
Abstract
Abstract
Introduction:
The vertical transumbilical incision (TU) technique during neonatal abdominal exploration involves dissection and ligation of umbilical vessels, which allow access to all quadrants of the abdomen and complete bowel evisceration with minimal violation to the anterior abdominal wall. We compared patient characteristics and outcomes for neonates undergoing TU with standard transverse exploration.
Materials and Methods:
A single-center retrospective review of neonates who underwent abdominal exploration between January 2010 and September 2015 was conducted after obtaining Institutional Review Board approval. Data included patient demographics, indication for operative intervention, operative details, complications, including incisional hernias, and long-term outcomes.
Results:
There were 88 neonates under 4 months of age who underwent abdominal exploration, with a median age of 5.5 ± 17 days and a median gestational age of 32.8 ± 16 weeks. Exploration was emergent in 38 patients (43%) and 49 (56%) required ostomy formation. A transverse incision (TV) was used in 30 patients and a TU in 58 patients. Both groups had similar postoperative complication rates; 27 (47%) in the TU group and 11 (36%) in the TV group, P = .51. Median length of follow-up in the TU group was 5.1 ± 18 months and 6.2 ± 16 months in the TV group, P = .48. The TU group had 4 incisional/umbilical hernias (7%), none have required repair.
Conclusion:
TUs for abdominal explorations in neonates have similar outcomes as the standard TV while preserving the integrity of the anterior abdominal wall.
Introduction
H
Materials and Methods
After obtaining Institutional Review Board approval, data were collected on neonates who underwent abdominal exploration from January 2010 to September 2015. Data included patient demographics, indication for operative intervention, operative details, complications, including incisional hernias, and long-term outcomes. Descriptive and comparative analysis was performed. Means are expressed as ± standard deviation and median values as ± interquartile range. Comparative data were analyzed using Student's t-test for two-group comparisons or Mann-Whitney U test, where appropriate, for continuous variables. Chi-square test with Yates' correction, or Fisher's exact test where appropriate, was used for discrete variables.
Neonates were defined as infants up to 4 months of age, regardless of gestational age at birth. TVs were those that created a horizontal incision traversing at least one rectus sheath, whereas transumbilical incisions (TUs) included those that involved dissection and ligation of umbilical vessels, and vertical fascial incision in addition to a vertical extension of the skin incision, allowing for complete bowel evisceration.
Results
There were 88 neonates under 4 months of age who underwent abdominal exploration, with a median age of 5.5 ± 17 days and a median gestational age of 32.8 ± 16 weeks. Exploration was emergent in 38 patients (43%) and 49 (56%) required ostomy formation. Procedures included 11 (13%) diagnostic laparoscopies converted to 10 TUs and 1 TV open exploration. Surgical interventions included bowel resections, duodenoduodenostomies, lysis of adhesions, meconium pseudocyst resections, Ladd's procedures, and reduction of volvulus.
A TV was used in 30 patients and a TU in 58 patients. Demographic data were comparable in both groups, as were operative duration and number of patients requiring ostomy formation (Table 1). Both groups had similar postoperative complication rates; 27 (47%) in the TU group and 11 (36%) in the TV group, P = .51 (Table 2). Of these, 17 (29%) in the TU group and 8 (27%) in the TV group required reoperation, P = .99. These complications included bowel obstructions, anastomotic strictures, hematomas, superficial wound dehiscence, wound infections, short gut syndrome, ostomy prolapse, and death. Time to full enteral feeds in those able to meet full feeds was similar in both groups with the TV group achieving full enteral feeds in 28 ± 23 days and the TU group achieving full enteral feeds in 22 ± 17 days, P = .5.
IQR, interquartile range; SD, standard deviation; TU, transumbilical incision; TV, transverse incision.
IQR, interquartile range; TU, transumbilical incision; TV, transverse incision.
Median length of follow-up in the TU group was 5.1 ± 18 months and 6.2 ± 16 months in the TV group, P = .48. The TU group had 4 incisional/umbilical hernias (7%) and the TV group had none, P = .29. Two of these incisional/umbilical hernias closed spontaneously before 3 years of age, 1 was closed at the time of stoma takedown, and the other did not return for follow-up after the initial postoperative clinic visit (Table 3).
Discussion
Neonatal surgical exploration has historically been achieved using a TV abdominal incision with reported advantages, including excellent exposure, greater tensile strength, and importantly a lower rate of wound dehiscence than a midline vertical incision.1,2,10 A circumumbilical incision was first described in 1986 as an approach for pyloromyotomy 4 and has since been used for other disease processes requiring exploration.5–8,11–13 Contemporary studies support the safety and feasibility of a TU approach.14–16
The recent focus on postoperative cosmesis has led investigators to evaluate laparoscopy versus open operations and even single-incision laparoscopy compared with traditional laparoscopy in an effort to achieve ever-improving cosmesis. 17 Laparoscopy has recently gained more widespread use in neonates as well. 18 The TU results in an almost hidden scar comparable with laparoscopy, and the argument has been made that this is a method to achieve improved cosmesis compared with traditional transverse laparotomy, with similar safety and efficacy.11,14 The shift in operative approach for some surgeons in our institution provided the opportunity to investigate this in a large cohort of patients. This study represents an evaluation of TU compared with TV laparotomies in the contemporary setting.
The circumumbilical or transumbilical approach described in the literature includes periumbilical skin incisions in either the supra- or infraumbilical region, sometimes with omega-shaped extensions or 350° extensions with a skin bridge.5–9,11–16 In terms of the fascial incision, studies have included transverse fascial incisions with or without inclusion of the rectus muscle,8,15 vertical midline fascial incisions,5,6,9,11,12,14,16 or both. 7 Our approach differs slightly, in that it includes a vertical transumbilical skin incision with vertical extension as needed, dissection and ligation of umbilical vessels, and a midline fascial incision as well. This allows for access to all quadrants of the abdomen and complete bowel evisceration with minimal violation to the anterior abdominal wall and an excellent cosmetic outcome (Fig. 1).
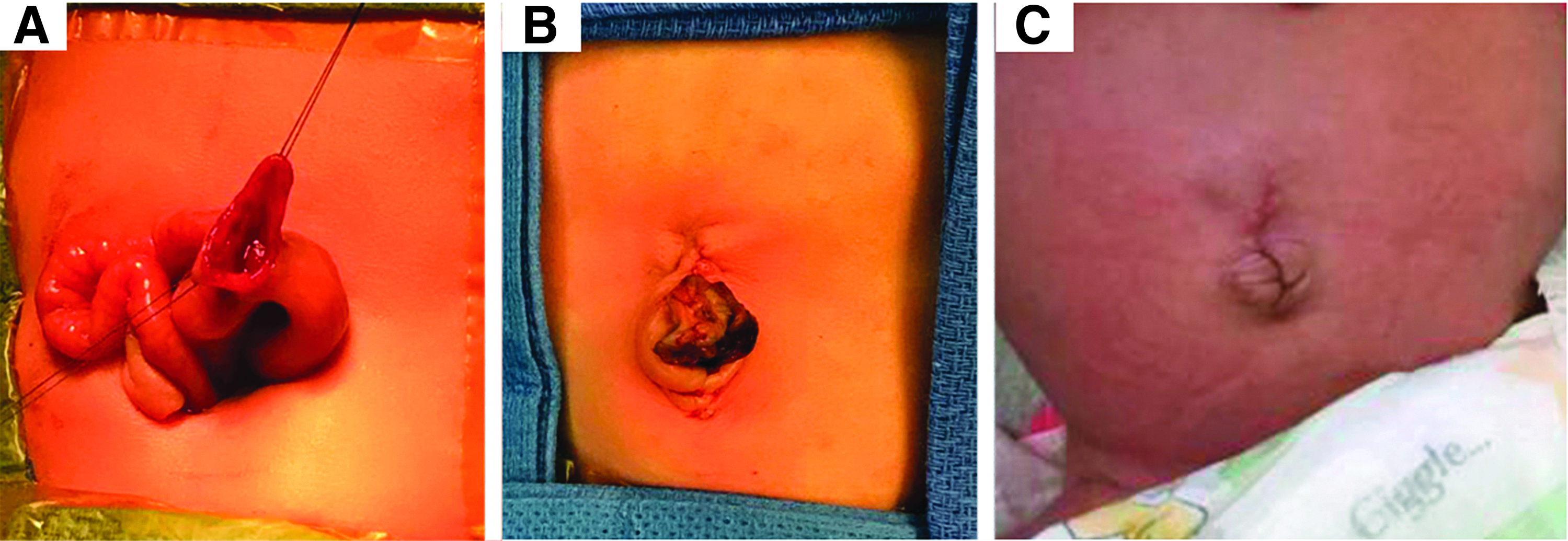
Transumbilical approach to abdominal exploration for bowel obstruction, with resection of jejunal web.
There was no difference in operative time between the two techniques of accessing the abdomen, which has been shown previously, 14 and may indicate the comparable ease of access to all quadrants of the abdomen. This is contrary to historical arguments favoring the TV for reasons of improved exposure related to the shape of the neonatal abdomen. 1
The good exposure of this technique is also supported by the wide variety of pathologies that can be addressed using a TU incision. In our study, we used the TU approach to perform bowel resections for multiple reasons, including atresias, internal hernias, necrotizing enterocolitis, and bowel obstructions. We also performed duodenoduodenostomies for atresia, lysis of adhesions, meconium pseudocyst resections, Ladd's procedures, and reduction of midgut volvulus. Other studies have supported the versatility of the TU approach, reporting its use for duodenal and jejunal atresias, Hirschsprung disease, intestinal duplications, ovarian pathology, and more.5–8,11,12,14,16
Two studies comparing the TU with the TV approach have been reported.14,15 whereas the majority of the literature reporting on the TU approach is in the form of retrospective case reviews. Our large retrospective cohort comparison therefore adds substantially to the literature. Additionally, our study also included neonates requiring emergent intervention with around 40% of both groups undergoing emergency surgery, with a similar rate of complications, similar rate of reoperation, and similar rate of ostomy formation in both groups, again demonstrating the versatility and efficacy of the TU approach. This is the first study to include hemodynamically unstable patients and those with evidence of peritonitis, bowel perforation, or bowel ischemia. This kind of study population was excluded in previous comparative studies.14,15 The ability to use the TU approach in unstable patients provides an advantage over laparoscopy, but maintains an excellent cosmetic outcome.
Another historical concern regarding vertical incisions in neonates was the decreased tensile strength of these incisions, including concerns for increased rates of incisional herniae and fascial dehisence1,10; however, our study shows a low incisional hernia rate in both groups and no incidence of fascial dehiscence. The TU group did have a higher rate of incisional herniae at the umbilicus with 4 patients (7%) presenting with postop hernias compared with none in the TV group; however, this was not statistically significant. More importantly, this finding was not clinically significant because 2 of these herniae closed spontaneously and 1 was closed at the time of stoma takedown using the same TU approach. One child with a hernia was lost to follow-up. Tsuji et al. did not report on the hernia rate in their study. 14 Suri and Langer did find an increased hernia rate in the TU approach, but all resolved spontaneously, whereas 33% in the TV approach required surgical intervention. 15
A major limitation of this study is its retrospective nature and relatively short length of follow-up considering a neonatal population. Additionally, there are no patient-specific factors evaluated or used to determine which patients had the TU versus the TV approach. However, since there has been a practice change in our department, with the majority of surgeons using the TU approach primarily and only some using the TV approach primarily, either approach is used for a variety of patient presentations and is primarily dependent on which surgeon is on call when the patient requires an operation, thereby controlling for patient selection.
This large comparative cohort demonstrates that in neonates requiring abdominal exploration, the transumbilical approach can be performed safely and effectively for both emergent and nonemergent settings, without an increased risk of complications.
Footnotes
Disclosure Statement
The authors have no conflicts of interest to disclose.