
Abstract
Abstract
Background:
Laparoscopic surgery is widely used in the treatment of Hirschsprung's disease (HD). However, constipation and soiling are still the main long-term complications. A new type of anastomosis, which is characterized by a heart-shaped colorectal anastomosis after splitting the posterior rectum wall to 0.5 cm above the dentate line, has been improved by our medical center. The purpose of this study was to determine the long-term effects of laparoscope-assisted heart-shaped anastomosis (LHSA) and to compare it with a more generally applied approach, the laparoscope-assisted Soave procedure (LSP).
Patients and Methods:
In this retrospective study, we investigated the symptoms of chronic constipation and soiling in 56 patients after LHSA and 54 patients after LSP between 2005 and 2011.
Results:
For LHSA, the median age at surgery was 1.4 years (0.2–7.3), and the median follow-up time was 7.1 years (5–11.3). For LSP, the median age at surgery was 1.2 years (0.1–6.2) and the median follow-up time was 7.0 years (5–9.3). Constipation was less frequent after LHSA than after LSP (7.1 versus 22.2%, P = .025), but there was no difference in the frequency of soiling after LHSA compared with that after LSP (8.9 versus 14.8%, P = .339).
Conclusions:
The improved anastomosis (LHSA) preserves most of the internal anal sphincter, and the wide anastomosis prevents stenosis as well. In the long-term follow-up results, the incidence of constipation after LHSA declined when compared with that after LSP, and soiling showed a satisfactory result. Our medical center has performed laparotomy-assisted heart-shaped anastomosis since the 1990s and LHSA since the 2000s. Because it is easy to learn and provide good outcomes, many medical centers in China have adopted the heart-shaped anastomosis to treat HD. Using the LHSA method to manage the affected bowel provides satisfactory long-term outcomes, that is, avoiding constipation and soiling. Thus, LHSA may provide a new choice for HD operations.
Introduction
H
Patients and Methods
Patients
A total of 367 patients with HD underwent surgery between January 2005 and December 2011 in a single medical center. The diagnosis was made by postoperative pathological examination. Among these patients, 139 were operated on using a laparoscope-assisted procedure in our institution. No patients were diagnosed with Down Syndrome, hypothyroidism, anorectal malformations, or total colonic aganglionosis. Eleven patients who accepted stage operation (n = 8) or reoperation (n = 3) were excluded to minimize bias. Eighteen patients were lost to follow-up for a lost rate of 12.9%. Ultimately, 110 patients were enrolled in this retrospective study. Among these 110 patients, 56 patients underwent LHSA and 54 patients underwent LSP. The LHSA group included 12 girls and 42 boys, and the LSP group included 14 girls and 42 boys.
The surgery methods were randomly selected. The purpose of this study and the potential risk of the procedure were fully explained to the patients' legal guardians. Informed consents were also signed. A single surgeon performed all of the procedures at the Pediatric Surgery Department of Tongji Hospital at the Huazhong Science and Technology University (Wuhan, China). Our study was approved by the ethics committee of the Tongji Hospital, and it adhered to the tenets of the Declaration of Helsinki. The diagnoses were confirmed by both frozen sections during surgery and postoperative histopathological studies of paraffin sections. Preoperatively, we gave patients colonic irrigation with normal saline for 7 days and oral metronidazole for 3 days for colon preparation.
Follow-up information was obtained by outpatient visits, detailed telephone interviews, and mail communications. We then recorded demographic data and postoperative outcomes including constipation and soiling. The Krickenbeck criteria were used to assess constipation and soiling 10 (Table 1). An Excel spreadsheet specifically designed for this study was used to record all the data.
Surgical technique
Laparoscopic access was established using the method described in our previous articles. 11 Biopsies of three or four places in the seromuscular layer of the colon were carried out by rapid frozen sections to determine whether the submucosal nerve plexus and ganglion cells were present. Resection lengths were confirmed with intraoperative biopsies and preoperative examinations such as barium enemas. The colon was then mobilized from 5 cm proximal to the most distal bowel with normal nerve plexuses and ganglion cells to the peritoneal reflection of the rectum. Anastomosis followed. The Soave anastomosis is the same as the classic procedure. 12 The heart-shaped anastomosis is a modified procedure for HD, and it has been widely used in many Chinese medical centers since the 1990s. It is characterized by a posterior longitudinal anorectal split followed by a heart-shaped anastomosis. Previous articles by our centers reported the detailed methods.13,14 First, an olive-shaped dilator was inserted into the upper rectum through the anus, and with the assistance of the laparoscope, the dilator was tied to the aganglionic bowel. The colon was then pulled out and everted (Fig. 1). This could also be done with sponge forceps. After the rectum was incised, the affected bowel was pulled out until normal colon was identified as determined by the intraoperative biopsy. Subsequently, the affected bowel was resected, and a longitudinal split was made in the posterior wall of the anorectal canal ∼0.5 cm above the dentate line (Fig. 2). Finally, the seromuscular layer of the remaining rectum and the normal colon were sutured. Remarkably, the anterior anastomosis was 4 cm above the anal verge, but the posterior anastomosis was 1.5–2.0 cm above the anal verge (Figs. 3 and 4).

An olive-shaped dilator is inserted into the lumen of rectum and is fastened. Then the bowel is pulled through the anus and is everted.

A longitudinal split is made in the posterior wall of anorectal canal about 0.5 cm above to dentate line.
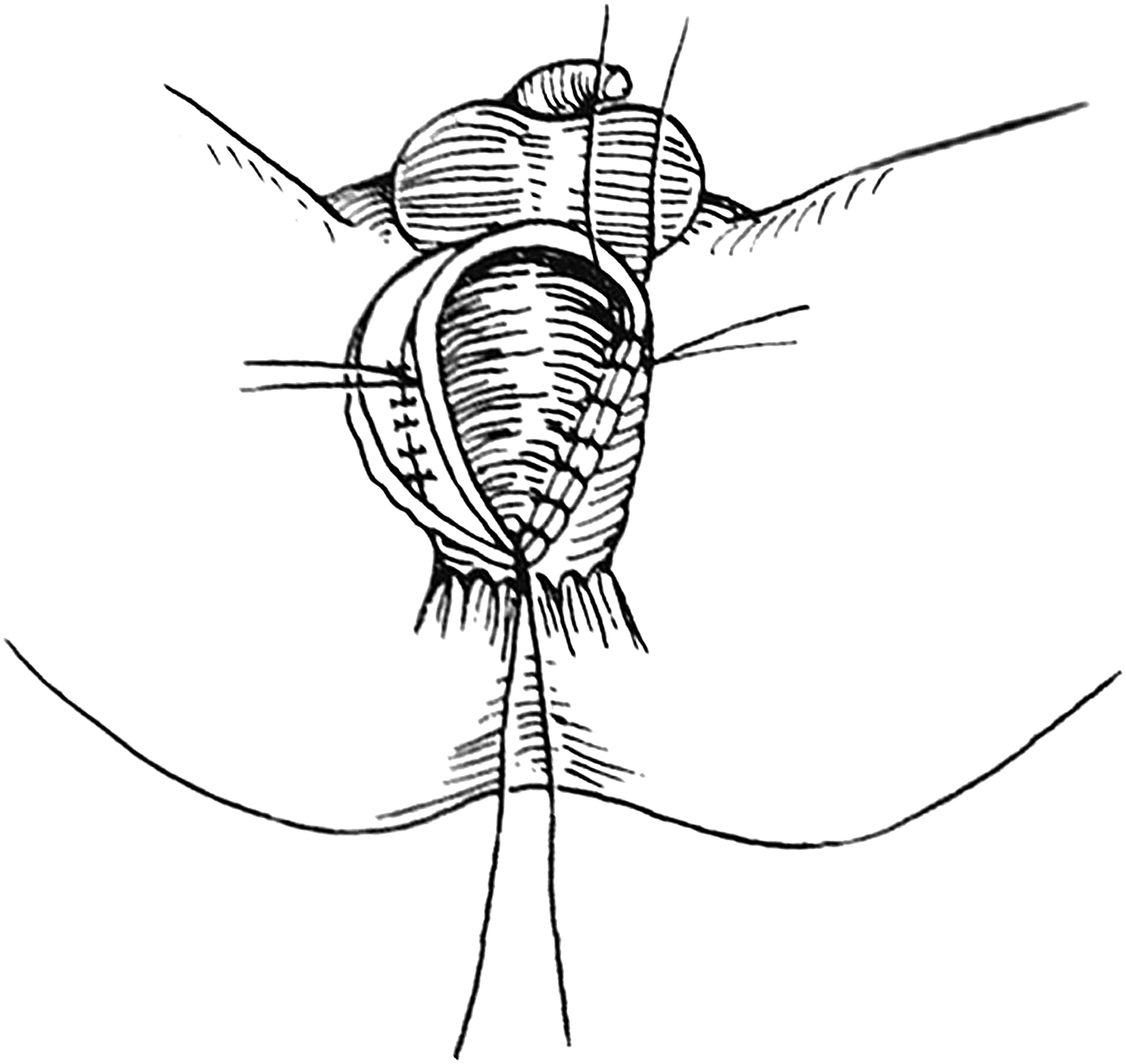
The anterior anastomosis is 4 cm above the anal verge, but the posterior anastomosis is 1.5–2.0 cm above the anal verge.
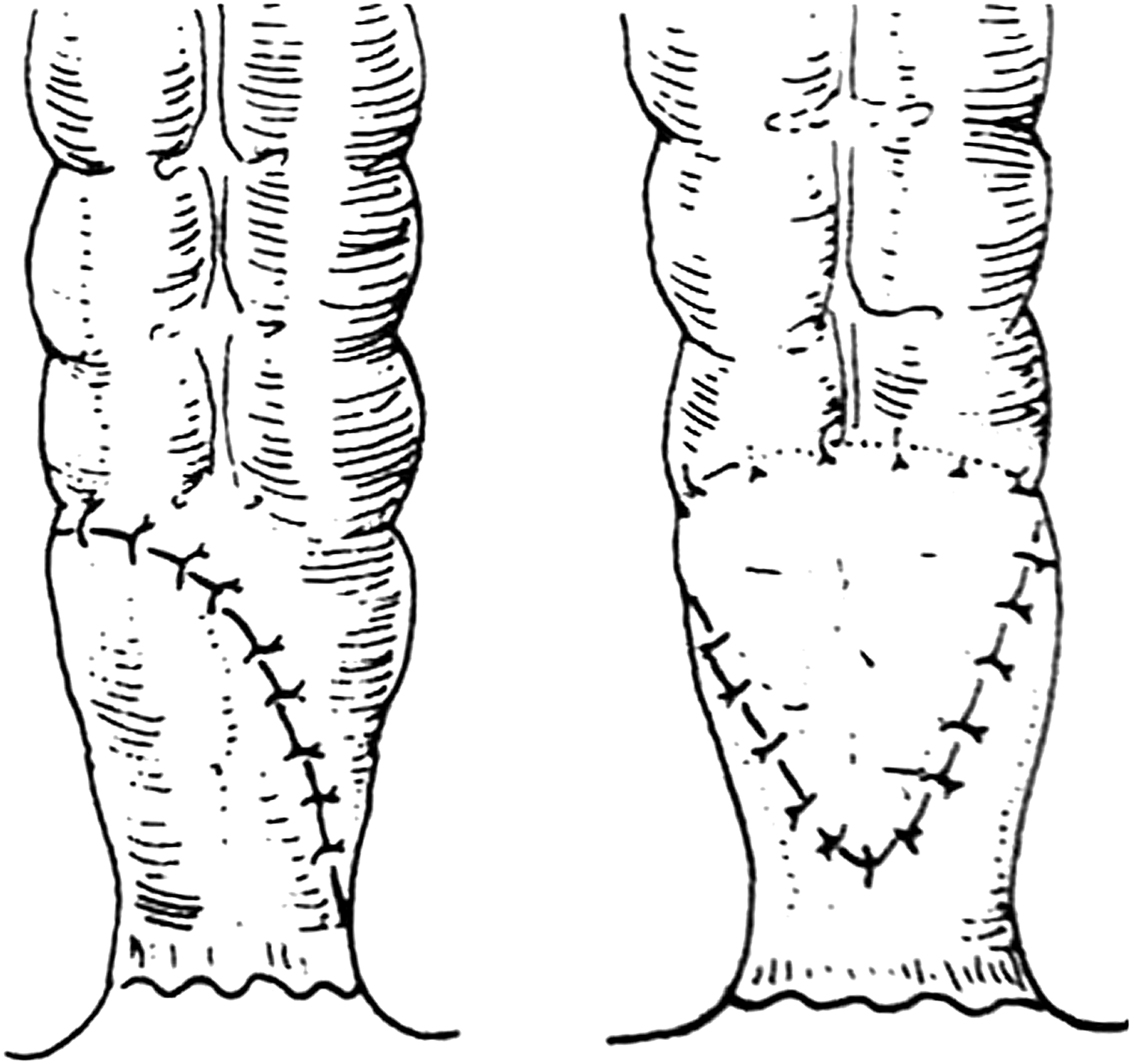
The completed anastomosis is heart shaped.
Statistical analysis
Statistics for all variables were calculated using SPSS Version 17.0. According to actual data, dichotomous variables were analyzed by χ2 tests or continuity correction χ2 tests. Student's t-test was used to analyze continuous parameters. All statistical tests were two sided. P values <.05 were considered statistically significant.
Results
Between 2005 and 2011, there were 110 patients who met the inclusion criteria, with 56 patients in the LHSA group and 54 patients in the LSP group. The LHSA group consisted of 42 males and 14 females, and the LSP group consisted of 42 males and 12 females (P = .732). Gender distribution was in accordance with the epidemiological features of HD. The mean patient age at the time of operation was 1.6 ± 1.2 years in the LHSA group and 1.7 ± 1.6 in the LSP group (P = .689). The mean patient age at follow-up was 9.1 ± 1.9 years in the LHSA group and 8.7 ± 2.1 years in the LSP group (P = .214). Mean follow-up time was 7.5 ± 1.7 years in the LHSA group and 7.0 ± 1.3 in the LSP group (P = .052). The length of removed bowel was analyzed in this study, and the LHSA group included 15 subcolectomies and 41 left colectomies, and the LSP group included 18 subcolectomies and 36 left colectomies (P = .454). All the mentioned characteristics did not differ significantly between groups (Table 2).
LHSA, laparoscope-assisted heart-shaped anastomosis; LSP, laparoscope-assisted Soave procedure; SD, standard deviation.
Table 3 gives the long-term complications after LHSA and LSP. In this study, constipation and soiling are the main complications that were noted. Krickenbeck classification (Table 1) was used to classify the grade of constipation and soiling. Constipation was defined as few voluntary bowel movements. Soiling was defined as more than one involuntary bowel movement, consisting of small quantities and liquid stools, between two voluntary bowel movements. Grades 1, 2, and 3 of constipation are characterized as being manageable with diet, requiring laxatives, and resistant to diet and laxatives, respectively. Grades 1, 2, and 3 of soiling are characterized as occurring occasionally (once or twice per week), occurring every day with no social problems, and occurring constantly with subsequent social problems, respectively. Four cases (7.1%) in the LHSA group and 12 cases (22.2%) in the LSP group reported constipation in this long-term follow-up (P = .025). In the LHSA group, 4 cases (7.1%) were classified as grade 1 and 10 cases (18.5%) in the LSP group were classified as grade 1 (P = .074). However, there were 2 of 54 patients (3.7%) in the LSP group with grade 2 constipation, and none in the LHSA group (P = .459) had grade 2 constipation. No patients were classified as having grade 3 constipation in either group. Soiling occurred in 5 of 56 patients (8.9%) from the LHSA group and 8 of 54 patients (14.8%) from the LSP group (P = .339). All 13 patients with soiling were classified as grade 1. These patients complained that soiling occurred occasionally, and they had no social problems.
P < .05.
LHSA, laparoscope-assisted heart-shaped anastomosis; LSP, laparoscope-assisted Soave procedure.
Discussion
In 1995, Georgeson described the primary laparoscopic pull through for HD patients. 15 Mobilization of the sigmoid colon and proximal rectum was completed with the assistance of the laparoscope, the affected colon was pulled out and removed through the anus, followed by perineal anastomosis. The Swenson, Duhamel, and Soave endorectal pull-through procedures have all been done laparoscopically. 16 Compared with open surgery, laparoscopic surgery shows good outcomes. It is minimally invasive with shorter hospital stays, blood loss is minimized, and there are cosmetic benefits. In addition, the laparoscopic pull through has complications similar to open surgery.16,17 Thus, the laparoscopic pull through is widely used in the treatment of HD. However, postoperative complications are always the most difficult problems to solve. To date, regardless of the procedure doctors select, some patients endure constipation and soiling, which may cause social problems and mental issues.16–18
In the Swenson procedure, after the full thickness of rectum is removed, the normally innervated bowel is anastomosed just above the anal sphincter. The resection of the bowel is inside the pelvis. In the Duhamel procedure, the normally innervated bowel is brought down and anastomosed with a stapler to the back of the aganglionic rectum just above the anal sphincter. Thus, in the new lumen, the aganglionic rectum is anterior and the normally innervated bowel is posterior. In addition, the internal sphincters are resected in the posterior wall. In the Soave procedure, after striping mucosa from the underlying muscles above the dentate line, the normally innervated bowel is brought down and anastomosed inside the muscular cuff above the anal sphincter. Thus, two layers of bowel wall exist, although a split may be done in the outer layer. 19 LHSA is the laparoscopic pull-through procedure with a “heart-shaped” anastomosis. It is a modified operation for HD, and it has been used in many medical centers in China since the 2000s. Remarkably, the anastomosis is heart shaped and is higher anteriorly and lower posteriorly. Intraoperative injury, bowel management, and anal sphincter preservation are closely related to the defecation function. In the long-term outcomes, anal sphincter dysfunction and intraoperative nerve injuries may be the main causes of constipation and soiling.
In this study, the incidence of constipation was 7.1% in the LHSA group and 22.2% in the LSP group (P = .025), which suggested that LHSA might be a better choice to avoid constipation. In addition, no grade 2 constipation cases (classified by Krickenbeck classification) existed in the LHSA group, but 2 cases were present in the LSP group. Laxatives are needed to maintain normal bowel movements in grade 2 constipation. In the Soave procedure, because part of the aganglionic muscular layer and almost all of the internal anal sphincter are preserved, constipation is more frequent and more severe. The incidence of soiling was 8.9% in the LHSA group and 14.8% in the LSP group (P = .339), this was also a good outcome. In the LHSA procedure, the posterior internal sphincter is resected, and the anterior sphincter is retained. Therefore, the internal sphincter is persevered to a great extent not only to avoid soiling but also to ensure that the anastomosis is wide enough to avoid the internal sphincter spasm syndrome, and thus prevent constipation.13,14,20 In the Swenson procedure, long-term management of affected bowel in the pelvis may cause contamination as well as injury to the nerves and other pelvic organs. However, in the LHSA procedure, after bowel mobilization, resection and anastomosis are completed outside the pelvis. This procedure prevents injuries and contamination, and it improves the outcome of HD surgery. In the Duhamel procedure, because of its unique anastomosis, a blind rectal pouch or septum may occur, and the internal sphincters of the posterior rectum wall could be destroyed. In contrast, the heart-shaped anastomosis is performed end-to-end that avoids such complications.
Owing to its retrospective nature, small sample size, and follow-up loss, this study has its limitations. Because this was a retrospective study and the standard randomized trial had not been designed before the operation was performed, it was not a strict, standard randomized trial. The inherent bias of the nonrandomized approach limited its significance. However, doctors chose the operation method randomly, and the opportunity was identical between the two groups. Therefore, the results were still meaningful to some extent, although a randomized trial would be preferable. To research the outcome of LHSA further, large-scale, multicenter, prospective clinical research should be launched. In addition, because of the wide anastomosis after LHSA, dilation postoperation may be omitted, and further study is needed to support this treatment.
Footnotes
Acknowledgments
This work was supported by the National Natural Science Foundation of China (81571478) and the Natural Science Foundation of Hubei Province (2015CFB658).
Disclosure Statement
No competing financial interests exist.