
Abstract
Abstract
Introduction:
The aim of this study was to evaluate a new method of parastomal hernia (PSH) repair by using a hybrid approach with a cylindrical-shaped mesh of 4 cm funnel length.
Materials and Methods:
In a pilot prospective case series, 12 patients underwent surgical repair of PSHs with a combined laparoscopic and ostomy-opening approach. After laparoscopic adhesiolysis, the ostomy opening was excised from outside and the bowel was closed. The hernia sac was excised after reduction of its content. Then, the bowel was guided through the funnel of the mesh and the implant was manually transferred into the peritoneal cavity through the hernia defect. Next, the fascial margins were narrowed with sutures. Laparoscopy was continued, and the mesh was placed and fixed with absorbable tacks in the proper position. Finally, the diverted bowel was shortened outside of the abdomen and the stoma was matured in its original location.
Results:
We documented no mesh-associated complications. Only one superficial peristomal wound defect occurred. No unplanned conversions were needed, and median duration of the operations was 72 minutes. There was no recurrence during the short-term follow-up of median 4 months (ranged from 3 to 8 months).
Discussion:
The technique described gives several advantages, such as a minimally invasive hybrid approach creating a real three-dimensional mesh-covered barrier between the trephine and stomal limb and optional shortening of a concomitant prolapse. When needed due to a concomitant incisional hernia, a second flat mesh can be laparoscopically placed in an intraperitoneal position.
Introduction
I
Recently, three-dimensional (3D) funnel-shaped meshes have become available. Initially developed for the prevention of PSHs,5,6 they also showed to be suitable for their repair.7,8 The size of the gap between the trephine and bowel wall has concerned some as this area is never truly protected by any of the mesh methods that rely on keyhole trephines in the mesh, whether placed in the prefascial, retrorectus, or intraperitoneal position. 9 One way to circumnavigate this problem is to use a funnel-shaped mesh with the funnel directed intraperitoneally, thus creating a barrier between the viscera and the gap around the stomal limb.
Materials and Methods
In a pilot prospective case series, 12 patients underwent elective surgical repair of symptomatic PSHs with a combined laparoscopic and ostomy-opening approach by using pre-shaped 3D meshes at the Department of General Surgery, Sisters of Charity Hospital, Linz, Austria, between October 1, 2016 and February 31, 2017.
Evaluated data were retrieved from patients' files and documents deposited in the hospital's electronic data systems. All 12 patients with underlying oncological conditions were seen in the outpatient departments at 3-monthly intervals during the first 2 years. Follow-up examinations comprised the patients' medical history, clinical examination, blood test, abdominal sonography, and plain chest X-ray. We had a particular focus on recurrent PSH formation, ostomy-site complications, and potentially present mesh-associated problems. Computed tomography scans during abdominal press are scheduled 1 year after the operation and will be done earlier in cases of clinically suspected recurrence. In addition, from 2010 onward, all patients have been followed up in accordance with the Herniamed register's regulations, 10 that is, postoperatively, after 1, and (scheduled) 5 and 10 years. Recurrence, chronic pain, and local complications were recorded. Statistical evaluations were extended to descriptive calculations.
Technical description
Bowel preparation was carried out with 2 L of a saline solution on the day before the operation. Perioperatively, all patients received intravenous antibiotic prophylaxis (2 g cefuroxim and 0.5 g metronidazol) and an indwelling urinary catheter. In addition, a nasogastric tube was placed intraoperatively. The first 10 mm blunt tip® trocar (Medtronic) was always inserted in the open technique and well away from the ostomy on the contralateral side at the height of the umbilicus. The ostomy was covered with a swab under a transparent adhesive film after applying the pneumoperitoneum process. Otherwise, the film can come off due to extensive bulging at the stoma site by insufflation. The transparent film alleviates orientation and enables pointedly gentle manual compression during laparoscopic dissection if required.
The next step involved introducing two more 5 mm trocars under direct vision: one reusable metal trocar and one AirSeal® (DACH Medical Group GmbH, Ostermiething, Austria) trocar for balancing pressure changes (Fig. 1). Patients were operated on in supine position with one arm tucked under their body located contralateral of the ostomy side, and the laparoscopic unit was routinely positioned opposite the trocars—that is, on the side of the ostomy. To summarize, we aimed at reimplanting the ostomy on the same side in its original location once the diverted bowel segment had been passed through the funnel mesh in order not to create another abdominal wall defect. Further, we averted cutting the implant with consequent destruction of the mesh integrity and loss of its elasticity.

Trocar position.
Laparoscopic adhesiolysis of the midline and peritoneum around the trephine opening was performed to create at least a 7–8 cm overlap around the hernia (Fig. 2). For better orientation and identification of the bowel limb, a Foley catheter can be inserted from outside through the ostomy opening or alternatively, methylene blue solution can be instilled. Intraperitoneal adhesiolysis allowed one to detect any concomitant incisional hernias.
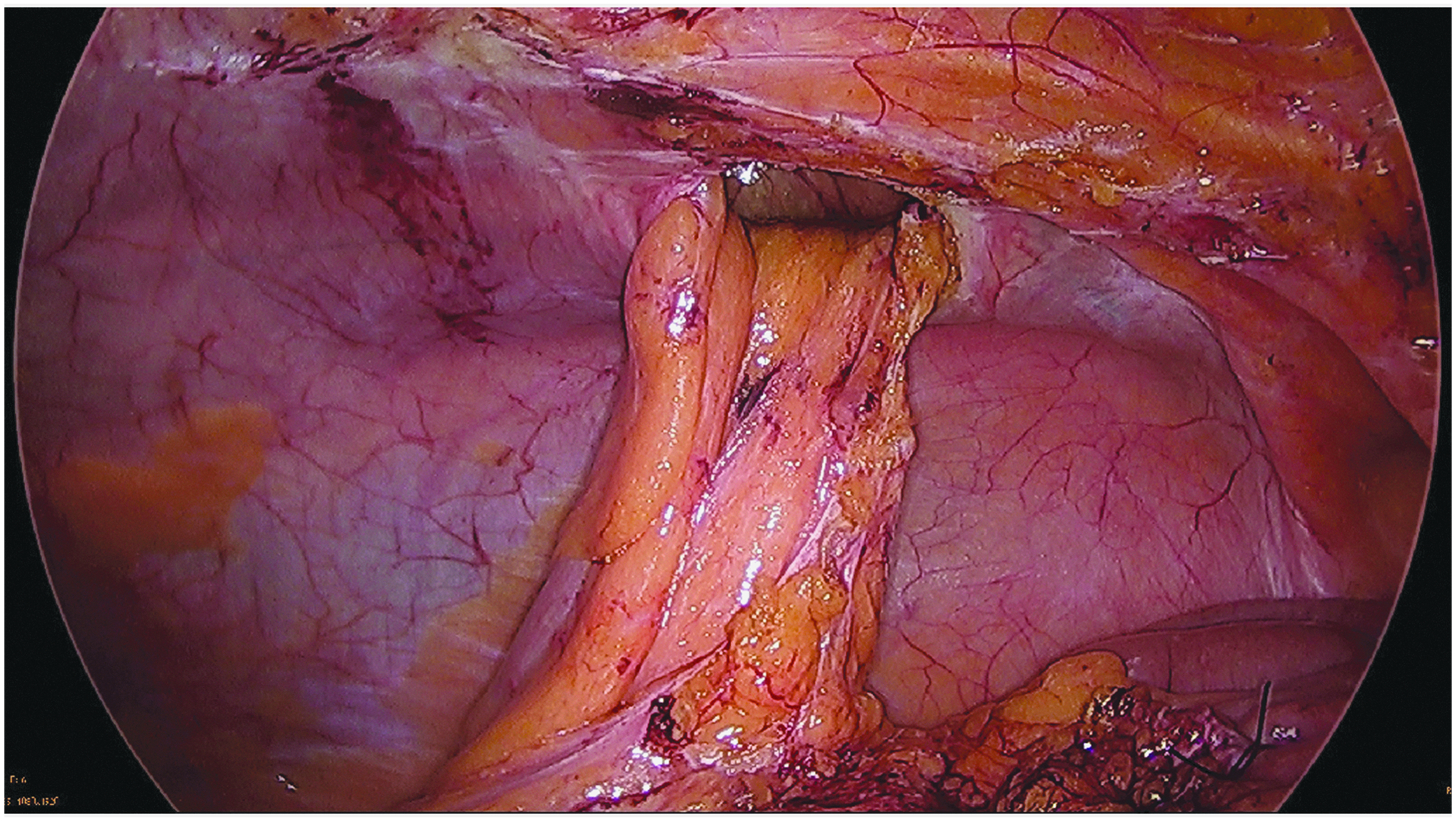
Laparoscopic adhesiolysis to ensure sufficient mesh overlap.
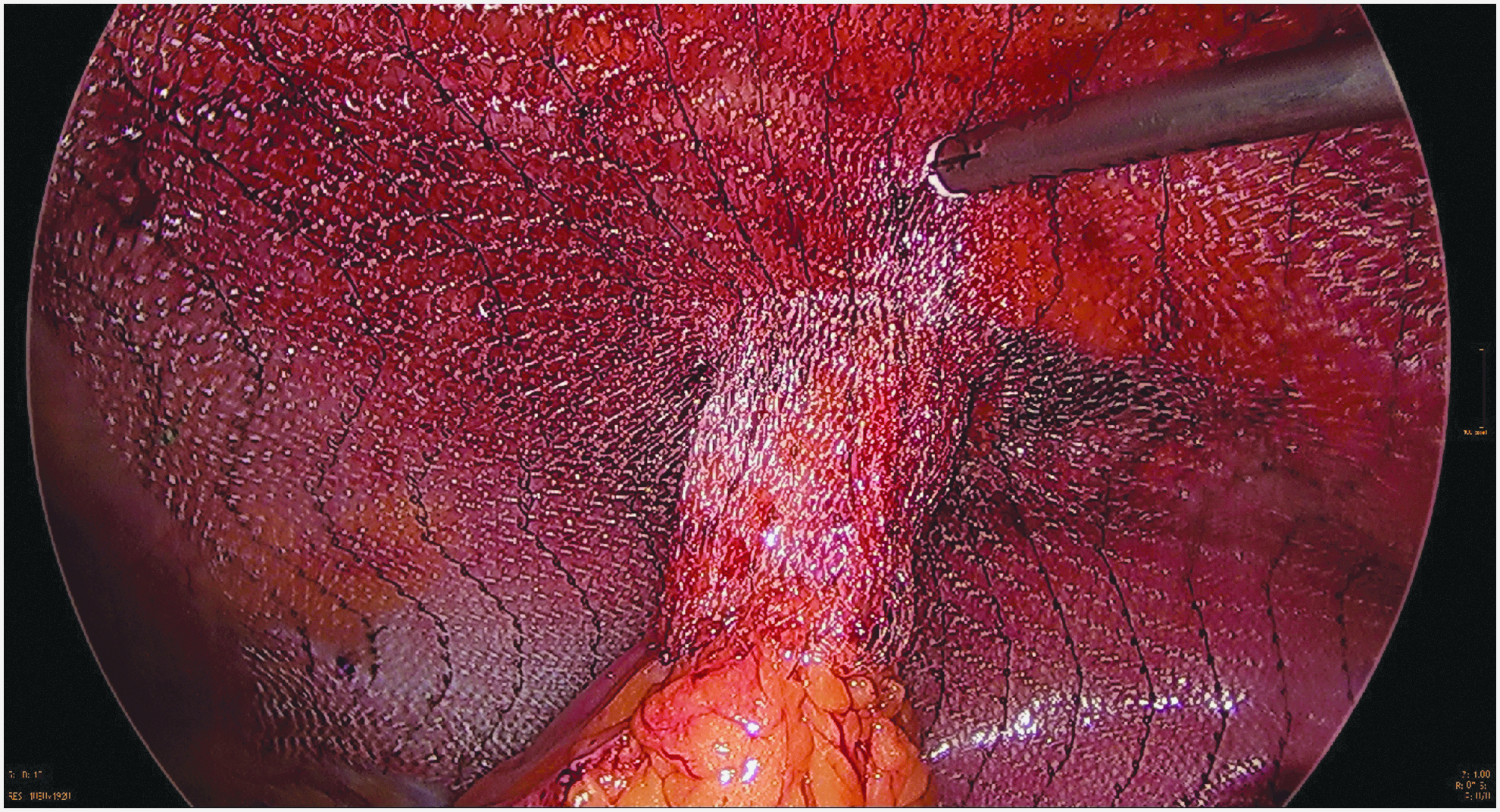
After laparoscopic adhesiolysis, the adjacent skin of the ostomy was sparingly excised from outside the abdomen along the mucocutaneous junction and the bowel loop was temporarily closed with a running suture (Fig. 3). Intra-abdominal pressure was maintained because it allows better visualization of the hernia sac and its proper dissection. The closed ostomy bowel segment was temporarily armed with sutures and replaced into the abdominal cavity. The hernia content was then reduced easily and safely, and the entire hernia sac was resected under direct view to prevent subsequent seroma formation (Fig. 4). Then, the closed diverted bowel loop was extracted and guided through the central funnel of a new mesh device outside of the abdomen (Dahlhausen, Dynamesh IPST®, FEG Textiltechnik, Aachen, Germany). Exclusively meshes of 15 × 15 cm diameter with a 2 cm central opening and a funnel length of 4 cm were used (Fig. 5). This is an improved design compared with the conventional meshes having a uniform funnel length of 2.5 cm. The implants are macro-porous and consist of visceral-sided polyvinylidene fluoride, including the seamless transition into the funnel and parietal-sided polypropylene. The elastic and rounded mesh tunnel rests around the diverted bowel and should, therefore, help to avoid erosion. Blunt junctions should protect the bowel segment and the special design, including a flat part, reliably prevents PSH formation. The implant was then manually transferred into the peritoneal cavity, with the funnel facing away from the abdominal wall toward the viscera (Fig. 6). The opportunity for an appropriate suture repair of the fascia to narrow the stoma opening at the PSH site with interrupted slowly absorbable monofilament sutures United States Pharmacopeia (USP) 0 was routinely used (Fig. 7).
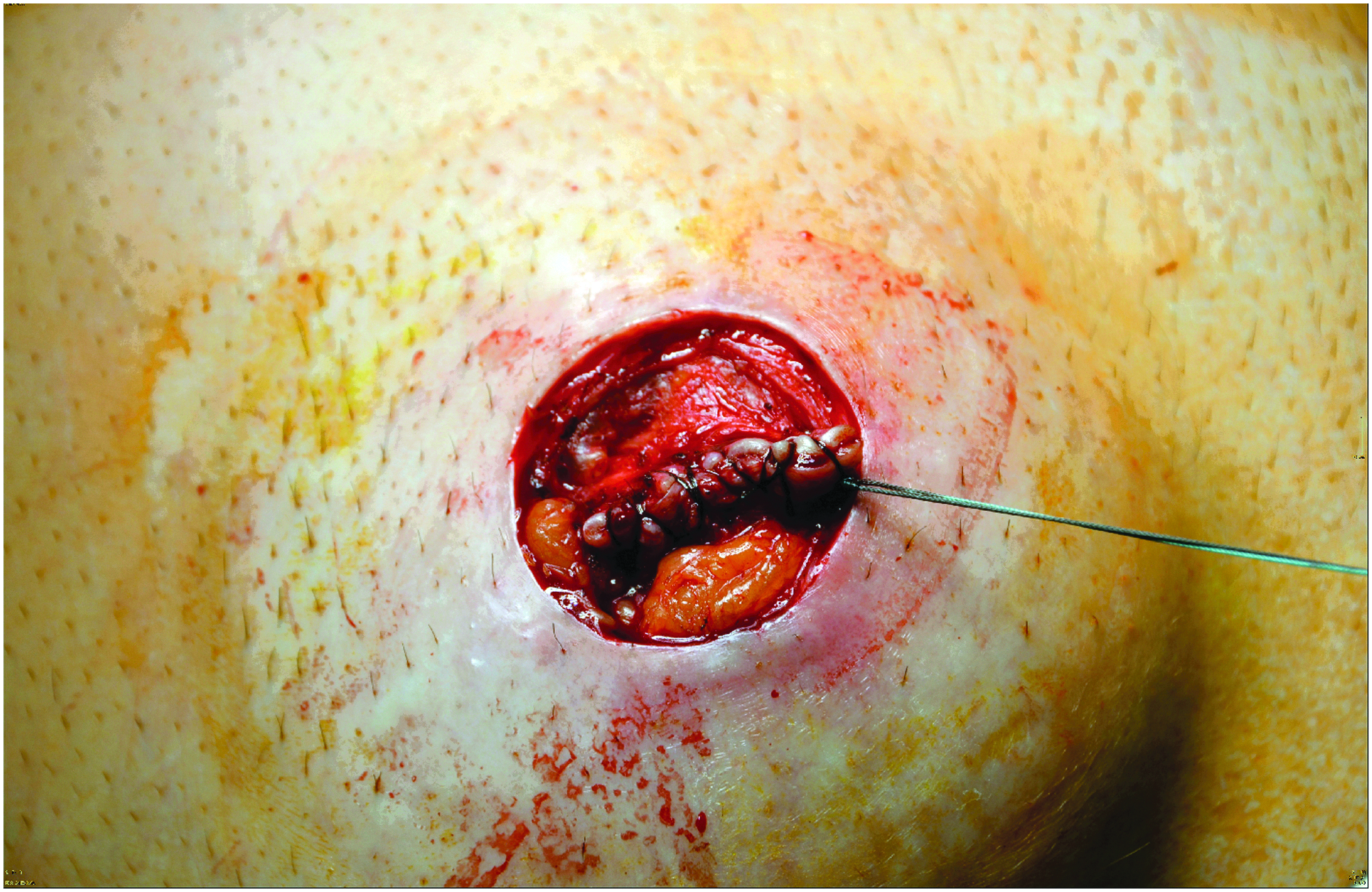
Peristomal skin incision along the mucocutaneous junction and ostomy closure with interrupted suture.
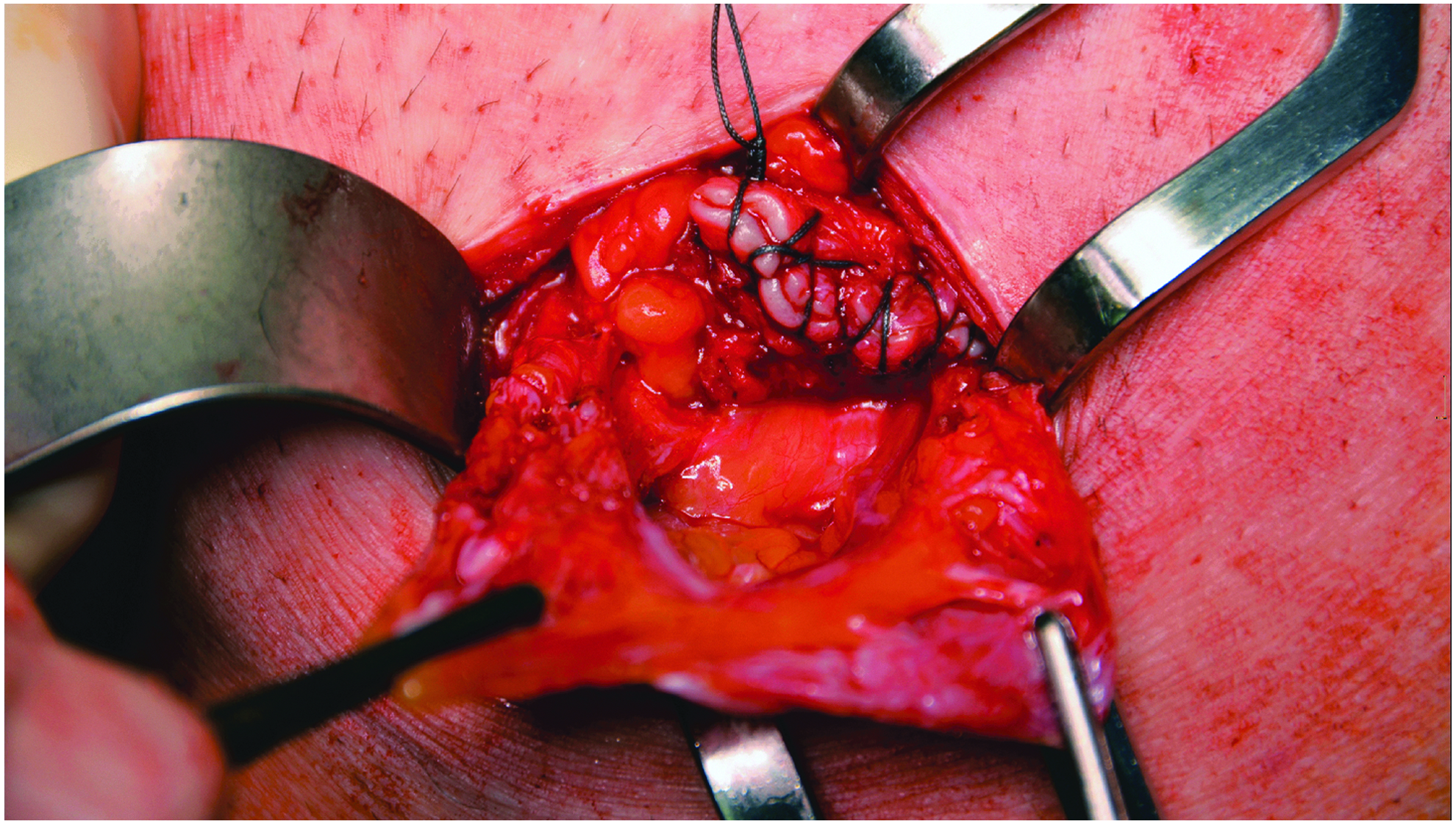
Excision of the hernia sac.

Depiction of the novel designed three-dimensional mesh with 4 cm funnel length.

The bowel is guided through the central funnel of the mesh device outside of the abdomen with the funnel facing the viscera.

Narrowing of the fascial defect with interrupted sutures.
After new application of insufflation and pneumoperitoneum achievement, the mesh was placed in the proper location by using laparoscopic instruments (Fig. 8). Laparoscopy was continued with AirSeal technology. This is a completely valve-free trocar and insufflation system, instantaneously balancing minimal or massive intra-abdominal pressure changes and, therefore, providing stable pneumoperitoneum even under challenging surgical conditions (airleak due to ostomy defect). Due to continuous smoke evacuation, a remarkably clear working environment was granted. The transparent and liquid permeable mesh implant was positioned inside the abdomen and fixated to the abdominal wall with absorbable strap devices (Ethicon, Securestrap®, Vienna, Austria) in the double crown technique, with the inner row close to the defect (Fig. 9). During the procedure, the mesh was already centered and maneuvered into position by the bowel inside the funnel, which further facilitated the orientation of the implant, which provides more elasticity in the longitudinal direction. When needed in the presence of a concomitant incisional hernia of the midline, a second-sized flat mesh was laparoscopically placed in the intraperitoneal position.
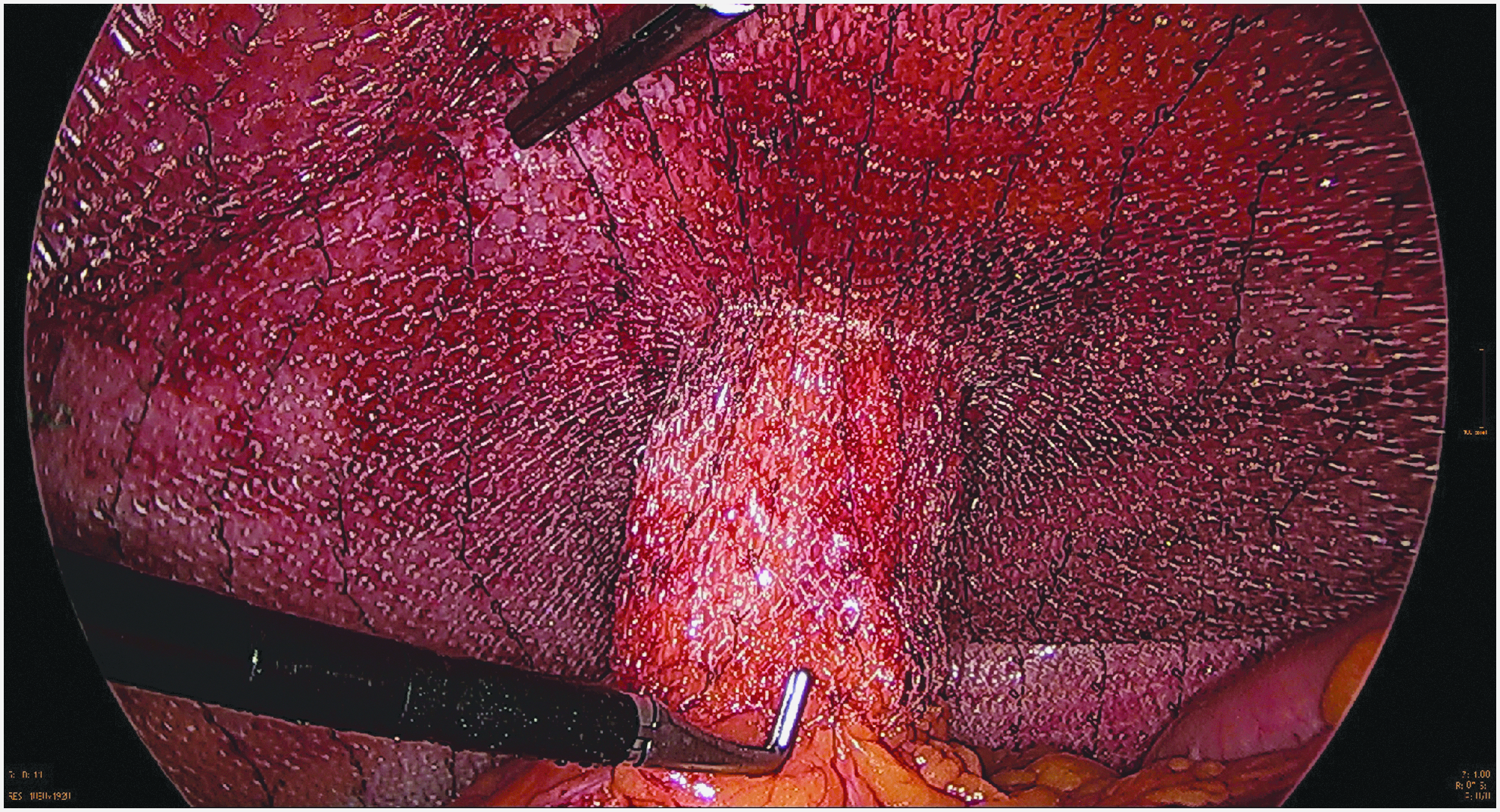
Laparoscopic mesh placement.
Laparoscopic mesh fixation.
To ensure permanent interconnection of the two meshes, areas where the two implants overlapped were secured with nonabsorbable fixation devices (Protack®; Medtronic) (Fig. 10). After deflation and removal of the trocars, the trocar openings were closed with interrupted sutures. Finally, the diverted bowel was shortened to a suitable length outside the abdomen to reduce an often-present concomitant prolapse (Fig. 11) and the stoma was refixed and fashioned at its original location with mucocutaneous interrupted sutures (Fig. 12). No drains are routinely used. Figure 13 shows the final situs from outside.

Occasional flat mesh placement in intraperitoneal position for covering a concomitant incisional hernia.

Stoma bowel shortening due to prolapse.

Stoma maturing at its initial location with mucocutaneous sutures.

Final situs from outside.
Results
We previously reported our results by using this technique for PSH repair,7,8 with an exclusively 2.5 cm funnel length of the 3D meshes. During the updated follow-up period of roughly 36 months, we currently recorded about 12% PSH recurrences (unpublished). We ascribe this fact mainly to the short funnel length and return to this in the “Discussion” section. For this analysis, we exclusively used 12 pieces of the specially new designed mesh with 4 cm funnel length and 2 cm funnel diameter, which has not been commonly commercially available so far. All operations could be completed without intraoperative complications and without conversions to open procedures. The mean operation time was 72 minutes.
Table 1 describes the detailed demographics, disease characteristics, 11 and procedure-related complications. 12 It is notable that no intraoperative complications and no postoperative mesh-related complications occurred. Further, no stoma retraction or bowel obstruction was recorded. The elastic funnel fits tight to the bowel but obviously does not lead to bowel restriction. One subcutaneous peristomal wound complication could be handled with conservative wound management. No patients were lost to follow-up (ranged from 3 to 8 months), and no early recurrence was observed.
Smietanski M, Szczepkowski M, Alexandre JA, et al. European hernia society classification of parastomal hernias. Hernia 2014;18:1–6 (small is ≤5 cm; cIH, concomitant incisional hernia); Type I = small PSH without cIH, Type II = small PSH with cIH, Type III = large PSH without cIH, Type IV = large PSH with cIH. 10
Risk factors in hernia surgery: (1) Diabetes mellitus, (2) COPD, (3) Nicotine dependence, (4) Coagulopathy, (5) Cumarine, (6) ASS (acetylsalicylic acid), (7) Aortic aneurysm, (8) Immunosuppression, (9) Corticosteroids.
Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg 2004;240:205–213. 11
ASA, American Society of Anesthesiologists; BMI, body mass index; c, colostomy; EHS, European Hernia Society; i, ileostomy; OP, operation; PSH, parastomal hernia; u, urostomy; 3a, Clavien-Dindo classification–peristomal wound defect requiring wound care but without need for a re-operation.
Discussion
We developed a new technique for the repair of PSH formation in 2012 and published our first experiences in 2014. 7 Although the technique is partly based on a small open approach, it still remains a minimally invasive procedure because the ostomy location remains unchanged. Repositioning of the diverted bowel through a 3D funnel mesh gives several advantages: The funnel meshes can be used in laparoscopic-assisted (hybrid) and open surgery. The PSH defect can be covered locally with a wide overlap to all sides. By using a second flat mesh, preexisting midline incisions can be well covered to treat concomitant incisional hernias. A positive effect on prolapse prevention arises from the dome, which is directed toward the abdominal cavity and fits to the bowel tightly, especially by using the novel implant with a tunnel of 4 cm length. The local fascia can be approximated with loose contact to the bowel to ensure adequate stoma function while providing a broad landing zone for the underlying mesh, preventing pseudo-recurrence due to mesh bulging. The parastomal fascial defect area in which PSHs commonly occur is well covered by the 3D design, whereas the surrounding abdominal wall remains supported with sufficient overlap by the flat part of the mesh.
Wound complications such as hematoma and infections should decrease compared with open techniques since the different layers of the abdominal wall need no separation. The “ipsilateral” (same sided) stoma relocation provides further advantages over the usually performed intraperitoneal onlay mesh (IPOM) techniques (keyhole, Sugarbaker, and sandwich).1,4 First, the localized approach easily allows for complete excision of the hernia sac, preventing seroma formation and the implant can be placed easy and quickly compared with the effortful laparoscopic Sugarbaker and sandwich techniques. The edges of the funnel opening are less likely to cause erosions since the fibers of the dome are molded into a perpendicular configuration and, therefore, run parallel to the bowel. The anatomical change in bowel configuration due to lateral deviation with the risk of obstruction caused by the “Sugarbaker” mesh can also be averted. The possibility of bowel irrigation for an improved quality of life is still ensured because of the unchanged straight course of the ostomy bowel. A lateral position of a fascia defect is also a weak point of the “Sugarbaker” technique because lateral parastomal defects cannot be well covered. 13
The purely laparoscopic techniques sometimes require an extensive surgical experience due to a potentially very difficult dissection and might not always be feasible due to dense adhesions and tissue scarring. The discrimination between stoma bowel, hernia sac, small bowel adhesions, bowel mesentery, and omental fat can be very difficult. Moreover, the impossibility to reduce or mobilize a large hernia and its sac's purely laparoscopic content may also limit its use. However, it is fundamentally important to dissect the ostomy bowel along its route through the whole abdominal wall. The bowel must go straight out of the skin opening by eliminating the typically siphon-like curve in a subcutaneous way, predisposing hernia and prolapse development. This is very advantageous regarding our described hybrid technique because it is solely necessary to free the abdominal wall laparoscopically several centimeters in all directions around the ostomy to ensure sufficient mesh overlap subsequently.
The remaining part of peristomal adhesiolysis is performed by the local open approach. The subcutaneous stomal prolapse can hardly be influenced with purely laparoscopic techniques. By using our hybrid technique, it is feasible to shorten the bowel until its suitable length and to prevent new prolapse formation by the tight-fitting mesh funnel. In some situations, there is a need for sigmoid ostomy translocation to the right side of the abdominal wall. In such a case, we do not recommend using the Sugarbaker technique due to a high risk of obstruction by creating a double curve. If an ileal conduit is lateralized, the insufficient propulsive peristalsis can lead to urinary obstruction, with sepsis caused by intestinal bacteria. The use of 3D funnel meshes in such cases is precisely once more a good option. All the same, in difficult cases requiring an open approach, the funnel mesh can be placed in the open IPOM technique.
We aim at reducing the PSH recurrence rate by using a new mesh with a 4 cm-long funnel in a pilot case series instead of the uniform 2.5 cm funnel length, which has been so far available. If the bowel mesentery is bulky and fat, the encasing funnel distends and becomes shortened in relation to the increasing diameter. This fact can lead to recurrence due to insufficient overlap of the mesh wrap around the bowel. Therefore, a 2.5 cm funnel seems to be too short and rather resembles a keyhole repair than a real funnel mesh augmentation.
It is notable that we recorded not a single stoma stenosis or bowel erosion due to mesh shrinkage neither in former cases with adequate follow-up 8 nor in this series. From our observations of redo surgeries, we learned that the mesh shrinkage of the flat parts happens in a concentric manner, with consequential eccentric funnel widening inducing PSH recurrence. The contraction of the funnel actually enlarges the opening, but it is hard to estimate the extent to which this occurs. The results of an experimental study regarding IPOM in rats clearly demonstrated that both in vivo and in vitro, the major reduction in mesh area due to shrinking was demonstrated between days 7 and 14, whereas after 21 days, it already seemed to narrow to a plateau. 14
The follow-up time after surgery is short and the number of cases is still low to allow conclusions, but we are convinced that the initial experience with a new funnel mesh is worth further outcome research ideally in the fashion of randomized controlled trials comparing funnel meshes with established techniques of PSH repair.
Footnotes
Disclosure Statement
No competing financial interests exist.