intraballoon pressure in mmHg.9,10 Before POEM, the EGJ distensibility index was 1.7 mm2/mmHg, intraballoon pressure was 27.3 mmHg, and the minimal EGJ diameter was 8.5 mm. Submucosal injection of saline mixing with 0.3% indigo carmine and adrenaline (500:5:1 mL) using ERBE HybridKnife® was performed at 10 o'clock over anterior wall of the midesophagus at 28 cm level. Mucosa was opened longitudinally using ENDO CUT® Q mode of ERBE VIO® 300S machine (Fig. 2a). A submucosal tunnel was created from the mucosal entry site down and ∼3 cm beyond the EGJ (Fig. 2b), of which the position was confirmed by identifying the palisading vessels within the submucosal layer at the EGJ (Fig. 2c) and bluish discoloration of the gastric cardia mucosa on retroflexed endoscopic view in stomach (Fig. 2d). Anterior myotomy cutting the circular muscle layer while preserving the longitudinal muscle was performed with combination of End cut Q (effect 3, cut duration 1 or 2, cut interval 4) and coagulation mode (40 watts, effect 2) at 12 o'clock from 30 cm level toward the EGJ and 2 cm beyond (Fig. 2e). Double-endoscope technique was used to confirm the adequacy of myotomy by inserting a 5-mm-diameter endoscope (Olympus GIF-XP260 N) through nostril into stomach and observing the transillumination of first endoscope at the end of submucosal tunnel. After POEM, repeat EndoFLIP measurements revealed increased minimal EGJ diameter to 11.2 mm, decreased intraballoon pressure to 17.5 mmHg, and increased distensibility index from 1.7 to 6.0 mm2/mmHg (Fig. 2f). Mucosal opening was closed with hemostatic clips (Olympus EZ clips 90 degrees) (Fig. 2g). Endoscopic examination at the end of the procedure showed widely patent EGJ before decompression of stomach (Fig. 2h).

Gastrografin esophagogram was performed on postoperative day 1 and showed smooth passage of contrast without leakage. He tolerated fluid diet well without dysphagia or regurgitation and was fit for discharge on postoperative day 3. Antibiotics and proton pump inhibitors (PPIs) were prescribed for 1 week and 1 month, respectively. At 1-week follow-up after POEM, Eckardt symptoms score improved from 9 to 0 though he experienced mild nocturnal heartburn sensation, which was alleviated with PPI. At 7-month post-POEM, Eckardt symptoms score remained zero with weight gain of >11 kg and weight-for-height regained to 50th percentile since POEM. He had been asymptomatic and not requiring any PPIs. Reassessment esophagoscopy showed widely open EGJ with easy passage of endoscope with no esophagitis (Fig. 3a), and esophageal HRM revealed normal lower esophageal sphincter resting tone and residual pressure with median integrated relaxation pressure of 3.5 mmHg (Fig. 3b). Esophageal 24-hour pH–impedance study showed no significant reflux with DeMeester score of 12.3 (Fig. 3c).
Discussion
Experience of POEM for treatment of achalasia in pediatric population is limited. Maselli et al. first reported successful POEM in a 3-year-old girl with Down syndrome and achalasia and showed satisfactory treatment outcomes at 1-year follow-up in 2012. 11 Recently, Caldaro et al. compared the outcomes of 9 children who underwent POEM with another 9 patients who underwent LHM. 12 The authors concluded that the POEM group had shorter operation time, longer myotomy, and shorter hospital stay than the LHM group with no differences in clinical and manometric parameters on follow-up. The largest POEM study by far included 27 pediatric patients with POEM, in which 1 patient failed submucosal tunneling due to severe adhesion. 13 The clinical and manometric outcomes were satisfactory on 2-year follow-up.
The technique of POEM, however, has been modified in different centers. The accurate extent of submucosal tunneling into the gastric cardia and the length of myotomy are the important determining factors to success of POEM. Majority of the studies in pediatric population described the submucosal injection of indigo carmine–saline for identification of bluish discoloration at gastric cardia; however, this method is rather crude and inaccurate. In our case, we introduced the intraoperative use of EndoFLIP system using impedance planimetry during volumetric distension, which allows real-time assessment of the distensibility of EGJ and immediate evaluation of the treatment effects after POEM. 14 This technology has been found in adult population that the intraoperative EGJ cross-sectional area during POEM for achalasia correlated with postoperative symptomatic outcomes and reflux.15,16 Petrosyan et al. recently also described their use of EndoFLIP during both LHM and POEM, which aid in identifying the adequacy of myotomy. 17 Incorporation of double-endoscope POEM was first described in our pediatric patient for ensuring complete gastric myotomy by observing the transillumination of the dissecting endoscope at the submucosal tunnel with retroflexed view of gastric cardia using second endoscope. This double-endoscope technique has been found to result in more complete gastric myotomy with high rates of technical and clinical success in an adult study. 18 However, we have to acknowledge that this technique may not be universally applicable for smaller children or infants as the esophageal lumen might be too small to accommodate two endoscopes at the same time.
From currently available literatures, POEM for achalasia in pediatric population appears to have encouraging results similar to adult patients. However, larger case series with long-term follow-up and multicenter randomized trials are needed to establish the efficacy and safety of POEM in the pediatric population.
Footnotes
Disclosure Statement
No competing financial interests exist.