
Abstract
Abstract
Background:
Many laparoscopic techniques have been evolved along years for pediatric inguinal hernia (PIH) with no standardization of technique. No single technique suits all varieties of hernia.
Purpose:
To propose an algorithm for allocation of PIH to laparoscopic technique based on internal ring (IR) diameter to improve outcomes.
Patients and Methods:
Along 10 years, 459 cases with unilateral PIH were treated in Tanta University Hospital. In the first 5 years (phase I), 214 cases included then an algorithm for stratification was designed and applied in the second 5-year period (phase II), where 245 cases managed. This algorithm included evaluation of the hernia based on IR diameter as measured by the laparoscope from inside by a piece of suture. When the IR diameter is from 4 to 15 mm, complete sac disconnection is used. When IR diameter lies from 15 to 25 mm a purse string is added. When IR diameter is >2.5 cm or recurrent cases, the interrupted muscular arch repair after sac disconnection is used.
Results:
In phase I, 170 boys and 44 girls from 6 to 180 months of age were treated. All cases managed by laparoscopy were 84 herniotomy, 82 by purse string, and 44 by interrupted muscular arch. In phase II, 180 boys and 65 girls from 3 to 180 months of age were included. Eighty were managed by herniotomy, 137 by purse string, and 25 by interrupted muscular arch. Recurrence rate decreased significantly in phase II.
Conclusions:
Application of Tanta algorithm reduces the recurrence rate significantly. The laparoscopic technique should be tailored according to criteria of each group of PIH to get the best outcome and reduced recurrence rate.
Introduction
P
We proved that the herniotomy alone needs added step to ensure effective outcome. 5 Schier 3 advocates purse-string closure at the level of IR or with adding lateral peritoneal incision to reduce mechanical tension to the suture. Laparoscopic repair of PIH became a routine. 6 Despite that, no single technique is suitable for all cases.5,7 Actually, inguinal hernia has a range of pathological conditions with differences regarding age, gender, wideness of the IR, depth of pelvis, and condition of local muscles, so no single technique suits all cases of PIH. 5 Based on this fact, Mouravas and Sfoungaris 8 raised the question whether we should follow similar steps to open technique to get comparable outcomes.
Purpose
The aim of this work is to propose a correlative algorithm for proper allocation of PIH to define laparoscopic technique results in the best outcomes in pediatric age group in a tertiary academic center.
Patients and Methods
Four hundred fifty-nine consecutive (459) children with unilateral PIH who presented to the Department of Pediatric Surgery, Tanta University Hospital and other affiliated hospitals, Egypt, over a 10-year period (2006–2016) were included in our study. Exclusion criteria included premature infants below 3 months of age, with irreducible and recurrent hernia cases as a primary diagnosis. No special preoperative measures were required for laparoscopic hernia repair in children.
In the first 5 years (phase I), 214 cases were treated. Based on phase I experience and observations, a correlative algorithm for stratification was designed by the first author (Dr. Sherif Shehata) as depicted in Figure 1.
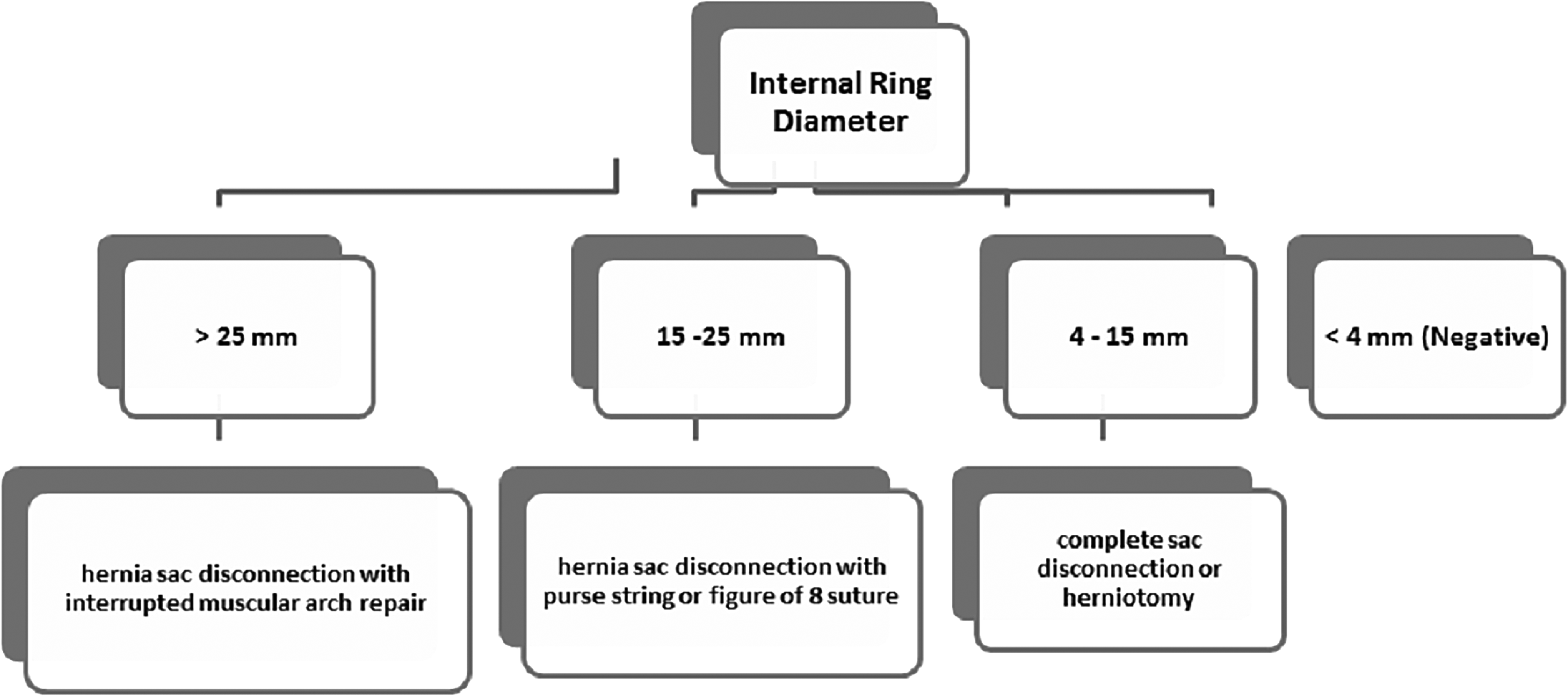
Graph representing the Tanta Correlative Algorithm for laparoscopic hernia repair based on internal ring diameter in millimeters.
This algorithm for stratification was applied in the second 5-year period (phase II), where 245 cases were managed after implementation of this algorithm. No special preoperative measures were required for laparoscopic hernia repair in children. All patients received general anesthesia with endotracheal intubation or laryngeal mask. In all patients, we had adopted the open technique to establish pneumoperitoneum. Intra-abdominal gas pressure ranging from 8 to 12 mmHg has been found to be sufficient for the procedure using 5 mm 30° telescope. All cases were subjected to laparoscopic exploration first, followed by LH by the same group. This algorithm included evaluation of the hernia side and contralateral side.
The diagnostic exploratory laparoscopy was first done for both inguinal regions being inspected from within the abdomen to confirm the clinical preoperative diagnosis and to detect any contralateral patent processus vaginalis (CPPV).
This algorithm included evaluation of the hernia side and contralateral side. Open processus of diameter <3 mm and/or <1 cm length was considered negative for exploration. This evaluation was done by the tip of the laparoscopic instrument with known diameter and length of tip until the insulated part of the laparoscopic instrument for CPPV. The IR diameter is measured laparoscopically from inside by a piece of suture along its longest diameter and measured outside on ruler at maximum diameter considering shape of the ring as seen in Figure 2. In cases where IR diameter ranges between 4 and 15 mm, herniotomy or complete sac disconnection (H subgroup) is used. 5 In cases where the IR diameter ranges between 15 and 25 mm, a purse-string or figure of eight stitch (PS subgroup) is added. 4 In cases with IR diameter >2.5 cm or recurrent cases, the interrupted muscular arch repair employing 3–4 sutures after sac disconnection is employed (MA subgroup) as our group published before. 9 Mesh is only used in bilateral cases with weak musculature.
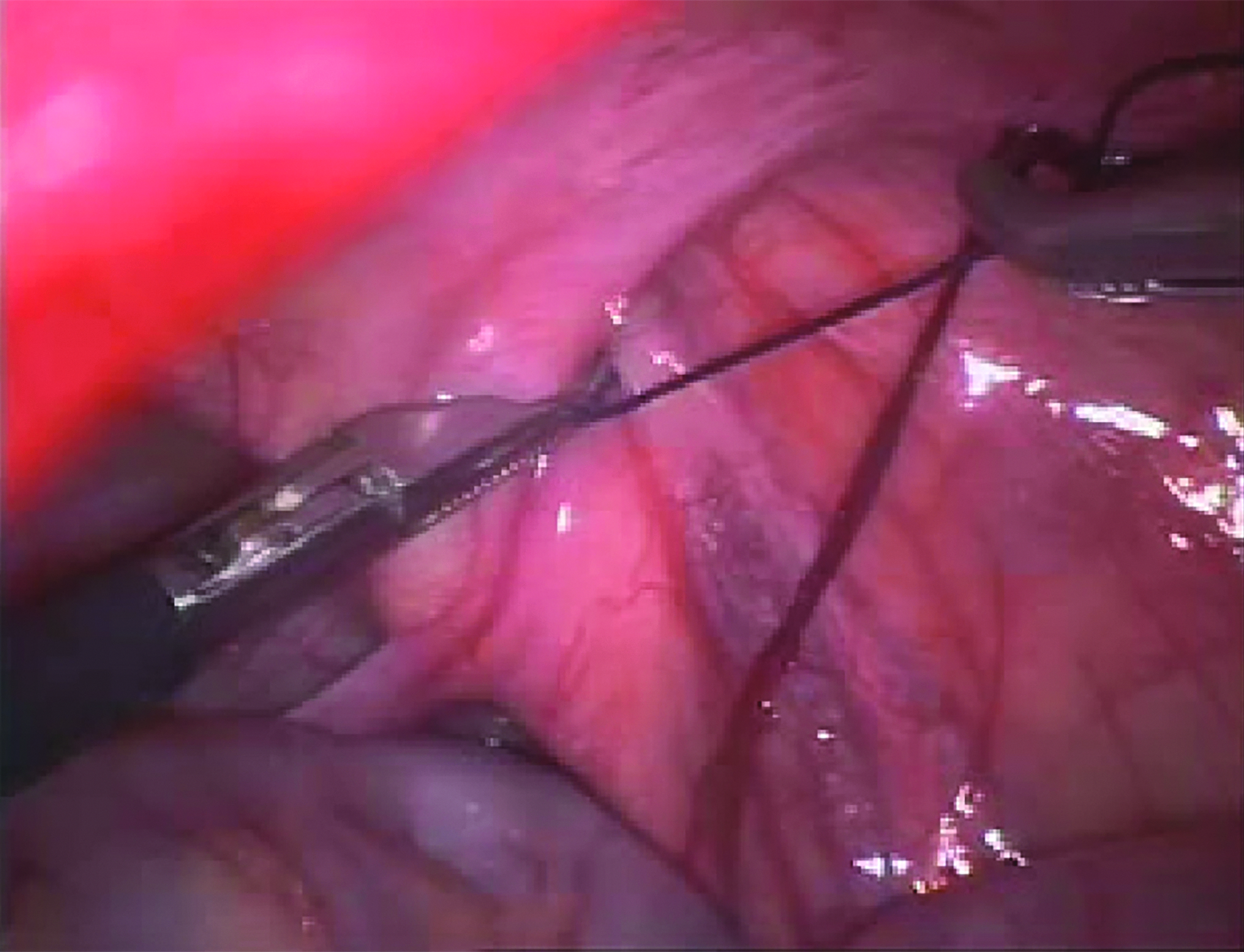
This photograph shows the laparoscopic view of the right inguinal hernia with a piece of Vicryl measuring the internal ring maximum diameter, from medial to lateral aspects as grasped between two Maryland foreceps. The nonfree foreceps is then taken to the outside where the diameter is measured with a regular ruler.
All cases were discharged the next morning. Patients are transferred to their wards and received medical treatment in the form of the second dose of IV first-generation cephalosporin—first one been given at the time of induction—and a nonsteroidal anti-inflammatory suppository was used for postoperative analgesia along the first 48 hours following the procedure as needed. Oral fluids were started when bowel sounds were audible. Operative findings and postoperative results and complications were assessed and reported during the follow-up period that ranged between 6 and 60 months. Follow-up protocol included outpatient visits at 1 week, 1, 3, and 6 months postoperatively, then by phone call every 6 months, thereafter until 3 years, and outpatient clinic visit arranged when needed. Recurrence was compared in both phases.
Results
In phase I, we have 214 cases of 170 boys and 44 girls with age ranging between 6 months and 15 years (mean of 19.1 months). All cases were managed by laparoscopy, where 84 were managed by herniotomy, 82 by purse string after sac disconnection, and 44 by interrupted muscular arch repair, including 15 recurrent cases excluding the 4 cases managed by Mesh hernioplasty. The IR diameter ranges were 26–42 (mean: 31.1) mm, 15–25 (mean: 19.8) mm, and 4–15 (mean: 8.9) mm in MA, PS, and H subgroups, respectively, in phase I. Operative time in phase I ranged between 20 and 85 minutes with a mean of 38.3 minutes. When the phase I group was subdivided according to operative time, we found it was 24–85 minutes (mean of 51 minutes), 23–60 minutes (mean of 38.7 minutes), and 20–50 minutes (mean of 31.5 minutes) in MA, PS, and H subgroups subsequently in phase I.
In phase II, we have 245 cases of 180 boys and 65 girls with age ranging between 3 months and 15 years (mean of 17.6 months). All cases were managed by laparoscopy, where 80 were managed by herniotomy, 137 by purse string after sac disconnection, and 25 by interrupted muscular arch repair, including 12 recurrent cases excluding the 3 cases managed by mesh hernioplasty. The IR diameter ranges were, 26–42 (mean: 32) mm, 15–25 (mean: 19.4) mm, and 4–15 (mean: 9.2) mm in MA, PS, and H subgroups, respectively, in phase II. Operative time in phase II ranged between 20 and 85 minutes with a mean of 36.1 minutes. When the phase II group was subdivided according to operative time, we found it was 35–70 minutes (mean of 51 minutes), 20–85 minutes (mean of 38.2 minutes), and 12–46 minutes (mean of 27.8 minutes) in MA, PS, and H subgroups subsequently in phase II.
Seven cases, including the 5 boys with bilateral hernia were managed by mesh hernioplasty in the two phases. Follow-up period ranged between 6 months and 5 years. The mean follow-up period in phase I cases was 16.5 months, whereas it was 15.5 months in phase II. When comparing the different subgroups among both phases according to surgical procedure category using nonparametric test regarding age, operative time, IR diameter, and follow-up time, the only significant comparison was that the operative time in LH subgroup in phase II was reduced as compared with phase I with P of .001. Recurrence rate decreased significantly in phase II to 1.2% (3 out of 245) after application of Tanta algorithm as compared with 3.7% (8 out of 212) in phase I, where P value was .016 using nonparametric test. All recurrences do appear in the first 6 months postsurgery.
Discussion
The advantages of the laparoscopic approach include the following: a procedure that clarifies and treats both sides in one session; any open CPPV or rare hernia can be detected during laparoscopy and closed immediately; trocar position is the same for both sides; excellent visualization of the cord structures; and they can be guarded well during the procedure.9–11 Children ≤3 years of age in a cohort safely underwent LH with similar pain scores, complications, and recurrence as open herniotomy. 11 Similarly, we reported excellent results in the same age group with mean age of 19.1 months in phase I and mean age of 17.6 months in phase II. In literature reports, recurrence rates are similar between the two studied laparoscopic methods (levels 1a and 1b evidence). 12
Comparison of demographics of both phases in our study, regarding the age, gender, and follow-up period, shows no statistical differences. No level 1 evidence exists to support one laparoscopic technique over another or that operating on a detected CPPV during laparoscopy makes any difference in long-term outcome to the patient.12,13 So, we propose the Tanta correlative algorithm to laparoscopic repair of inguinal hernia repair in children, as no single technique is suitable for all sizes and ages of PIH. 14 Evermore, in older boys recurrences are increased following laparoscopy as the retained area of peritoneal sac is large or the suture material gave away with intact preformed sac as reported in experimental rabbit model 15 and human. 16
Choosing the measurement values are based on our observations and literature review. Considering the value of 3 mm IR diameter of negative hernia is supported by the findings of Treef and Schier 17 that cases were excluded if they only had openings of <3 mm in recurrent cases, obviously too narrow to allow bowel prolapse. Complete circumferential incision may lead to a reduction of the recurrence rate because of the scarring involved as applied in open technique. This is the first step of procedure in all cases included in our study whatever the laparoscopic technique will follow.
This fact is supported by our work 5 and others. 18 Tanta correlative algorithm with cutoff at 15 mm IR diameter as candidate for LH alone is supported by the current findings of reduced recurrences in phase II allowing proper allocation of hernia case under study to which laparoscopic procedure. This is supported by Riquelme et al., 18 and others who advocate adding suturing in cases with IR around 2 cm.19,20 In the current study, we take 15–25 mm IR to be subjected to laparoscopic purse-string suture after complete sac disconnection in phase II to minimize the observations of some recurrence in phase I. Treef and Schier 17 reported that it is interesting that true circumferential ligatures, as they are applied in open hernia repair techniques, when performed laparoscopically yield lower recurrence rates as we applied in our study.
As inguinal hernia pathogenesis in pediatric age is multifactorial, age, gender, weight, muscle condition of canal, and IR diameter are all contributing factors to the outcome.17,21 The interrupted muscular arch repair is an excellent solution to cases with wide rings as we reported earlier,9,22 and will prevent tearing or tension repair by single purse-string suture.9,17,23 Hence, the proposed Tanta correlative algorithm we applied in phase II showed improvement in results mainly in statistical reduction of recurrence rate from 3.7% in phase I to 1.2% in phase II with P value of .016. This rate of recurrence is comparable to rate of open hernia repair that ranged between 0.4% and 8% in literature.24,25 In our study, we presented our experience along 10 years of laparoscopic hernia repair. We reported that recurrences usually developed in the first six postoperative months as reported by many.6,26
In our study, the significant reduction in operative time from 31.5 to 27.8 minutes in LH repair in phase II as compared with phase I could be attributed to the experience and learning curve of the whole team, surgery, anesthesia, and operative room nursing. Experience is of paramount importance to get excellent outcome. 6 We reported no conversion and tailoring the laparoscopic procedure to the characteristics of IR in unilateral PIH. Esposito et al. 27 reported similarly, no conversion in 1833 hernia repairs. Since no single laparoscopic technique suits all cases of PIH, the need of algorithm to allocate the case of PIH individually to laparoscopic procedure is warranted.6,27
To our knowledge, this is the first correlative algorithm to categorize PIH cases according to IR diameter with subsequent correlation laparoscopic approach. Tanta IR correlative algorithm provides a simple stratification guide based on IR diameter to allocate PIH cases to the suitable laparoscopic approach as documented from the results of the current study.
Conclusions
No single laparoscopic technique is suitable for all inguinal hernias as we are facing a disease of wide range. We apply the golden steps of open repair in different laparoscopic techniques. All types of PIH can be managed laparoscopically without conversion. Application of Tanta IR correlative algorithm reduces the recurrence rate significantly. The laparoscopic technique should be tailored according to criteria of each group of PIHs to get the best outcome and reduced recurrence rate.
Footnotes
Disclosure Statement
No competing financial interests exist.