
Abstract
Abstract
Introduction:
Piriform fossa sinus tracts (PFSTs) are a cause of recurrent neck infections in the pediatric population. Conventional management required open resection, but over the last years minimally invasive approaches have been reported in an attempt to endoscopically obliterate the PFST, using different methods such as electrocautery, laser, trichloroacetic acid, or silver nitrate.
Materials and Methods:
We undertook a retrospective review of the medical records of 12 children (aged 4 months to 14 years) with PFSTs treated with endoscopic sclerosis with diathermy (ESD) between 2010 and 2016 at a tertiary care children's hospital. We also present a technical modification of ESD, using continuous infusion of airflow through the gastroscopy, to distend the piriform sinus and facilitate its recognition. PFST obliteration was performed using diathermy through a guide wire.
Results:
Clinical presentation of the 12 affected children included neck tumor (7 [58%]), neck abscesses (4 [33%]), and thyroiditis (5 [41%]). All lesions occurred on the left side. All patients underwent both ultrasonography and barium esophagography (the latter being positive only in 50%). Two patients were treated with ESD after the open approach had failed. There was no procedure-related morbidity. One patient had a recurrence (positive barium swallow without symptoms). The success rate of this procedure in our series was 91% with one attempt and 100% with two attempts.
Conclusion:
In our experience, treatment of PFST with ESD is a reproducible, noninvasive, and an effective option. ESD could be considered a primary approach and also for revision after open surgery has failed in these patients.
Introduction
A
Barium swallow, ultrasonography, and computed tomography scan are useful, but the definitive diagnosis is confirmed by laryngoscopy. 2
Conventional surgery consists of an excision of the fistulous tract with or without partial thyroidectomy by a cervical approach.
Over recent years, minimally invasive endoscopic techniques to obliterate the PFST have been performed in many institutions.3–8 Electrocautery is the most commonly reported technique for endoscopic obliteration, but several methods of obliterating the PFST have been described.
The objective of this study is to present our results using a slightly modified technique of endoscopic sclerosis with diathermy (ESD).
Materials and Methods
We undertook a retrospective medical review of 12 cases of PFST treated in the La Fe Hospital (Valencia, Spain) from 2010 to 2016. The diagnosis was suspected by the presence of a neck mass. We used barium swallow (Fig. 1) and ultrasound in all patients and tomography scan and magnetic resonance imaging (MRI) when there were any doubts before performing laryngoscopy.
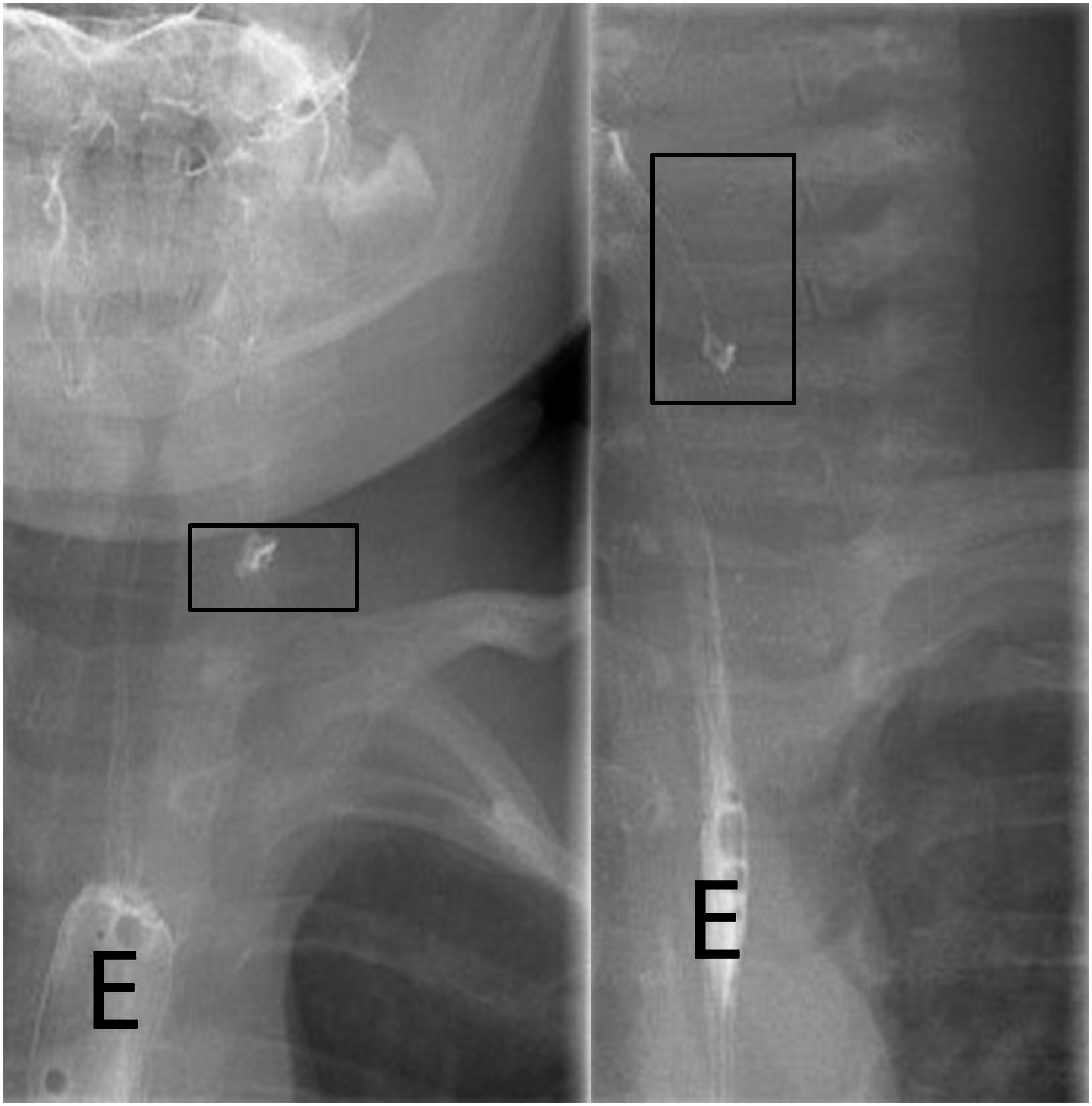
The barium swallow. Box shows the PFST. Letter “E” shows the esophagus. PFSTs, piriform fossa sinus tracts.
Data regarding the patients' demographics, clinical presentations, and treatment before endoscopy, imaging findings, complications, and recurrence were collected and analyzed by using descriptive statistics.
Description of the procedure
With the patient under general anesthesia in dorsal decubitus and neck hyperextension, and under antibiotic prophylaxis with cefazolin, the PFST was explored endoscopically (Olympus® gastroscope GIF-Q165; 9.2 mm outer diameter, 2.8 mm working instrument channel).
First, a continuous airflow infusion (maximum 10 L/minute) was instilled through the flexible endoscope to distend the piriform sinus and facilitate the recognition of the fistula opening.
We used a “Y” connection (Fig. 2) to introduce simultaneously both the airflow and a metallic guide for further cauterization.

Olympus® gastroscope, 9.2 mm outer diameter. The “Y” connection is shown. We introduced the airflow and the metallic guide that we used to do electrocautery.
Second, the guide wire was introduced through the PFST until a stop point could be felt and it could advance no further. The sinus obliteration was then performed using diathermy (Valleylab electrosurgical unit®). The guide wire was then slowly pulled back while applying diathermy, so that the entire tract could be obliterated. An optimal result was considered achieved when the mucosa had an off white appearance (Fig. 3).

Oral feeding was started on the same day of the surgery and discharge was the next day for all patients.
Results
Eight boys (66.6%) and 4 girls (33.3%) with a median age at presentation of 6 years (range: 4 months to 14 years) were included in our study. Their clinical characteristics are summarized in Table 1.
Clinical presentation of the 12 affected children included neck tumor in 7 patients (58%) with neck abscesses in 4 patients (33%), acute thyroiditis in 5 patients (41%), and recurrent suppurative thyroiditis in 1 patient (8%). All lesions occurred on the left side.
All patients underwent both ultrasonography and barium esophagography, 6 (50%) a tomography scan, and 3 (25%) underwent MRI. Barium esophagography was positive in 6 patients (which represents a sensitivity of 50% in our series).
Two patients were treated with ESD after the initial open approach had failed. One of them was a female with acute thyroiditis at presentation who initially underwent an open excision, including partial thyroidectomy; the other patient was a 4-month-old female with a neck tumor, who was initially operated via an open approach without thyroidectomy.
Four patients with neck abscess were treated with antibiotics and drainage to resolve the neck infection 4 weeks before performing the definitive endoscopic treatment.
The mean duration of follow-up was 3.8 years (median [range], 4 [0.2–6] years)
No postoperative complications were reported in any patient. One patient had a recurrence (positive barium study without symptoms), which was again treated endoscopically with success; no more recurrences have been found. The overall success rate of this procedure in our series was 91% with one attempt and 100% with two attempts.
Discussion
The human head and neck develop from the branchial apparatus, which begins differentiation at week 4 of gestation. There are controversies about the anatomy of the PFST. The external opening, if it exists, of both third and fourth remnants arises in the same location: along the anterior border of the junction of the middle and lower part of the sternocleidomastoid muscle; that is why some authors have suggested grouping both as the same entity. Third branchial fistulae are classically described as vestiges of a tract that originates from the base (cranial end) of the piriform fossa. It crosses the thyrohyoid membrane, travels around the hypoglossal nerve, and then loops over the hypoglossal nerve, inferior to the glossopharyngeal nerve, posterior to the internal carotid artery, and anterior to the vagus nerve.1–3,9,10 The tract of fourth branchial arch anomalies originates from the apex (caudal end) of the piriform fossa, by the proximal esophagus, and passes through the cricothyroid membrane below the superior laryngeal nerve. 11 Then it descends parallel to the recurrent laryngeal nerve under the subclavian artery on the right side and under the aortic arch on the left side. There is a strong left-sided predominance of PFST (89% vs. 11% on the right side) 12 ; it could be related to the common absence or involution of the fourth branchial arch on the right side.
The first neck mass caused by a PFST was described by Sandbom and Shafer in 1972. 9 PFSTs are typically observed in children and young adults. These anomalies are rare, accounting between 2% and 8% of all branchial anomalies. 13 PFSTs usually present as recurrent lateral neck abscess (45% of the cases) and suppurative thyroiditis (42%). Other presentations such as retropharyngeal abscess with cellulitis, upper respiratory infections, stridor, and mediastinitis have been reported with less frequency. PFST needs to be suspected in the presence of the described symptoms. Ultrasonography can be helpful in making the diagnosis, and gas around the left upper pole of the thyroid gland is a pathognomonic sign of PFST. 14
Contrast-enhanced computed tomography might be useful; some feel that routine use is not justified, since ultrasonography can provide enough information without patient radiation, before definitive diagnosis is obtained with endoscopic visualization. 13
Barium swallow can be useful in the diagnosis of PFST, with a reported sensitivity of up to 80%. In our series, it was positive in only 6 patients (sensitivity of 50%), so its utility might be limited. It has low sensitivity during the acute infective stage because the inflamed tract presents an obstacle to the passage of barium.14,15
PFSTs are confirmed by endoscopic visualization of the fistula hole, most cases will be left sided. Flexible nasoendoscopy or using of a smaller laryngoscope is an alternative for small patients. 16
Traditional surgery consists of excision of the fistulous tract during a quiescent period via a cervical approach, with or without partial thyroidectomy. Open resection has a described success rate of about 85%, but a reported complication rate of 6% (the most common complication is vocal cord paralysis). Other complications are salivary fistula and infection. 17 These problems are more frequent in young children. 18
When acute suppurative thyroiditis is present, a partial thyroidectomy is recommended by many authors, but the failure rate has been described similar, with or without thyroid lobectomy. 19
Incision and drainage during infection yield a high recurrence rate. Treatment should be preceded by the administration of antibiotics to allow regression of associated infection and inflammation.
An endoscopic approach has become increasingly popular, and could be the initial therapy for PFST as an alternative to open surgery. This treatment has been reported since the late 1990s. This approach can be performed with a gastroscope (as in this report) or via direct pharyngoscopy with a rigid scope. 19 The principle of the endoscopic treatment is to cut the communication between the sinus tract and the upper aerodigestive tract to prevent infection.
Electrocautery is the most commonly reported technique for endoscopic obliteration. There are other techniques such as using trichloroacetic acid 1 with or without previous mucosal ablation, 4 laser 5 (including CO2, diode or thulium laser), silver nitrate, 6 fibrin glue, or a combination of silver nitrate and laser.7,8
Endoscopic techniques are minimally invasive, effective, and safe. The endoscopic approach has a reported success rate of around 92%. Vocal cord paralysis has been reported after cauterization with trichloroacetic acid. This treatment is most often performed as an outpatient surgery, with an early return to normal. 20
Endoscopic cauterization also represents an important option in patients with reappearance of PFST. The success rate in patients with a recurrence after primary open approach is 85.7%. In our series, we performed successful endoscopic obliteration in 1 patient in whom previous open surgery had failed.
Nicoucar et al. 17 published a systematic review in 2010, where they recommended observation for patients who initially responded to antibiotics, and also recommended an open approach only for patients older than 8 years. They reported that it is best to avoid the open approach in younger patients because of the possible complications in that group.
We recommend an endoscopic approach as the first choice for all patients with PFST, due to its safety and high rate of success.
Conclusion
Endoscopic treatment with diathermy of PFST in children has revolutionized the management of this pathology avoiding the complications of the classical open approach.
Endoscopic cauterization of PFST is a safe and effective procedure to treat a newly diagnosed PFST. It can also be considered for treating a recurrence after primary open surgery.
Footnotes
Disclosure Statement
No competing financial interests exist.