
Abstract
Abstract
Objective:
This study aimed to evaluate the safety, feasibility, and prognosis of three different types of minimally invasive procedures for treating gastric gastrointestinal stromal tumors (GISTs) ≤5 cm.
Materials and Methods:
The clinical data, perioperative conditions, and the follow-up results of patients who underwent laparoscopic resection (LAP), laparoscopic and endoscopic cooperative surgery (LECS), or endoscopic submucosal dissection (ESD) for gastric GISTs ≤5 cm were retrospectively collected and analyzed.
Results:
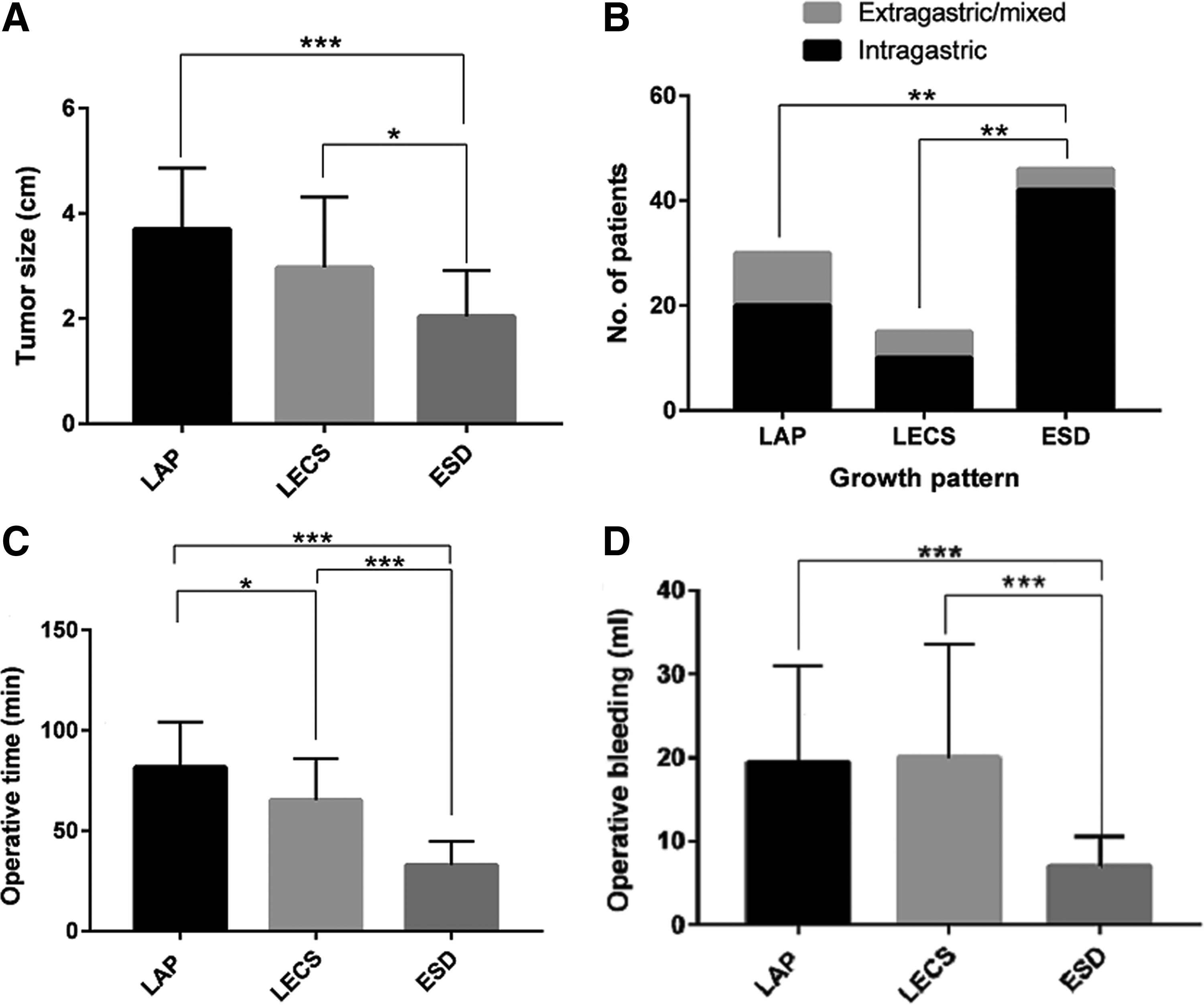
A total of 91 patients were enrolled in this study, and the number of cases who underwent LAP, LECS, and ESD was 30, 15, and 46, respectively. Compared with patients in the LAP and LECS group, patients in the ESD group had a smaller tumor size (P < .001, <.05, respectively.) and a higher percentage of intragastric growth pattern (all P value <.01). Significant differences were found in operative time and intraoperative blood loss among the three groups (P < .001). The operative time and intraoperative blood loss in ESD group were significantly less than that in LECS and LAP groups. No statistical difference was found in the postoperative recovery and complications among the three groups, such as nasogastric tube retention, anal exhaust time, oral intake, postoperative complication, and tumor recurrence.
Conclusions:
Minimally invasive surgery for gastric GISTs ≤5 cm is safe and feasible. The final choice regarding a minimally invasive approach should be based on the tumor size, tumor location, pattern of tumor growth, and experience of laparoscopic surgeons.
Introduction
G
To date, surgical resection with a free margin is the gold standard for primary localized GIST.3,4 Currently, minimally invasive technology has gained widespread application, and its feasibility and safety have been reported.5–11 Various types of minimally invasive procedures, such as endoscopic submucosal dissection (ESD), laparoscopic resection (LAP), and laparoscopic and endoscopic cooperative surgery (LECS), have been performed for gastric GISTs. Recent studies have certified that in GIST patients with tumor not larger than 5 cm, minimally invasive procedure is safe and feasible. However, few studies have compared the clinicopathological characteristics and oncological outcomes of different types of minimally invasive surgery for gastric GISTs ≤5 cm. Hence, in our study, we retrospectively compared the general information, perioperative condition, and oncological outcomes of 91 patients who underwent three different minimally invasive procedures for gastric GISTs ≤5 cm in West China Hospital of Sichuan University from December 2007 to March 2015. We aimed to determine the optimal approach for patients with gastric GIST ≤5 cm by differentiating the three approaches in a Chinese population.
Materials and Methods
Patient selection
Patients who underwent surgical resection for gastric GIST ≤5 cm at West China Hospital of Sichuan University from December 2007 to March 2015 were retrospectively reviewed. Eligible patients met the following criteria: patients with tumor ≤5 cm based on the preoperative endoscopic ultrasonography (EUS) and/or computerized tomography (CT) examinations; aged 18–75 years; diagnosis of gastric GISTs confirmed by postoperative pathological and immunohistochemical analyses; and patients who underwent LAP, LECS, or ESD. Patients with the following conditions were excluded: pregnant or nursing women; patients with severe diseases of other systems or coexistence of any other malignancies; patients with unresectable metastases or recurrent GIST; and patients who underwent concomitant organ resection. Subsequently, 91 patients were included in this study. This study was approved by the Institutional Review Board of the West China Hospital of Sichuan University, and informed consents were obtained from each patient in this cohort. Among patients in this study, 30 patients underwent LAP resection for gastric GIST, 15 patients underwent LECS, and 46 patients received ESD.
Surgical procedures
All operations were performed by skilled endoscopic specialists and specialists with extensive experience in laparoscopic technique in West China Hospital, Sichuan University. Three procedures were available for patients with tumor ≤5 cm and included LAP, LECS, and ESD.
Laparoscopic surgery
After the induction of general anesthesia, the patient was placed in the reverse Trendelenburg and supine position. The surgeon stood on the patient's right side. The first assistant was positioned on the patient's left side. The laparoscopist was between the patient's extended legs. First, an umbilical trocar (10 mm) as a camera port using an open technique was inserted. CO2 pneumoperitoneum was established with an insufflation pressure of 15 mmHg. Four additional ports (three 5 mm ports and one 12 mm port) were inserted into the left upper, left lower, right upper, and right lower quadrants. Before the resection, an overall laparoscopic abdominal examination was carried out to detect the tumor location and size and eliminate tumor disseminations and metastases. Different approaches can be chosen according to the size and location of the tumor. Wedge resections could be performed with laparoscopic stapling devices for tumors within the anterior or posterior walls of the stomach. Proximal or distal gastrectomy was conducted for GISTs that were too close to the cardia or fundus of the stomach because gastric motility may be affected by a wedge resection in that location. Care was taken to make sure that a negative margin was achieved. To reduce the risk of iatrogenic spreading, resected specimens were placed into an endoscopic retrieval bag and extracted through the umbilical wound.
Laparoscopic and endoscopic cooperative surgery
This newly developed LECS-related procedure was widely used for the dissection of intraluminal protruding lesions. The patient position and port setting were placed in the same way as in the LAP group. The tumor was positioned and turned over toward the abdominal cavity by endoscopy. As a result, the tumor location was confirmed by laparoscopic image through the light sent from endoscopy. The direct incision of the mucosal and submucosal layers around the tumor was performed using the ESD technique. A laparoscopic stapling device was used to dissect the seromuscular layer of the tumor and close the incision line, and a sufficient margin could be ensured by endoscopy.
Endoscopic submucosal dissection
ESD was mainly used for the resection of submucosal tumors, especially for intragastric tumors. Before the operation, EUS was performed to determine the tumor size, margins, and the layer of origin. On finding the tumor, methylene blue-stained saline containing epinephrine (1:100,000) was injected into the submucosa to lift the lesion off the muscle layer. A hook knife, a needle knife, an insulated-tip knife, a polypectomy snare tip, and grasping forceps were used for complete tumor resection. An electrocautery snare was used in some cases to promote blood clotting. Endoscopic treatment was considered a complete resection when no residual tumor was visible microscopically on endoscopy.
Data collection and postoperative follow-up
All data were retrospectively recorded from their medical records, including demographic and clinicopathological characteristics, operative data (procedures, operative times, intraoperative blood loss, and complications), and postoperative recovery (anal exhaust time, time of nasogastric tube retention, time of oral intake, postoperative hospitalization days, and postoperative complications). Moreover, telephone or outpatient follow-ups were consecutively conducted. During the follow-up, data collection included postoperative adjuvant therapy with imatinib mesylate, tumor recurrence or metastasis, and death.
Statistical analyses
Statistical analyses were calculated using SPSS for Windows version 19.0 to compare the differences among the three groups. Quantitative results are expressed as mean ± standard deviation. One-way analysis of variance was used to assess significant differences in continuous variables among the three groups. Least significant difference (LSD) method was used to put up multiple comparisons if the variances were homogenous; otherwise, Dunnett's T3 method was conducted. Dichotomous variables were expressed as percentages. Categorical data from three groups were compared using the χ2 test or Fisher's exact test. A P value of <.05 was considered statistically significant.
Result
Demographic and clinicopathological characteristics
Table 1 summarizes the demographic and clinicopathological features of the patients. Among the 91 patients, 42 were male and 49 were female, with the average age of 57.59 ± 10.72 years (range, 33–78 years). The most common clinical presentation was abdominal discomfort and alimentary tract bleeding. Approximately 30% of the patients were symptomatic. The average tumor size was 2.74 ± 1.29 cm, and 96.7% and 97.8% of the patients were CD117 and DOG1, respectively. More than 50% of the patients exhibited tumors located at the proximal one-third of the stomach, and 80% of the patients were at very low or low risk according to National Institutes of Health (NIH) risk classification. Compared with patients in the LAP or LECS group, patients in the ESD group had smaller tumor sizes (P < .001, <.05, respectively) and had higher percentages of intragastric growth patterns (both P value <.01), the results are shown in Figure 1. However, no significant difference occurred in the age, gender, tumor location, clinical presentation, mitotic count, and NIH risk classification among the three groups, as shown in Table 2.
Multiple comparisons were conducted in variables that were statistically significant difference among the three groups:
CD117, CD117 protein; CD34, CD34 protein; DOG1, DOG1 protein; HPF, high-power field; LAP, laparoscopic resection; NIH, National Institutes of Health; SD, standard deviation.
ESD, endoscopic submucosal dissection; HPF, high-power field; LAP, laparoscopic resection, LECS, laparoscopic and endoscopic cooperative surgery; NIH, National Institutes of Health; SD, standard deviation.
Perioperative information and postoperative complications
A total of 91 patients underwent minimally invasive surgery of gastric GISTs. LAP resection was performed in 30 cases, LECS was performed in 15 cases, and ESD was performed in 46 cases. Among the patients who underwent LAP or LECS, one case underwent proximal gastrectomy, one case underwent distal gastrectomy, and other patients underwent wedge resection. All operations were successful and had no tumor rupture and conversion to open surgery. Significant differences were found in operative time among the three groups (P < .001). The operative time in ESD group was significantly shorter than that in LECS and LAP groups. Patients who underwent ESD had significantly less intraoperative blood loss compared with the patients who underwent LAP and LECS (P < .01), and the results are shown in Figure 1. No statistical difference was found in nasogastric tube retention, anal exhaust time, oral intake, and postoperative hospital stay among the three groups. A total of 12 patients in our study had postoperative complications. The most common complications were pulmonary infection, postoperative bleeding, perforation, wound infection, intestinal obstruction, and severe sour regurgitation. No significant difference was found in postoperative complications among the three groups, as shown in Table 3. All patients with postoperative complications recovered after given symptomatic relief and supportive treatments, and none of the patients required reoperation.
ESD, endoscopic submucosal dissection; LAP, laparoscopic resection, LECS, laparoscopic and endoscopic cooperative surgery; SD, standard deviation.
Tumor-related outcomes
Follow-ups were achieved in 84 patients, with the median follow-up time of 69.5 months (range, 12–100 months). Eighty-three (98.8%) patients were disease free, one patient with high risk in the LAP group had tumor recurrence at 23 months after resection. No death was noted during the follow-ups. Among the 84 patients, 6 patients were given imatinib therapy: 4 cases in the LAP group, 1 case in the LECS group, and 1 case in the ESD group. There was no statistically significant difference in the proportion of patients who received imatinib therapy among the three groups (P > .05). The main toxic reactions for imatinib were palpebral edema, nausea, and leukopenia, which were well tolerated by patients.
Discussion
GISTs are relatively rare mesenchymal tumors of the gastrointestinal tract. The annual incidence of GIST is ∼10–15 cases per million. 12 They are derived from the interstitial Cajal cells or their precursor cells and characterized by gain-of-function mutations in the tyrosine kinase and platelet-derived growth factor alpha genes.13,14 All GISTs are potentially malignant. The malignancy is mostly associated with tumor size and mitotic activity.15,16 However, metastasis and/or recurrence can be observed in most GISTs, even in small GISTs (< 2 cm) or GISTs with low mitotic counts. The molecule-targeted drug imatinib has remarkably improved the long-term outcomes of GIST patients; however, surgery with a negative margin remains the standard initial treatment for nonmetastatic GISTs. Most GISTs are localized within a distinct boundary to the normal tissue and rarely metastasize to lymph nodes. Hence, a wide resection combined with systemic lymphadenectomy is not necessary. Local excision, including a wedge resection, can be achieved in the majority of GIST cases.
With the rapid development of minimally invasive surgeries, more surgical procedures, including LAP, endoscopic resection, and combined laparoscopic and endoscopic approaches, can be chosen for localized GISTs. In 1992, Lukaszczyk and Preletz 17 first reported a successful LAP of gastric GIST. Numerous retrospective studies with small samples have confirmed that minimally invasive surgery is safe and feasible.5,6,11,18,19 Compared with open surgery, minimally invasive surgery has better advantages in operative time, intraoperative blood loss, and postoperative recovery. In our study, the operation time of 91 patients was 54.35 ± 28.30 minutes. The intraoperative blood loss was 13.25 ± 10.88 mL. The nasogastric tube retention time was 2.24 ± 1.75 day/second. The anal exhaust time was 2.48 ± 1.10 day. The postoperative hospital stay was 6.14 ± 2.45 days. These data were consistent with those of previous studies, thereby reconfirming the safety and feasibility of minimally invasive surgeries.
To our knowledge, publications have reported the advantages of minimally invasive approaches by comparing them with open surgery. However, a few have focused on the safety, feasibility, and outcomes among different types of minimally invasive approaches. In our study, all 91 patients who underwent minimally invasive surgeries were divided into LAP, LECS, and ESD groups. Compared with patients in the LAP and LECS group, patients in the ESD group had smaller tumor sizes and a higher percentage of intragastric growth patterns. Moreover, significant differences were found in operative time and intraoperative blood loss among the three groups (P < .001). The operative time and intraoperative blood loss in ESD group were significantly shorter than that in LECS and LAP groups. These results suggest that ESD is a safe procedure with good surgical outcomes for small and intragastric GISTs. However, no statistical difference was found in the postoperative recovery and complications among the three groups. These data indicated that the choice of operative procedure, for GIST patients, that is considered for minimally invasive resection should be based on tumor size, tumor location, tumor growth pattern, laparoscopic surgeon's experience, patient's wishes, and other factors.
Debates exist regarding the standard size for minimally invasive surgery of GISTs. In 2005, the National Comprehensive Cancer Network (NCCN) and the European Society of Medical Oncology recommended that LAP may be acceptable for tumors <2 cm.20,21 However, the tumor size was modified to smaller than 5 cm by the 2007 guidelines. The guidelines of the NCCN in 2010 suggested that a laparoscopic or laparoscopic hand-assisted approach could be considered for gastric GISTs larger than 5 cm. 22 However, many scholars proposed that tumors with large diameters may cause intraoperative iatrogenic ruptures during laparoscopic procedures. Tumor rupture is considered to be a high-risk factor of postoperative recurrence, but few researchers hold different opinions. Nakamori et al. 23 suggested that the LAP of medium-sized gastric GISTs was safe and feasible. Ronellenfitsch et al. 24 also reported the feasibility of tumors larger than 10 cm. Minimally invasive surgery for tumors ≥5 cm can be taken into account after careful discussion. Hence, we considered tumor diameter to not be the decisive factor for minimally invasive treatments.
The influence of minimally invasive surgery on oncological outcome has been controversial.25,26 In our study, all operations were successfully performed because no tumor rupture and conversion to open surgery occurred. In terms of postoperative complications, ESD is associated with a high rate of postoperative bleeding and perforation. However, no statistical difference was found in the postoperative complications among the three groups. Moreover, among 91 patients, only one patient was at high risk in the LAP group and experienced tumor metastasis or recurrence, and 98.8% of patients were disease free, thereby certifying the favorable outcome of minimally invasive resection, with a follow-up of 12–100 months (median, 69.5 months).
LECS, as an emerging minimally invasive approach, shows the positive value in treating gastric GISTs.8,27 LECS can realize accurate and rapid position using a gastroscope and could minimize normal gastric tissue resection, reduce stomach deformation, and guarantee complete tumor resection. LECS is mostly applied for tumors that are intraluminal and those that are close to the cardia or pylorus. These tumor locations indicated a difficult complete resection using traditional laparoscopic procedures. Hiki et al. 28 reported that compared with traditional laparoscopic surgery, LECS has significant advantages in operative time, intraoperative blood loss, postoperative recovery, and complications. In this study, the operation time was significantly shorter (P < .05) in the LECS group than that in the LAP group. However, the estimated blood loss, nasogastric tube retention, complications, and long-term outcomes were not significant between the two groups. Therefore, further study by multicenter and prospective randomized controlled trials should be done to verify the benefits of minimally invasive procedures.
In conclusion, we confirm the safety and feasibility of minimally invasive procedure for gastric GISTs, especially for the tumors smaller than 5 cm. By comparing the three types of minimally invasive surgery, we suggest that for tumors with size not larger than 5 cm, LAP can be considered. Endoscopic resection could be better used in elderly patients or patients with small-sized, intragastric tumors. LECS, as an emerging produce, can realize the position of the tumor more accurately and rapidly compared with classical laparoscopic surgery. LECS could be used in intraluminal tumors and those that are located at the esophagogastric junction or near the pylorus, in which a complete resection using the classical laparoscopic approach would be difficult. However, the final decision for every case should be based on tumor size, tumor location, tumor growth pattern, and laparoscopic surgeon experience.
Footnotes
Acknowledgment
The authors gratefully acknowledge the whole staff of the Department of Gastrointestinal Surgery and pathology, West China Hospital, who generously provided assistance in the collection of data throughout the duration of the study.
Disclosure Statement
No competing financial interests exist.