
Abstract
Abstract
Background:
Pediatric robot-assisted surgery is increasingly being performed, but it is difficult to perform this procedure in infants. A pediatric thoracoscopic model of a 1-year-old patient was developed in our previous study, and this model was used to evaluate the use of a surgical robot for infant surgery.
Methods:
Eight pediatric surgeons performed an intracorporeal suturing and knot-tying task using the da Vinci Xi Robotic Surgical System. The task completion time, number of needle manipulations, and force applied during suturing of the robot-assisted thoracoscopic surgery (RATS) group were compared with those of the video-assisted thoracoscopic surgery (VATS) group whose data had been collected from the same 8 surgeons in our previous study.
Results:
The RATS group showed a significantly shorter completion time than the VATS group in the knot-tying phase (P = .016) and in the total phase (P = .0078). The RATS group showed a significantly smaller number of manipulations than the VATS group in the total phase (P = .039). The RATS group showed a significantly smaller pushing force index than the VATS group in the suturing phase (P = .031), knot-tying phase (P = .031), and in the total phase (P = .031). A seventh rib in the model was dislocated in all RATS group cases.
Conclusions:
The da Vinci Surgical System might be useful in infants because of fast movement and small pushing force. However, the robotic 8 mm instruments were too large for use in the thoracic cavity of the 1-year-old infant.
Introduction
P
In our previous study, a pediatric thoracic model of a 1-year-old infant was developed and its construct validity as a simulator was proven by a skills assessment experiment in which we recruited surgeons with various levels of experience.10–12 The pediatric thoracic model was more useful than a conventional box trainer to distinguish skilled pediatric surgeons. This was because the simulator replicated the anatomy and the difficulties associated with pediatric thoracoscopic tasks more accurately than the conventional box trainer. In this study, pediatric thoracoscopic suturing using the da Vinci Xi Robotic Surgical System was compared with conventional manual thoracoscopic suturing using the pediatric thoracic model, and the advantages and disadvantages of pediatric RATS are discussed.
Materials and Methods
The protocol of this study was approved by the Ethical Committee of the Graduate School of Medicine and Faculty of Medicine, The University of Tokyo (No. 10033). A detailed explanation of the study was provided to the participants before the experiment, and written informed consent was obtained from all participants.
Pediatric thoracic model
We used the rapid-prototyped pediatric thoracic model of a 1-year-old patient that was used in our previous studies.10–12 The thoracic rib cage was segmented from the computed tomographic data of a 1-year-old infant and fabricated by 3D rapid prototyping, and thereafter covered by a skin sheet. A suture pad with force-sensing capability (Suture Evaluation Simulator M57; Kyoto Kagaku Co., Kyoto, Japan)13,14 was placed in front of the third thoracic vertebra to simulate the thoracoscopic repair of tracheoesophageal fistula type C. The model was arranged in the left hemidecubitus position.
Robot-assisted thoracoscopic surgery
Eight pediatric surgeons who had no experience in performing robot-assisted surgery were recruited for this study. First, the participants practiced robotic surgery using the virtual reality simulator15,16 for the da Vinci Si or Xi until they obtained scores of >80 in the three drills, namely “Thread the Rings,” “Energy Switching 1,” and “Suture Sponge 1.” Then, they practiced robotic suturing in a box simulator for 5 minutes and then in the pediatric thoracic model for 5 minutes using the da Vinci Xi.
After practicing manipulation of the da Vinci Xi, the participant was asked to perform one suture and three knot tying tasks at the location of the open cut in the suture pad, and the thoracoscopic view and force-sensing data were recorded. At the beginning of the experiment, the surgical robotic instruments were positioned in three trocars inserted in the seventh intercostal space while keeping a sufficient gap between each trocar and the target (Fig. 1a–c). An 8 mm and 0° direct-viewing thoracoscope was mounted on the robot. Two large needle drivers were used as the right and left instruments. A 5-0 PDS II suture with a 13 mm, 3/8 circle needle (Z126H; Ethicon Endo-Surgery, Cincinnati, OH) whose thread had been cut at 100 mm was placed on the suture pad at the beginning of the experiment. If the participant failed to finish the task, he or she was instructed to restart the task from the beginning.
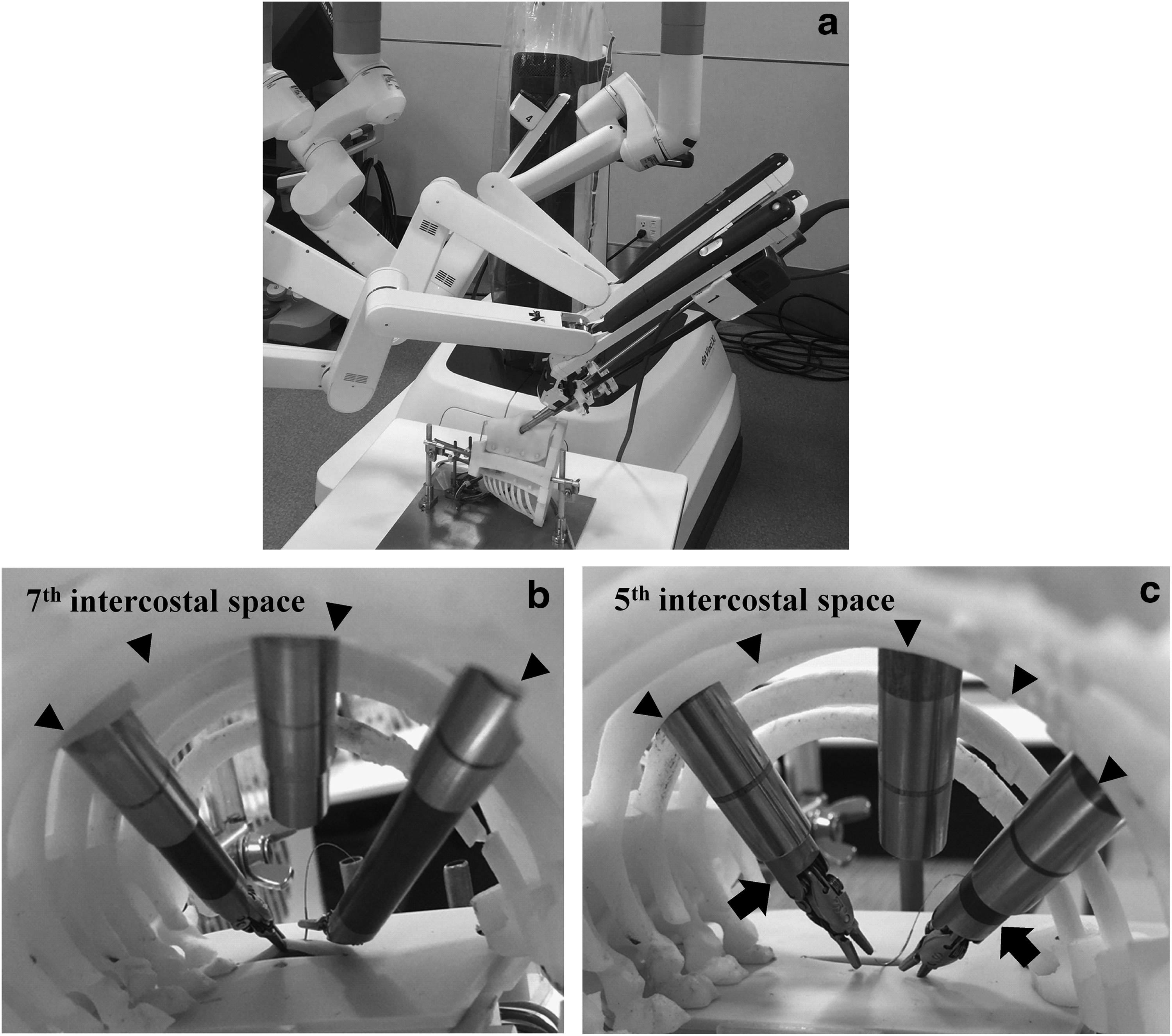
The robot experiment using the pediatric thoracic model.
The data of RATS suturing by the 8 surgeons in this study were compared with the data of video-assisted thoracoscopic surgery (VATS) suturing that had been performed by the same 8 surgeons from our previous study 12 ∼1 year before the RATS suturing experiment. In the previous study, 12 the participants had performed intracorporeal suturing mimicking tracheoesophageal fistula repair in the VATS setting using a 5-mm 30° endoscope, a 3 mm needle driver, and a 3 mm forceps.
Assessment of suturing performance
The task completion time and the number of needle manipulations were manually measured from the recorded videos. The number of needle manipulations was increased by one point for each grasping of a thread or needle.17,18 Each task was divided into the suturing and knot-tying phases. The definition of the start of the knot-tying phase was when the thread was grasped after the needle was totally pulled out from the suture pad. The total phase consisted of the suturing and knot-tying phases.
Deformations of the sponges placed under the suture pad were due to the force applied by the needle and surgical instruments, and they were detected by the photointerrupters surrounding the sponges. The sum of the absolute displacements during each task detected by each sensor was measured. Three force indexes were defined as follows: (1) pushing force index: the sum of the absolute displacements in the vertical pushing direction detected by the bottom sensor; (2) pulling force index: the sum of the absolute displacements in the vertical pulling direction detected by the bottom sensor in only the pulling direction; and (3) the sum of the absolute displacements in the lateral directions detected by the sidewall sensors. A small force index indicates gentle manipulation.
The results between the RATS group and the VATS group were compared using the Wilcoxon signed-rank test. All statistical analyses were performed using JMP Pro 11 (SAS Institute, Inc., Cary, NC). A P value < .05 was deemed as statistically significant.
Results
Comparison of suturing performance
In the following, the data are expressed as median values (interquartile ranges). The task completion times are shown in Figure 2. The RATS group showed a significantly shorter completion time than the VATS group in the knot-tying phase [96 (31) seconds versus 145 (48) seconds, P = .016] and in the total phase [152 (37) seconds versus 203 (64) seconds, P = .0078]; however, no statistically significant difference was observed in the suturing phase [46 (18) seconds versus 59 (15) seconds, P = .23].
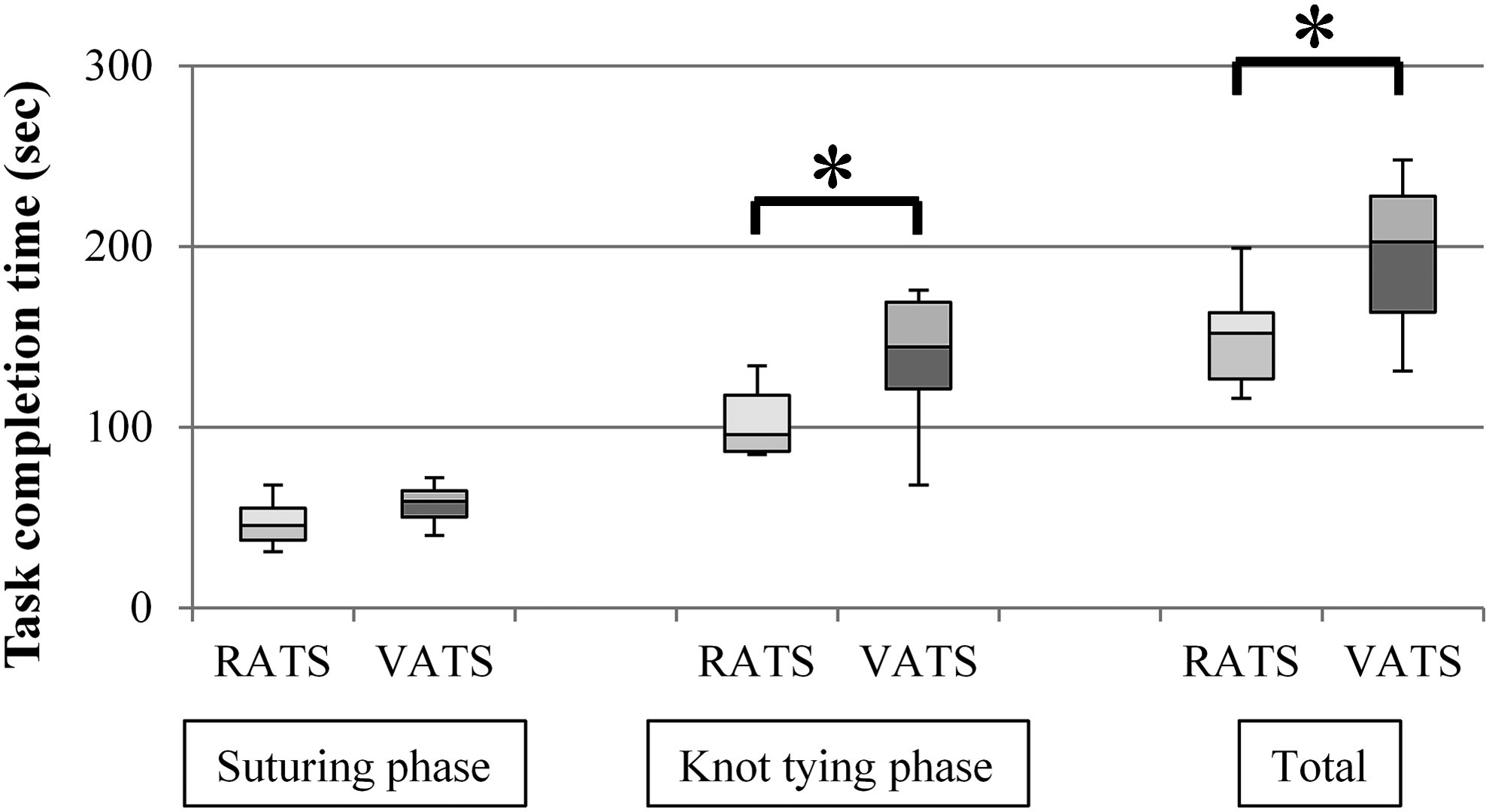
Comparison of the task completion time between the RATS and VATS groups. The central black line shows the median; data within the boxes are the interquartile ranges, and the ends of the vertical lines denote the range. *P < .05 by the Wilcoxon signed-rank test. RATS, the robot-assisted thoracoscopic surgery group; VATS, the video-assisted thoracoscopic surgery group.
The number of needle manipulations is shown in Figure 3. The RATS group showed a significantly smaller number of manipulations than the VATS group in the total phase [17.5 (6.5) versus 27 (8.0), P = .039]; however, no significant differences were observed in the suturing phase [6 (3) versus 6.5 (2.3), P = .91] and the knot-tying phase [12 (5.3) versus 20 (8), P = .086].
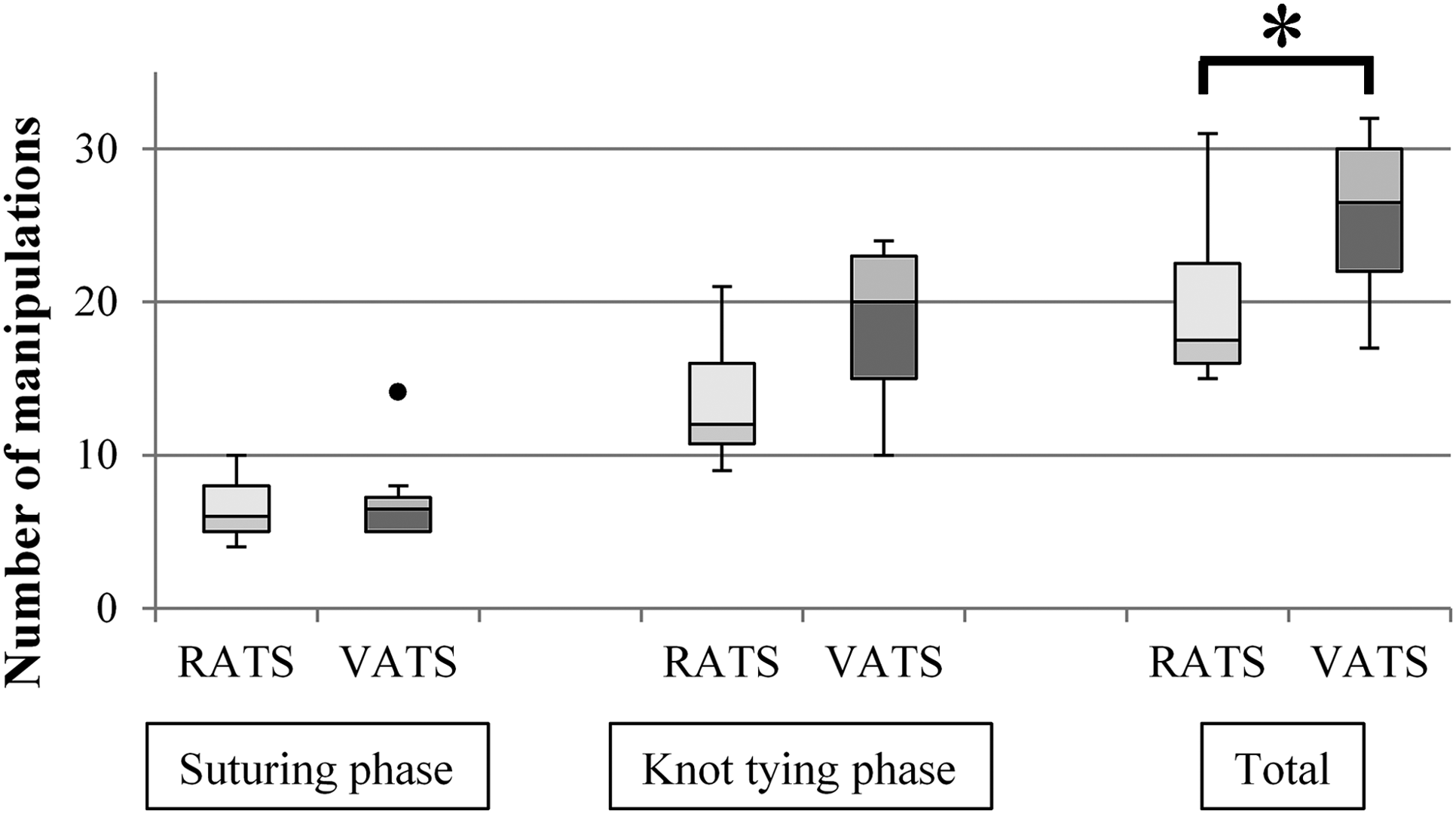
Comparison of the number of needle manipulations between the RATS and VATS groups. *P < .05 by the Wilcoxon signed-rank test. The dot denotes an outlier.
The data of 2 surgeons were invalidated in the force index analysis because of failures of the force measurement system. The pushing force index is shown in Figure 4. The RATS group showed a significantly smaller pushing force index than the VATS group in the suturing phase [54 (30) versus 422 (354), P = .031], knot-tying phase [297 (272) versus 901 (646), P = .031], and in the total phase [343 (233) versus 1431 (314), P = .031].

Comparison of the pushing force index between the RATS and VATS groups. *P < .05 by the Wilcoxon signed-rank test. RATS, the robot-assisted thoracoscopic surgery group; VATS, the video-assisted thoracoscopic surgery group.
There were no significant differences in the pulling force index between the RATS and VATS groups in the suturing, knot-tying, and total phases [suturing phase, 217 (49) versus 119 (152), P = .56; knot-tying phase, 137 (119) versus 162 (117), P = .84; and the total phase, 401 (79) versus 327 (372), P = 1.00].
There were no significant differences in the sidewall force index between the RATS and VATS groups in the suturing, knot-tying, and total phases [suturing phase, 526 (194) versus 413 (127), P = .84; knot-tying phase, 847 (358) versus 1180 (671), P = .16; and the total phase, 1428 (281) versus 1571 (475), P = .16].
Observation
The seventh rib in the pediatric thoracic model was dislocated during the suturing experiment in all RATS group cases (Fig. 5). The model itself was also pushed by the robot instrument and moved several times during the experiment.
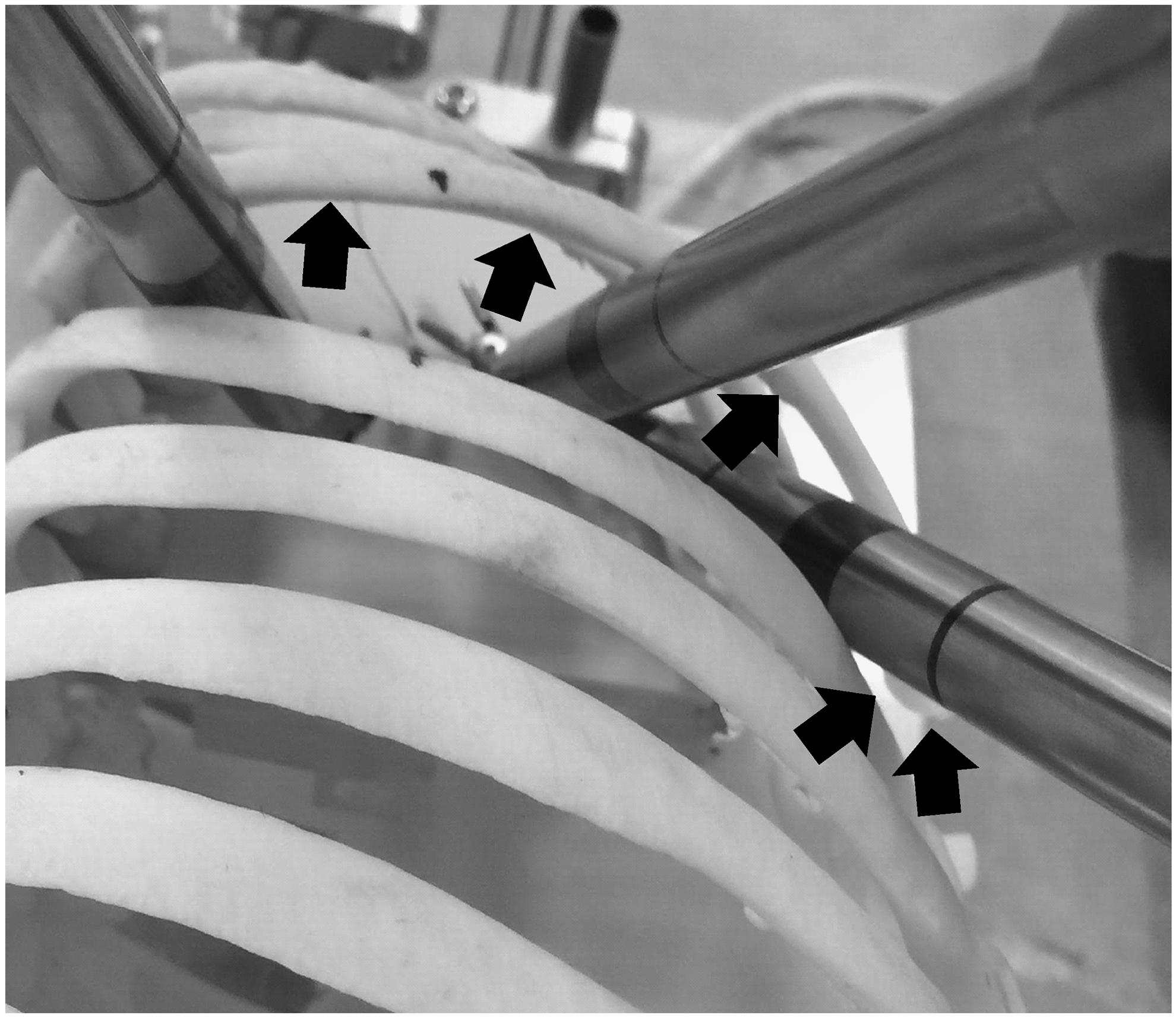
Dislocation of the seventh rib bone in the pediatric thoracic model. The seventh rib bone in the model was dislocated during the RATS experiment (arrows). RATS, robot-assisted thoracoscopic surgery.
Discussion
The RATS group had a shorter task completion time and smaller number of manipulations than the VATS group. Chandra et al. 19 reported a comparison of manual and robotic-assisted suturing performances in simulated laparoscopy using the ProMIS surgical simulator, and they reported that robotic suturing was faster than conventional laparoscopic manual suturing in an experimental environment, which was also observed in our study. In the RATS group, the surgeons completed the task more efficiently because the multi-DOF robotic instrument facilitated the grasping of a needle and thread. Another reason for the shorter completion time in the RATS group was that the da Vinci Surgical System provided 3D vision while the VATS suturing was performed using a two-dimensional (2D) camera; it was previously reported that pediatric laparoscopic suturing under 3D vision was faster than that under 2D vision. 20
In addition, the deformation of the suture pad in the direction of the vertical pushing force in the RATS group was smaller than that in the VATS group. Oshima et al. 13 reported that the measured deformation in the vertical pushing direction became larger when the needle insertion angle and/or the speed of insertion was increased. The robotic multi-DOF instruments assisted the surgeons in driving the needle along its curve, resulting in the small pushing force index in the RATS group. In contrast, it was difficult to perform such dexterous needle driving when using a conventional thoracoscopic instrument. The small force in robot-assisted surgery is an advantage because neonates and infants have fragile organs.
However, some disadvantages of pediatric robotic surgery were observed during the experiment. First, the robotic instruments were too large for use in the thoracic cavity of a 1-year-old infant. The seventh rib in the model became dislocated during the experiment in all cases because the diameter of the instrument, 8 mm, was larger than the intercostal space of the model that measured ∼5 mm. This result suggests that bone fracture or dislocation may occur if the current robot is used in an infant. Another factor in the dislocation may have been inappropriate port placement that led to application of a large stress on the seventh rib. The current pediatric thoracic model can be used to determine ideal port placement so that dislocation of the rib would not occur during RATS using the da Vinci Xi in the clinical setting. Second, the force applied by the instrument's shaft to the trocar was large and pushed the model. An infant's body also has a light weight, and would move easily if pushed with such a large force. A method to further reduce the force applied on the trocar needs to be developed for pediatric robotic surgery in neonates.
We propose the use of an artificial human body model to evaluate a surgical device. Several groups have studied pediatric robotic surgery and reported the feasibility and survival rate in animal experiments. 21 Animal experiments are often performed to demonstrate the feasibility of robotic surgery for neonates and infants, but have some limitations: for example, possible collisions of robotic instruments cannot be evaluated because experimental animals such as the porcine model and ovine model cannot sufficiently simulate the human neonatal body. Tanaka et al. 22 evaluated an eye surgical robot using an artificial eye model with a force sensor, demonstrating that such a model is useful for evaluating the usability and feasibility of robotic surgery when there is no adequate animal model. The use of artificial models is also ethical and can reduce the use of experimental animals.
During the RATS experiment, the trocars were placed at a lower intercostal space than during the VATS experiment because robotic instruments need a wider space. When we first oriented the robot and the pediatric thoracic model, we tried to place trocars in the fifth intercostal space as in the manual experiment. However, the distance between the thoracic wall and the suture target (i.e., the cut line in the suture pad) was too short for the robotic instrument to move properly (Fig. 1c). Then, the robotic tools were inserted in the seventh intercostal space. In the study of Thakre et al., 23 7 surgeons performed five drills using the da Vinci robotic instruments in cubic boxes of several different sizes; they reported that the drills could not be performed in a 45 mm or shorter edge cube due to significant collisions. Therefore, the available thoracic workspace in a pediatric patient varies depending on the patient's body size, and thus the intercostal space in which robotic instruments would be inserted needs to be carefully determined after evaluating the performance of the robot in the model.
In Japan, pediatric robotic operation is currently not reimbursed by health insurance, and most pediatric surgeons have no experience in performing robotic surgery. The participants in this study had sufficient experience in performing endoscopic suturing in a neonatal or infant body cavity but had no experience in pediatric robotic surgery. They practiced robotic surgery using the virtual reality simulator before the experiment using the da Vinci Surgical System. If more surgeons with experience in pediatric robotic surgery are identified, we will recruit them to conduct the same experiment.
In conclusion, the fast and smooth movement of the da Vinci Surgical System is an advantage for pediatric robot-assisted surgery in infants. In addition, the small pushing force that was applied during robotic suturing indicates gentle manipulation, which would reduce postoperative complications. However, the robotic 8 mm instruments were too large for use in the thoracic cavity of a 1-year-old infant. Pediatric surgical instruments can be evaluated using a sensorized artificial model before clinical use.
Footnotes
Acknowledgments
This study was supported by a Grant-in-Aid for Scientific Research (B) (No. 26293378) from the Ministry of Education, Culture, Sports, Science, and Technology (MEXT), and the project entitled “Assessment methodology for innovative minimally invasive therapeutic devices, materials, and nano-bio diagnostic devices” from the Accelerating regulatory science initiative, Ministry of Health, Labour and Welfare (MHLW), Japan.
Disclosure Statement
No competing financial interests exist.