
Abstract
Abstract
Background:
Endoscopic vacuum-assisted closure (EVAC) therapy is increasingly being used as a new promising method for repairing upper gastrointestinal defects of different etiologies with high success rates. EVAC therapy consists of placing a sponge either within the lumen or within an abscess cavity connected with a nasogastric (NG) tube to a negative pressure system, thus decreasing bacterial contamination and edema and promoting granulation tissue proliferation, thereby gradually decreasing the cavity size until complete closure. Herein, we describe a modified technique for EVAC therapy in which the NG tube is passed into the esophagus through an existing intrapleural drain tract using a rendezvous technique. The small residual fistula was amendable to fibrin glue embolization. This allows easier sponge placement and exchange compared to traditional EVAC technique, and allows oral intake during treatment. We also review the literature regarding other endoscopic treatment options for esophageal anastomotic leaks and perforations.
Methods:
The PubMed database was searched using the terms “esophagus,” “esophageal,” “leak,” “fistula,” “endoluminal vacuum-assisted closure (VAC),” “endoscopic VAC,” “stent,” “sealant,” “glue,” and “over-the-scope clip (OTSC).” Reference lists of identified articles were searched for further articles, and the “similar articles” function was used on all included articles.
Results:
Complete closure of the nonhealing fistula was achieved after 8 days of EVAC treatment and fibrin glue embolization.
Conclusions:
Modified EVAC technique as described is feasible and safe. To the best of our knowledge, this is the first description of this technique. The technique allows easier sponge placement and exchange compared to traditional EVAC technique, and allows oral intake during treatment.
Introduction
I
Herein, we describe a modified technique for endoscopic vacuum-assisted closure (EVAC) therapy in which the NG tube is passed through an existing intrapleural drain tract with a rendezvous technique. This modification carries several advantages, which will be discussed.
Methods
The PubMed database was searched using the terms “esophagus,” “esophageal,” “leak,” “fistula,” “endoluminal VAC,” “endoscopic VAC,” “stent,” “sealant,” “glue,” and “over-the-scope clip (OTSC).” Reference lists of identified articles were searched for further articles, and the “similar articles” function was used on all included articles.
Results
Case history
A 48-year-old man presented to our institution with progressive dysphagia for 6 months, without significant weight loss. His past medical history is significant for end-stage renal disease with hemodialysis, hypertension, diabetes mellitus, peripheral neuropathy, and heavy smoking.
Esophagogastroduodenoscopy (EGD) showed a mass at the gastroesophageal junction. Biopsy was consistent with adenocarcinoma within Barrett's esophagus. The disease was staged as cT2N0M0 by endoscopic ultrasound and positron emission tomography/computed tomography (CT). The patient underwent an uneventful three-hole minimally invasive esophagectomy. An upper GI series performed on the sixth postoperative day did not show any leak. The NG tube was removed and the patient was started on clear liquids. Turbid drainage appeared in the cervical drain on the next day and within a few hours, through the chest tube as well. A CT scan showed a leak at the level of the cervical anastomosis, draining completely into the chest drain.
During the following days, the output in the drains gradually decreased from 1000 to 200 mL/day. The patient was kept on clear liquids and received tube feeding through a feeding jejunostomy and showed no signs of sepsis. Three weeks following surgery, the fistula failed to close and an 18 × 103 mm fully covered metal stent (WallFlex esophageal stent; Boston Scientific, Marlborough, MA) was placed, which completely sealed the leak for 72 hours. No means for securing the stent in place were employed. At this point in time, the stent migrated and a leak reappeared at a rate of 20–30 mL/day. Three weeks later, the stent further migrated and was eventually removed. Repeat EGD showed a smaller defect at the anastomosis and an 11/6t sized OTSC was placed (Ovesco Endoscopy AG, Tübingen, Germany). The clip was misplaced and occluded the gastric lumen, leaving the fistula opening intact. Removal attempts by cooling, as recommended by the manufacturer, and Argon probe failed, and the clip was eventually removed using the Ovesco remOVE system (Ovesco Company).
Following removal of the clip, EGD showed a widely patent conduit. At 10 weeks from surgery, the fistula persisted; the patient was still on clear liquids with tube feeds, in good nutritional status, and showed no signs of sepsis. We decided to place an EVAC system to close the fistula. Since the patient was reluctant of having an NG tube, we decided to place the NG tube through the external cutaneous fistula opening (Fig. 1).
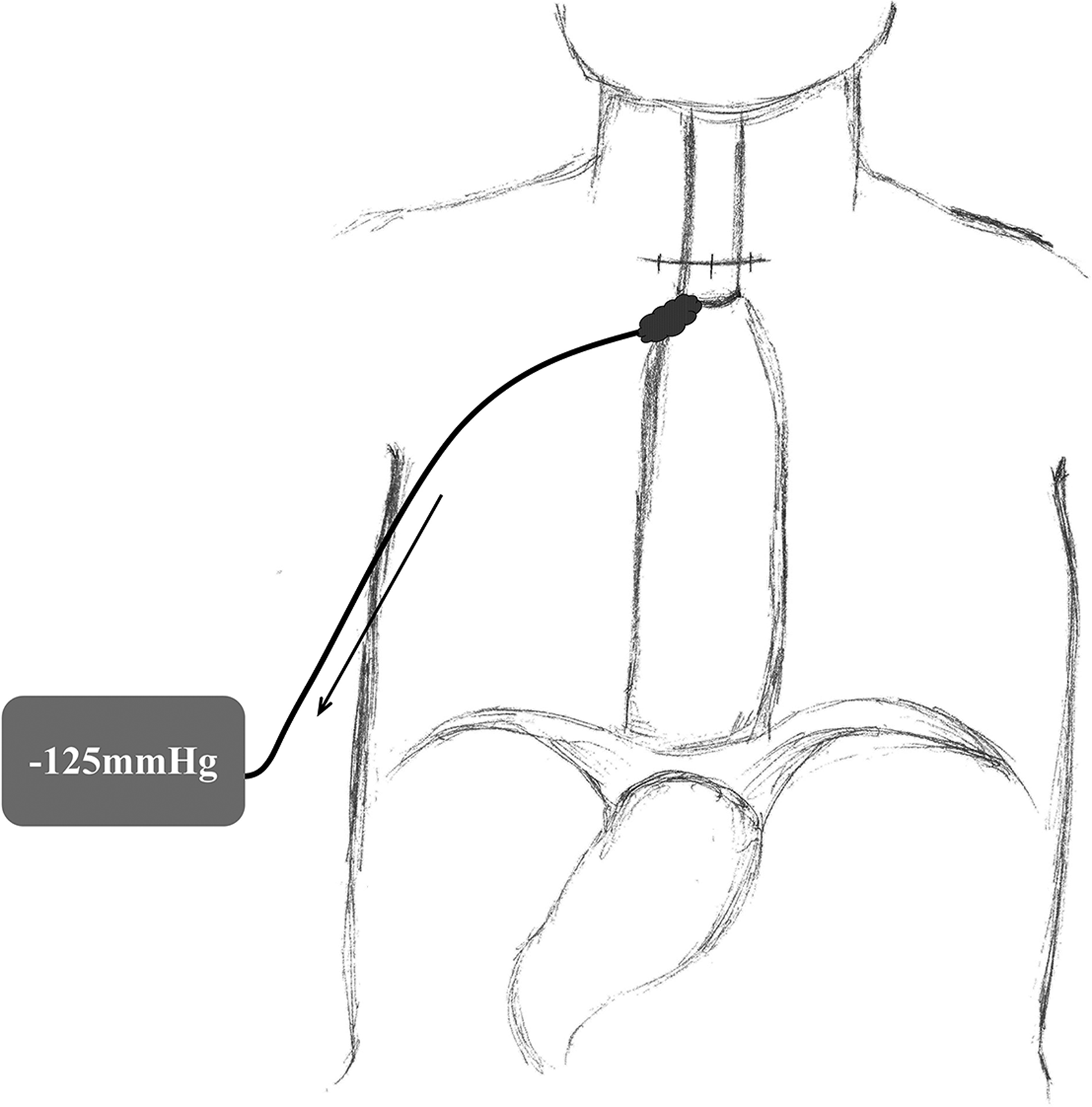
The modified endoscopic vacuum-assisted closure system: a small caliber NG tube is passed through an existing chest tube tract. NG, nasogastric.
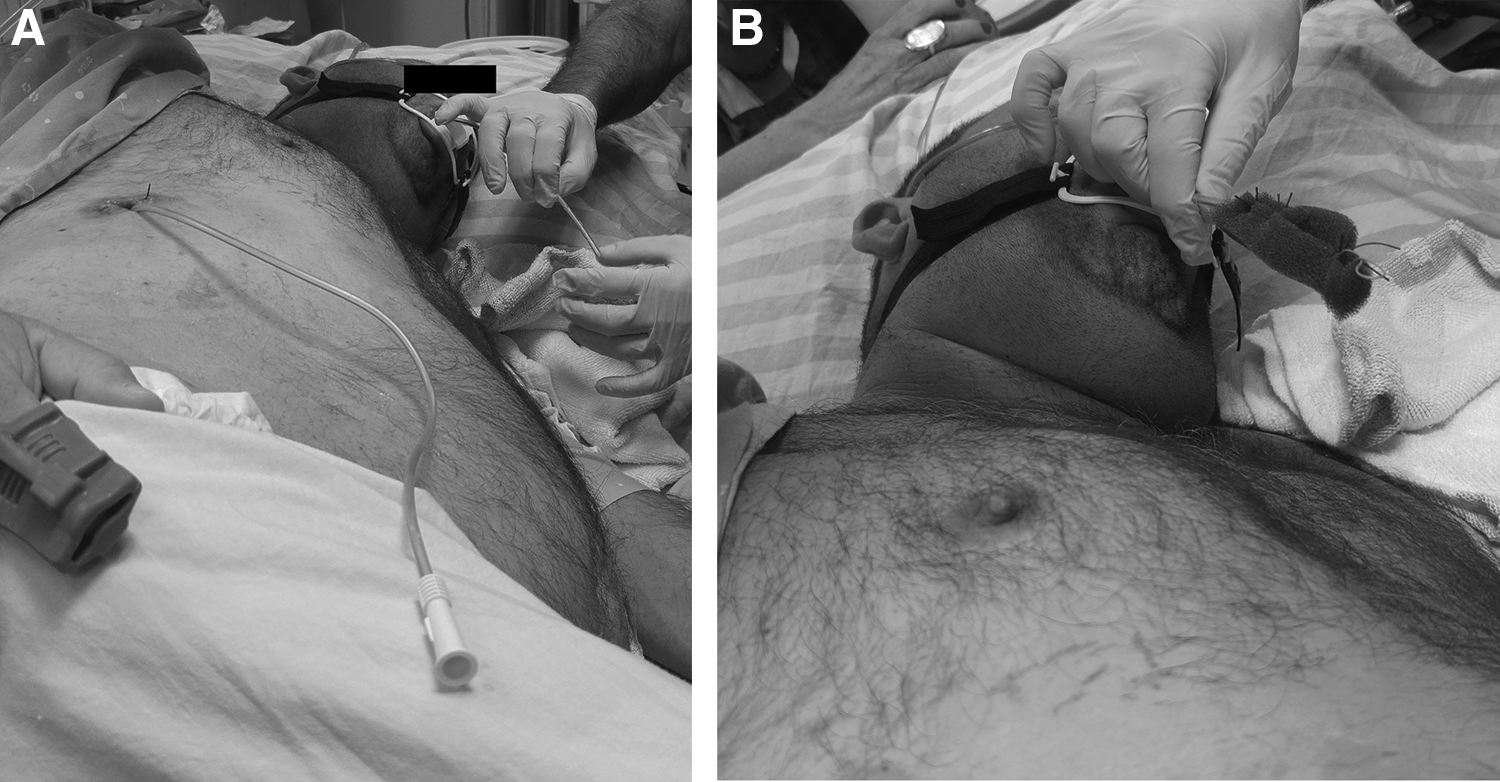
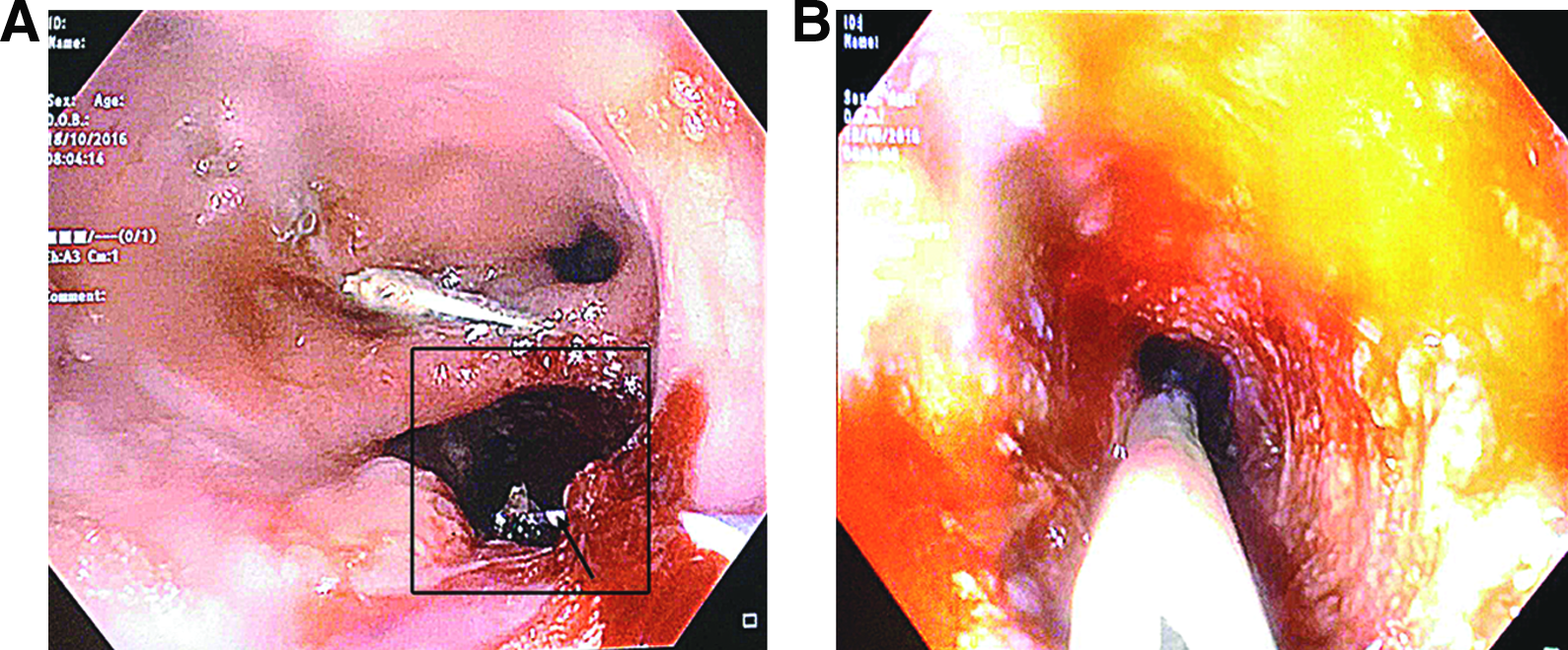
The patient was taken to the endoscopy suite and under conscious sedation, a rendezvous technique was used—a guide-wire was passed through the external fistula opening and grasped with an endoscopic snare once it emerged through the internal fistula opening, brining it out through the mouth. An 8F NG tube was passed over the guide-wire. A heavy nonabsorbable suture was placed at the tip of the NG tube for easy retrieval once the sponge is changed. A properly sized sponge was sutured to the tip of the NG tube (Fig. 2a, b) and pulled under endoscopic guidance into the internal fistula opening (Fig. 3). Continuous suction was applied to the system and set at −125 mmHg. The sponge was replaced under sedation 3 days later, showing a significantly smaller cavity with a clean base. A smaller sponge was placed and after 5 days, the fistula opening had reduced to the size of the NG tube (Fig. 4).
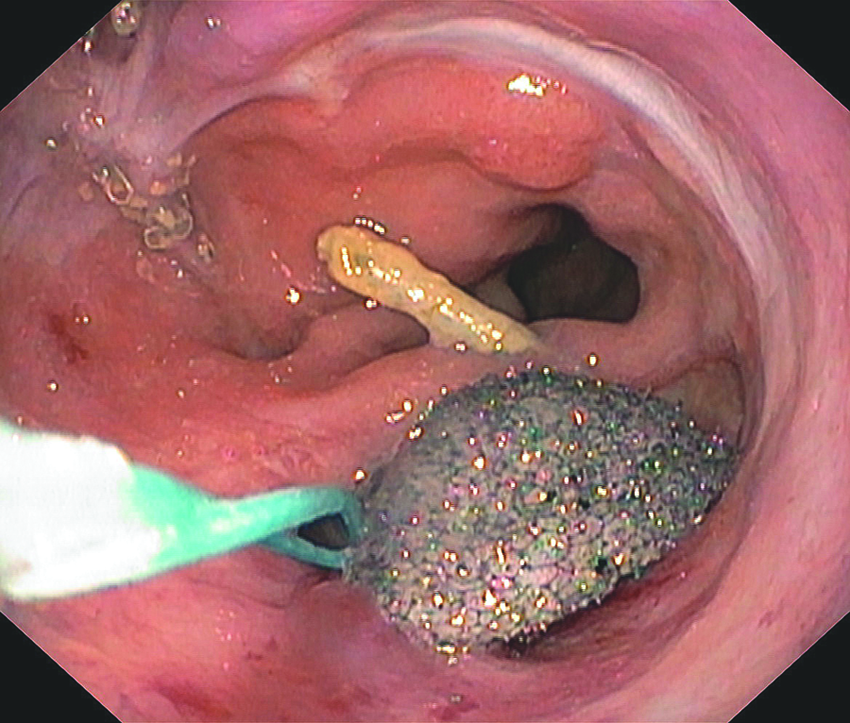
The sponge was pulled into the esophagus and positioned in the internal fistula opening under endoscopic guidance.
The patient was allowed water and tea during the first 5 days of EVAC treatment, and advanced to a full liquid diet during the following 3 days. The output through the EVAC system was about 30cc/day during the first sponge session and about 60–100cc/day during the second sponge session, and seemed to be related to sponge size or position, rather than the patient's diet. We did notice that the nightly output did not differ significantly from the daily output.
Once the EVAC therapy was finished, the fistula opening was then embolized with 10 mL of fibrin glue (Evicel; Omrix Biophamaceuticals Ltd., Ramat-Gan, Israel) with complete closure of the fistula: the 45 cm Evicel application catheter was introduced through the external fistula opening until its tip was seen by the endoscope emerging from the internal opening. The glue was then injected to the tract, while withdrawing the catheter.
An 8F NG tube, similar to the one used for the EVAC system, was placed superficially as a drain in the fistula tract, with its tip 7–8 cm from skin level. No drainage emerged and the drain was removed 3 days later. An upper GI study following fibrin glue embolization showed no evidence of fistula, and the patient was discharged 5 days later on a full liquid diet for 2 weeks, and gradually advanced to a regular diet. An upper GI study and EGD performed 3 months following discharge due to dysphagia showed no evidence of stricture or fistula, and at the 11-month follow-up, the patient is eating a regular diet with improving dysphagia.
Table 1 summarizes published data for EVAC outcomes for upper GI defects.
Schniewind's study excluded from analysis since no data provided regarding fistula closure rates.
Late bleeding excluded from analysis.
EVAC, endoscopic vacuum-assisted closure.
Discussion
Intrathoracic anastomotic failure is one of the most dreadful complications of esophagectomy, occurring in 7%–8% of cases. Mortality rate may be as high as 18%–50%,5,6 especially if treatment is delayed beyond the first 24 hours. Until recently, therapy consisted of surgical control of the leak and wide drainage of the pleural space. Even with timely intervention, the morbidity and mortality are high. 5 Endoscopic techniques have been successfully applied to this life-threatening complication with good results. Herein, we will review these options and describe our modification to the endoscopic vacuum-assisted fistula closure.
Endoscopic vacuum-assisted closure
EVAC therapy has emerged in recent years as a reliable treatment for esophageal anastomotic leaks and perforations. It consists of a sponge placed either within an extraluminal abscess cavity or intraluminally across an internal fistula opening, and through an NG tube to a negative pressure system. Reported success rates range from 86% to 100%,7–10 but only small case series have been published.
Ahrens et al. 11 reported a prospective study of five patients with esophagogastric anastomotic leak after esophagectomy treated with EVAC. The sponges were changed thrice a week with a median of nine sponge changes and mean time to cavity closure of 42 days. The authors reported a 100% success rate. Two patients developed anastomotic strictures necessitating dilatations. One of these patients died of massive aortoesophageal bleeding following dilatation.
The largest prospective cohort study of the use of EVAC among patients with perforations and anastomotic leakage of the upper GI tract was published by Laukoette et al. 3 The authors reported the use of EVAC among 52 patients with anastomotic leak after esophagectomy or gastrectomy (n = 39), and esophageal perforations (n = 13). Negative pressure of 125 mmHg was applied in all patients. EVAC therapy was started after 5.5 days from the diagnosis of the leak with a median therapy length of 22 [3–104] days. Median hospital stay was 53 [16–180] days. Sponges were changed every 3–5 days and were placed either into the extraluminal cavity or intraluminally in case of small defects. Patients were fed through an NG tube, gastrostomy or jejunostomy.
Success rate was 94%. EVAC failed to completely close the internal fistula opening in two patients. In one patient, the fistula was closed with an OTSC, and in the other, a self-expanding covered metal stent was placed. Four patients developed late strictures after termination of the EVAC therapy, managed by endoscopic dilatations.
Two patients died due to massive hemorrhage during sponge changes. The authors report that both patients developed a leak after distal esophagectomy. The first patient died due to acute hemorrhage that occurred during sponge exchange on the 56th EVAC day with subsequent cerebral edema and intracranial air embolism resulting from esophageal-right atrial fistula found at autopsy. The second patient died due to a nonmanageable bleeding during the 12th EVAC day, at a scheduled endoscopic change of the sponge. The authors report a massive hemorrhage after removal of the sponge, assuming rupture of the descending aorta. The authors could not identify any predictive factors for this devastating complication, and note that despite these two cases, there was subsequently no additional need for termination of EVAC due to a close contact of the sponges with cardiovascular structures.
These two rare devastating complications along with the late fatal bleeding during dilatation reported by Ahrens et al., 11 mentioned earlier, represent sponge erosion into a major cardiovascular structure or adhering the now closed fistula to one as in the latter case. This complication occurred in 1% of reviewed cases (Table 1). Dense inflammation during sponge placement precludes visual identification of the surrounding mediastinal structures to avoid placement of the sponge next to a major cardiovascular structure. One possible solution is carefully reviewing imaging studies, such as chest CT for the proximity of such structures to the fistula bed. In these cases, EVAC may carry a higher risk of bleeding, and care should be taken in these patients. The novel method we present does not address this potential complication.
Schniewind et al. 12 compared the results of 62 patients with esophagogastric anastomotic leak who were either treated surgically (n = 18), with endoscopically placed stent (n = 12) and with EVAC therapy (n = 17), or conservatively (n = 15). The authors compared Acute Physiology and Chronic Health Evaluation II (APACHE II) scores, in-hospital mortality, cervical leakage, and mean in-hospital time and time in the ICU.
The compared groups of patients were not homogeneous. Patients who were treated conservatively had a lower APACHE II score (5 ± 2 vs. 14 ± 4 in the EVAC group, 15 ± 5 in the surgical treatment group, and 11 ± 3 in the stent treatment group). In systemically ill patients matched for APACHE II scores, patients treated by EVAC had a lower mortality rate (12%) compared to surgically treated cases (50%, P = .01) and patients managed by stent placement (83%, P = .00014). Another retrospective study compared the effectiveness of EVAC (n = 7) versus covered self-expanding metal stents (SEMS) (n = 11) among 18 patients with esophagogastric anastomotic leak. Success rate among the EVAC group was 100% compared to 63% in the SEMS group. EVAC group had a shorter hospital stay (37.1 vs. 87.1 days) and fewer complications (0% vs. 54%).
The most challenging part of the EVAC procedure is placement of the sponge into the cavity, since the sponge obstructs the view of the endoscope. The technique we used overcomes this limitation since the sponge is pulled into place under endoscopic guidance and not pushed, greatly simplifying the placement process. Each procedure lasted ∼20 minutes. The other major advantage of this technique is that it allows the patient to continue oral intake, obviating the need of a transnasally placed NG tube. The disadvantage of this technique is the residual fistula at the end of the treatment, which is the size of the NG tube used. For this reason, we used the smallest NG tube possible. The remaining fistula could then be closed either by a short course of conventional EVAC technique or by glue embolization, as elected in the presented case. A single application of fibrin glue sealed the remaining fistula. To the best of our knowledge, this is the first report of such a technique.
Tissue sealants
There are scarce reports of the use of sealants to treat postoperative esophageal leaks and perforations. There are two major groups of sealants: cyanoacrylates and fibrin glues. 13
Successful embolization of pancreatic fistulae, 14 prolonged bile leaks, 15 and esophagus-bronchial 16 fistulae have been described in case reports and small case series. A systematic review of case series by Lopez et al. reported a cumulative success rate of 81% in embolization of enterocutaneous fistulae. 17 Few studies have described its use in esophageal leaks: N-butyl-2-cyanoacrylate (Histoacryl; B. Braun Dexon GmbH, Spangenberg, Germany) has been successfully used to treat an esophagojejunal anastomotic leak after total gastrectomy. 18 Bianchi Cardona et al. reported two successful cases of cervical esophagogastric anastomotic fistulae treated with cyanoacrylate glue. 19 Ojima et al. reported successful use of alpha-cyanoacrylate monomer in four patients with aortoesophageal fistula, esophagogastric anastomotic leak, and perforation of colon conduit after esophagectomy. 20 Four to six applications were needed to close the fistulae in these patients, performed in 1–2-week intervals.
Fibrin glue use has been reported in enterocutaneous fistulae with promising results.21,22 It has also been used to close esophageal fistulae either by fistula embolization or by submucosal injection into the edges of the fistula.23,24 The glue is repeatedly injected into the submucosa until the lumen is occluded. Other options include combining an absorbable mesh with fibrin glue application for larger fistulae. After the mesh is placed over the defect, fibrin glue is applied under endoscopic guidance. Repeated applications may be needed until the defect completely epithelializes.
Bohm et al. reported complete healing among 13/15 patients treated with this technique. 25 Other small case series have reported high closure rates with the use of fibrin glue for esophageal perforations and anastomotic leaks. 26 Fibrin glue has been reported to seal esophagobronchial fistulae by either direct embolization or fistula wall injection both in adults and children.23,27,28
Currently, no comparative data exist to support the use of one sealant over the other. Also, the optimal fistula size for successful treatment of esophageal perforations or anastomotic leaks is unknown. More than one application is often needed for compete fistula closure. Formation of a well-established fistula tract seems crucial for the success of this technique. In our case, the fistula diameter was reduced to 5 mm after only 8 days of EVAC therapy, and a single application of fibrin glue was required to seal off the fistula.
Covered self-expanding stents
Covered self-expanding metal and plastic stents have been used with high success rates for esophagogastric anastomotic leaks. Better results were reported with intrathoracic rather than cervical anastomotic leaks. 29 Dasari et al. reported a systematic review of success rates and complications with use of covered self-expanding stents for anastomotic leak and benign perforations. 30 Cumulative technical and clinical success rates of stenting were 91% and 81%, respectively, with a mean of 1.34 stents per patient. Overall stent migration was 20%, and was higher among plastic stents (27% vs. 11%, P < .05). Other complications reported were bleeding and stent perforation (2%). Duration of treatment was highly variable and ranged from 4 to 16 weeks. A higher rate of postprocedural strictures was found with metal stents (n = 9 vs. 1, P < .05).
Freeman et al. retrospectively analyzed stent failures among 187 patients. 31 Stent migration rate was 27%. No other stent-related compilations were reported. Stent failures occurred among 8% of patients who eventually required an operative repair. A comparison of the two patient groups identified several risk factors for stent failure: cervical esophageal leak, gastroesophageal junction leaks, esophageal injury longer than 6 cm, or a conduit leak.
Stent migration remains a major issue with esophageal stents, and migration rates up to 40% have been reported. 32 Repositioning is not always successful and stents may need to be replaced when they migrate. Several techniques have been used to prevent stent migration with various success rates. Vanbiervliet et al. 33 described application of 2–4 endoscopic clips to the proximal end of the stents. The clips were placed in 23 of 44 patients. They reported an overall 34% stent migration, but only in 3 of the 23 patients (13%) with clips, with an odds ratio of 2.3 to prevent stent migration.
Wang and Lou found similar results in a randomized controlled study of stents placed for malignant esophageal strictures. 34 Other methods of preventing stent migration include endoscopic suturing of the stent in place 35 or application of an OTSC to anchor the proximal end of the stent, 36 even though removal of the clip may require advanced endoscopic techniques. 37
In the case we present, the stent placed migrated shortly after placement, thus creating an angle between the proximal end of the stent and the esophageal wall, preventing complete occlusion of the leak. We did notice a reduction of the internal fistula size after 3 weeks of stent treatment even with an incomplete seal.
Over-the-scope clips
In the past, endoscopic through-the-scope clips (TTSC) application has been used as an endoscopic treatment option for small anastomotic leaks or fistulae of the upper GI tract. These clips were originally designed for endoscopic bleeding control. Only small case series were reported with these clips.38,39 The limitations of TTSC are their small size and low compression force. OTSC (Ovesco Endoscopy AG), on the other hand, are an effective treatment for GI leaks and fistulae. 40 Its “bear claw” configuration provides a full-thickness closure of the wall as opposed to regular endoscopic clips. Before the clip is applied, the lesion is sucked into a clear cap. In cases of a more fibrotic tissue, a through-the-scope anchor can be used to pull and hold the tissue in place (Ovesco anchor, twin grasper, or endoscopic forceps). The clip in then applied over the tissue.
Haito-Chavez et al. reported a multicenter retrospective study of the results of OTSC in closure of GI defects. 41 A total of 188 patients (108 fistulae, 48 perforations, and 32 leaks) were included in the study. They found a significantly higher success rate in closure of perforations (90%) and leaks (73.3%) compared to fistulae (42.9%) (P < .05), and higher closure rates when OTSC were used as the primary therapy rather than rescue. Several case reports and small case series have been reported on the use of OTSC for esophageal perforations and anastomotic leaks.42,43
Mennigen et al. reported a systematic review of the results of OTSC for GI perforations. 44 A total of 301 patients were included in their analysis. Of these, 186 patients had OTSC placed for upper GI perforations and 94 for colorectal perforations. Overall success rate was 73% with 1.3% complication rate. Overall success rate was higher for acute iatrogenic perforations (90%) compared to anastomotic leaks (68%) or fistulae (59%). Success rates were similar among upper GI perforations (73%) and colorectal perforations (78%). Four complications were reported: one detached clip with late surgical intervention, esophageal perforation during system introduction, and two cases on misplaced clip occluding the lumen, necessitating surgical intervention. Misplaced clips may be occasionally removed endoscopically with iced saline application. 45 These clips are made of nitinol, and at temperatures below 10°C, the clip becomes malleable allowing endoscopic removal. Other options include Yttrium Aluminum Garnet laser or argon, 46 submucosal injection, and snare grasping 47 or Ovesco remOVE system.
Applying an OTSC is challenging in the case of an anastomotic leak following esophagectomy for two reasons: first, considering that the diameter of the applying device of the clip is quite large, traversing the anastomosis at an early stage following surgery may be impossible; second, the application cap should ideally be placed en face of the perforation, which can be quite challenging in the esophagus due to its small diameter.
In the case we present, the clip was misplaced probably due to the immobile edge of the esophageal margin and the mobile conduit wall on the opposite side of the fistula opening, causing suctioning of the conduit walls into the suction cap. This led to misplacement of the clip fully occluding the conduit lumen. It was removed using the Ovesco remOVE system after failure to remove with iced saline and argon as recommended by the manufacturer.
Operative management
Mediastinal anastomotic leak is the most important complication after esophagectomy. Surgery is the mainstay of treatment for patients in whom expectant of endoscopic management is unsuitable, especially among patients who develop sepsis or uncontrolled leak. Surgical exploration is mandatory in these patients, and may include irrigation, debridement of necrotic tissue, decortication of the lung, and wide drainage. Reanastomosis or primary repair is possible in selected cases; others may require esophageal diversion. 48 Lee et al. 49 compared surgical to conservative management of anastomotic leaks among 663 patients after esophagectomy. Leak was diagnosed in 23 patients: one patient died, 13 were managed conservatively, and 9 underwent surgical exploration. Primary closure was feasible in five patients. Fistula closure time was shortest among patients who had primary repair of the anastomosis compared to surgical exploration alone of conservative management (36.2 ± 34.5, 67.5 ± 92.2, and 84.0 ± 113.7 days respectively). Timely intervention is essential to decrease mortality and improve outcome of this devastating complication.
Conclusions
Modified EVAC, in which a small caliber NG tube is passed through an existing tract, is feasible and safe with several advantages compared to conventional EVAC methods, allowing easier placement and providing the patient with the ability to continue oral intake during treatment. The residual fistula equaling the size of the NG tube used can be easily occluded with tissue sealant.
Authors’ Contributions
All authors have contributed significantly to the drafting, reviewing, and final approval of this article.
Footnotes
Disclosure Statement
No competing financial interests exist.