
Abstract
Abstract
Background:
Mastering proper force manipulation in minimally invasive surgery can take many hours of practice and training. Improper force control can lead to necrosis, infection, and scarring. A force-sensing skin (FSS) has been developed, which measures forces at the distal end of minimal access surgeries' (MAS) instruments without altering the instrument's structural integrity or the surgical workflow, and acts as a minimally disruptive add-on to any MAS instrument.
Methods:
A proof of concept study was conducted using a FSS-equipped 5 mm straight-tip needle holder. Participants (n = 19: 3 novices, 11 fellows, and 5 staff surgeons) performed one intracorporeal suturing knot task (ISKT). Using participant task video footage, each participant's two puncture forces (each wall of the Penrose drain) and three knot tightening forces were measured. Force metrics from the three expertise groups were compared using analysis of variance (ANOVA) and Tukey's honest significance test with statistical significance assessed at P < .05.
Results:
Preliminary ISKT force metric data showed differences between novices and more experienced fellows and surgeons. Of the five stages of the ISKT evaluated, the first puncture force of the Penrose drain seemed to best reflect the difference in skill among participants. The study demonstrated ISKT knot tightening and puncture force ranges across three expertise levels (novices, surgical fellows, and staff surgeons) of 0.586 to 6.089 newtons (N) and 0.852 to 2.915 N, respectively.
Conclusion:
The investigation of force metrics is important for the implementation of future force feedback systems as it can provide real-time information to surgeons in training and the operating theater.
Introduction
M
Minimal access surgeries (MAS) is a surgical technique using long surgical instruments ranging from 30 to 45 cm in length and 2 to 10 mm in diameter that offers many advantages when compared with open surgery (less postoperative pain and infection, and recovery time), and as a result these techniques have become widely used. 3
Unlike open surgery, MAS lacks direct hand–eye coordination and the fixed incision point prevents translational movement (loss of two degrees of freedom), thus resulting in a decrease in dexterity. The greatest limiting factor of MAS pertains to the reduced access to the surgical site, which ultimately affects the surgeon's ability to sense the forces between the laparoscopic instrument and the tissue. In MAS, the laparoscopic instrument is affected by forces from the trocar, abdominal (or thoracic) wall, and involved tissues. The combination of these forces results in a leveraging (fulcrum) effect that causes the forces experienced at the tool's handle to be 2 to 6 times larger than that of the tool tip. 1 Due to the nature of MAS procedures, unintentionally large forces may be exerted at the surgical site, thus resulting in tissue damage and potentially affecting the short- and long-term outcomes of the patient.
Despite this perceived need, conventional box simulators (including the fundamentals of laparoscopic surgery [FLS] course) focus primarily on a surgeon's precision, speed, and qualitative tissue handling skills with considerably less attention paid to forces exerted directly on tissues.4,5 Recent studies, however, have shown that precision and time parameters alone are unable to fully assess a surgeon's tissue handling skills. As a result, the investigation of the forces exerted during MAS tasks by surgeons of varying experience could help determine whether force measurements can be used as an additional metric to assess surgical skills, incorporating tissue handling in future evaluations. The purpose of this study was to: (1) determine the range of forces exerted during a MAS intracorporeal suture knot task (ISKT) in a box simulator, and (2) to perform a proof of concept study for the classification of surgical expertise using force metrics in a conventional MAS training task and setup.
Methodology
Force-sensing “skin” technology
A novel, thin MAS force-sensing “skin” (FSS) was developed to measure and quantify forces exerted by standard MAS instruments (Fig. 1a). 6 The FSS does not alter the MAS instrument's structural integrity or the surgical workflow, and acts as a minimally disruptive add-on to any MAS instrument. The sleeve is comprised of a polyimide flexible printed circuit (FPC), which spans the majority of the instrument shaft length and adds 0.3 mm of circumferential thickness. The total weight of the FSS is 1.8 g. When adhered, this FPC section surrounds the entire shaft circumference over a short 18 mm length of the instrument. The FSS can be applied to tools between 3 and 10 mm in diameter.
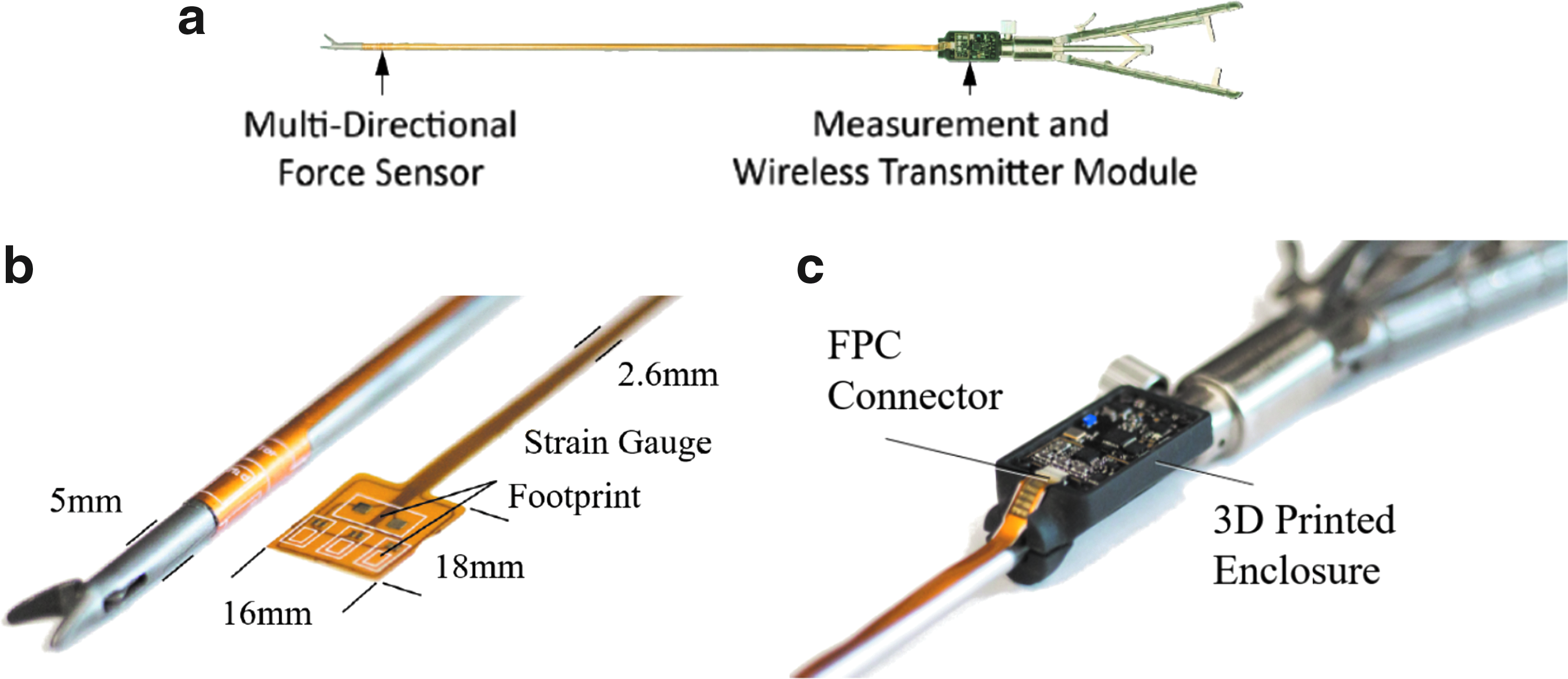
At the distal end of the tool shaft, the FPC can be equipped with up to three linear strain gauges and one torque strain gauge, creating a multidirectional force sensor (Fig. 1b). Mechanical deflections in the MAS instrument's shaft can be measured by these strain gauges and used to calculate the applied force at the distal end of the tool. For the ISKT, axial forces (shaft elongation and compression) are assumed to be negligible and resultant bending forces can be characterized by two linear strain gauges in the FSS.
Strain data from the FSS is transferred in real-time through a Bluetooth transmitter module to a mobile application which logs the data (Figs. 1c and 2). The module (40 mm by 20 mm, 7 g) is located at the proximal end of the tool. In the mobile application, data are stored locally on the mobile device in a comma-separated value file. During a surgical task, a user can manually timestamp points of interest (e.g., suture knot tightening). These timestamps are appended to the logged data and can be accessed during postprocessing.

Screenshots of mobile device application illustrating the home screen (left), user data screen (center), real-time plotting of force data (right).
Participant recruitment
The proof of concept study was conducted during a Pediatric Urology workshop at The Hospital for Sick Children. Participants (n = 19: 3 novices, 11 surgical fellows, and 5 staff surgeons) were recruited with differing levels of experience in MAS. All novices (operating room nurses) were selected based on having no prior surgical or MAS training. All fellows and staff surgeons specialized in Pediatric Urology. All fellows, except 1 had basic pediatric MAS experience (laparoscopic appendectomy or laparoscopic cholecystectomy procedures/year) and 7 fellows had advanced pediatric MAS experience (laparoscopic fundoplication, bariatric laparoscopy, or laparoscopic adrenalectomy procedures/year), refer to Tables 1 and 2 for summary. Nine fellows had at least 1 hour of training inside a box trainer and 6 fellows had training with robotic MAS systems.
Basic pediatric MAS procedures include laparoscopic appendectomy or laparoscopic cholecystectomy. Advanced pediatric MAS procedures include laparoscopic fundoplication, bariatric laparoscopy, or laparoscopic adrenalectomy.
MAS, minimal access surgeries.
Dash lines represent lack of participant response to questionnaire detailing their MAS training history.
MAS, minimal access surgeries.
Study protocol
Participants performed one MAS ISKT using a 5 mm straight-tip needle holder (in the dominant hand) equipped with a FSS. The FSS tool was characterized and the results showed that the system responded linearly to tool-tip forces independent of direction with a Root Mean Square error of 0.088 newtons (N). The ISKT was performed using standard materials: a laparoscopic box-trainer, Penrose drain, and 2-0 suture with a small semicircular needle.
Each ISKT was divided into five stages: two puncture forces (each wall of the Penrose drain) and three knot tightening forces. Participants were told before the task that they would be performing an ISKT. No instructional video was provided, however, the novices who had never performed an ISKT were verbally instructed by a staff surgeon. During the task, video footage was recorded from within the box trainer and instrument forces were logged on a mobile phone. At each stage of the ISKT, a timestamp marking the point of interest was logged within the force data manually by the study coordinator.
Evaluation parameters, such as mm from dot on Penrose, apposition, and avulsion, were determined after each task was completed. Calculation of FLS raw scores for the ISKT was performed poststudy with the assistance of an MAS training center at Toronto Western Hospital. Scores were based on efficiency (time) and precision (number of errors). The ISKT was allocated a cutoff time of 600 seconds. The efficiency score was calculated by subtracting the time of task completion from the cutoff time. Penalties were scored for errors or lack of precision, and the penalty score was subtracted from the efficiency score to yield a final score for the ISKT. Higher scores correspond to higher levels of performance.
FLS penalty scores were given if: (1) the needle was not passed precisely through the target points (sum of the distance in millimeters that suture misses from the target points), (2) the stitch was not tied sufficiently tightly to approximate the edges of the slit and close the defect (sum of the gap in millimeters for where the suture did not properly approximate the edges), (3) if the knot slipped when tested, or (4) if the Penrose drain was avulsed from the Velcro tab.
Each participant completed a follow-up questionnaire on the ease of use of the force-sensing system.
Signal processing and video analysis
To address the issue of high-frequency noise and low-frequency drift, each strain gauge channel is passed through a low-pass filter (96 Hz) and first differencing algorithm. A force model utilizes the processed strain data to determine the magnitude of force applied. The bending force model for a FSS equipped with two strain gauges placed 120° apart is given below:
where E is the Young's Modulus of steel, l is the distance between the strain gauges and the tool-tip, ro and ri are the outer and inner radii of the instrument shaft, respectively, and
Timestamps marked in the logged force data were crossreferenced with participant video footage to determine the peak force of each stage of the ISKT. Video footage was also used to determine the time to completion and number of ratchet clicks performed.
Statistics
Mean force for all five stages of the ISKT from the three expertise groups were compared using analysis of variance (ANOVA) and Tukey's honest significance test with statistical significance assessed at P < .05.
Results
Participants who exceeded the 600 seconds time requirement were allowed to finish the task. Five participants tied more than three suture knots, in these instances only the first three suture knots were used in the force comparisons. Each expertise group's force metrics for the five stages of the ISKT are summarized in Table 3. Mean first puncture force was statistically different between expertise groups (P < .02). The differences in the other force metrics were not significant. Fellows applied lower first puncture forces than novices (P = .02); a similar relationship was observed between staff surgeons and novices (approaching statistical significance with P = .06), but not between fellows and staff (P = .99). The maximum force recorded in the study was a knot tightening force of 6.089 N.
N = newtons.
Accuracy and precision metrics utilized in FLS score calculations are summarized for each participant in Tables 4 and 5. Linear regression between raw FLS scores versus mean puncture force and mean knot tightening force resulted in R2 values of 0.5498 and 0.3230, respectively. A linear regression between the security of knot metric and mean knot tightening force showed no significant association with a R2 value of 0.5880.
Metrics include: (1) mm from dot: sum of the distance in millimeters that suture misses from the target points, (2) apposition: if the edges of Penrose drain were positioned side by side after suturing, (3) avulsion: if the Penrose drain was removed from Velcro tab, and (4) time of completion in seconds.
Higher raw FLS score and lower penalty values indicate higher proficiency. Penalties are given for errors in mm from dot, mm of gap incision (improper apposition), and low security of knot. Tasks requiring over 600 seconds or which avulse the Penrose drain are automatic fails (awarded a raw FLS score of zero).
FLS, fundamentals of laparoscopic surgery.
From the questionnaire, all participants stated that both the FSS and electronics module did not impede or affect their ability to perform the ISKT. Five participants stated that the ratchet mechanism of the Faux Medical needle holders were difficult to disengage.
Discussion
The ISKT was chosen for its complexity and requirement of accurate force control. The ISKT has limits for force exertion intrinsically embedded within the simulated procedure: if the surgeon applies too much upward force, the Penrose drain will avulse and too much force applied to the Penrose drain rather than the suture knot will cause the drain to tear. On the other hand, applying too little force causes the knots to be loose potentially resulting in incomplete apposition.
Novices were expected to exert larger forces than staff surgeons, and fellows were expected to apply forces in between the ranges of the novice and staff surgeon expertise groups. These predictions were based on the assumption that with more years of surgical training, surgeons would learn and develop refined tissue handling skills, which would be reflected in their force application.
In general, the mean forces of the novices were greater than those of the fellows and staff surgeons. However, statistical significance was only found in the first puncture force between novices and fellows, while approaching statistical significance between novices and staff. This may in part be explained by the angle at which the needle tip is placed into the Penrose drain, with angles that are greater than or less than 90° requiring higher forces to puncture the drain; the less experienced participants would likely have less appreciation of the optimal angle of needle entry through the drain and perhaps would be more challenged by determining this angle with a curved needle.
Overall, fellows and staff surgeons did not display a statistical mean difference for each stage in the ISKT. These results could be partially explained by the fact that most of the fellows have had sufficient training and experience in MAS and have begun to approach the force profiles of staff surgeons; data on procedures performed in Table 1 only reflects the participants' experience with pediatric cases; it is possible that some of these participants have had significant adult MAS case experience, which are not accounted for. In addition, the sensitivity of the FSS is another possible reason for the lack of differentiation between the two expertise groups. The FSS may not be sensitive enough to detect the force differences between fellows and staff surgeons.
Fellows and staff were observed to have a larger knot tightening force on the third knot relative to their first two knots. This observation may provide insight into the force profile of the ISKT and how generally the last knot is tightest to secure the suture from slippage.
From this proof of concept study, the absolute minimum and maximum forces across the three experience levels were knot tightening forces of 0.586 and 6.089 N, respectively. In general, puncture forces had a smaller range and found to be less than knot tightening forces having minimum and maximum forces across the three experience levels of 0.852 and 2.915 N, respectively. Peirs et al. found ±2.5 N to be an adequate force range for MAS needle driving tasks.1,7 To investigate these forces, Peirs et al. had a skilled surgeon perform in vivo testing using a 5 mm needle driver equipped with strain gauges and determined the force ranges for differing sutures, needles, and tissues. Differences between prior results and this proof of concept study results may potentially be due to the use of different sutures, different suture needles, different target tissues (biological rat tissue versus synthetic Penrose drain), and the expertise level of the surgeons.
A low linear correlation, R2 value, was found between the raw FLS scores and the mean puncture force, as well as between the raw FLS scores and mean knot tightening force. A trend was observed where higher mean puncture forces resulted in lower FLS scores; however, due to the limited number of participants, this finding cannot be verified. No linear trend was observed between mean knot tightening force and raw FLS score. Since FLS scores combine several metrics, such as (1) completion time, (2) mm from dot, (3) apposition, and (4) security of knot, it is highly possible that instrument force may either not be accounted for within the score or a linear correlation is not present between the scores and instrument force. Past groups have shown that precision and time parameters alone are unable to fully assess a surgeon's tissue handling skills, which could explain the lack of correlation found in these results.4,5
This proof of concept study was able to determine the range of forces exerted during a MAS ISKT in a box simulator. The ranges include those of novices with no MAS experience and extend up to those of staff surgeons. In this small group of participants, it is unclear what the optimal forces should be for each of the five parts of the ISKT; it may be that higher forces are more beneficial for certain actions, such as knot tying, and lower forces are more suited for tasks such as puncturing of the Penrose drain.
Limitations of this proof of concept study include: (1) Limited number of participants. The main limitation of this study is the small sample size potentially reducing the statistical significance found in the results. More participants are required before an accurate determination of the force metrics which correspond to each expertise group can be established. (2) Categorization of expertise level. During the force analysis of the ISKT, participants were placed into groups based on training level and number of procedures performed annually (limited only to pediatric experience and did not include adult MAS procedures). As there is no clear optimal way to determine expertise from participant occupation or history, participants with differing MAS expertise may have been placed in an incorrect category. In addition, participant estimations of number of procedures per year and hours trained in MAS box trainers are approximations, which add uncertainty to the categorization of the participants. Future analysis should define expertise based on an unbiased assessment system which evaluates proficiency using video assessment and/or task performance metrics. 8 (3) Participant specialization. All fellows and staff surgeons specialized in Pediatric Urology and several participants had more experience in robotic surgery than standard MAS. A future study incorporating other specialties (e.g., general surgery) will help remove any potential biasing from occupational specialization. (4) FSS device limitations. The version of the FSS used in this proof of concept study was susceptible to temperature drift, moisture, and contaminants affecting the electronics module. As a result, multiple signal processing techniques were required to remove unwanted noise and artifacts in the signal. Potentially signal characteristics can be inadvertently removed through signal processing along with undesirable noise, leading to a loss of signal data. Future studies will incorporate an improved FSS design, which accounts for these noise-related characteristics, reducing the amount of signal processing required. (5) Participant preference for equipment. Multiple participants complained that the ratcheting mechanism on the needle holders were difficult to disengage and hindered their ability to perform the ISKT. One participant complained about the ease of use of the green nylon suture used to perform the task.
In summary, the FSS is a minimally disruptive add-on, which was capable of measuring forces within a conventional MAS training task using standard tools. Further development of the FSS and evaluation of MAS tasks using a larger sample size of participants are required to establish the role of force metrics in surgical trainee assessment and education. Moreover, a study on MAS forces utilizing a real tissue model will provide insight into the correlation of excessive force exertion and tissue damage. Ultimately, the goal of the FSS is the incorporation of force metrics into future force feedback systems to provide real-time information to surgeons in training and the operating theater.
Footnotes
Disclosure Statement
No competing financial interests exist.