
Abstract
Abstract
Background:
Spigelian hernia (SH) is a rare entity, but its surgical treatment is essential because of its high complication risk. Laparoscopic approaches have become the option in elective surgery because it has less morbidity and requires a shorter stay. Several laparoscopic techniques have been employed, but there is no gold standard technique for this kind of hernia. We report, in this study, our experience with intraperitoneal onlay mesh (IPOM) repair.
Materials and Methods:
Fifteen patients underwent elective surgery for SH between 2008 and 2015 in a Short-Stay Surgical Unit. Laparoscopic IPOM technique was performed in all patients. The technique, epidemiological data, operative findings, hospital stay, morbidity, and follow-up are presented.
Results:
Fifteen patients (8 males) with a median age of 57 years were operated on. They commonly presented an abdominal mass in the flank (73.3%). Computed tomography was necessary in 4 patients to complete preoperative diagnosis. The mean operating time was 43 minutes. No closure of the defect was associated and we employed expanded polytetrafluoroethylene-coated and polyvinylidene fluoride-coated polypropylene meshes. There were no postoperative complications and early discharge was possible in all cases. No recurrences or complications related to the mesh have been detected so far, with a median follow-up of 4 years (1–8).
Conclusions:
Our experience shows IPOM laparoscopic SH repair is a safe and effective technique with advantages that allow us to recommend it as the most advisable for SH treatment in Short-Stay Surgical Units. However, current controversies in the use of intraperitoneal meshes must be clarified.
Introduction
T
Because of its high complication risk, the treatment of SH is surgery. Traditionally, SH has been repaired by an open technique. Laparoscopic hernia repair has become increasingly more popular and it is associated with some advantages, such as a minimal postoperative morbidity, a shorter convalescence period, and an acceptable recurrence rate. 2 These characteristics are essential components of the major outpatient surgery. Since 1992, when Carter and Mizes 3 described their laparoscopic technique, several procedures have been developed in the treatment of SH. It can be repaired laparoscopically by total extraperitoneal (TEP), transabdominal preperitoneal (TAPP), or intraperitoneal onlay mesh (IPOM) technique. But to date, there is no gold standard laparoscopic technique for this kind of hernia.
The aim of this study was to assess the safety, efficacy, and potential benefits of IPOM repair for SHs in an Outpatient and Short-Stay Surgery Unit.
Materials and Methods
A retrospective review of all laparoscopic SH repairs by IPOM technique carried out at our institution between January 2008 and December 2015 was performed. All patients were diagnosed preoperatively and surgery was performed in an elective setting. All patients were included in a follow-up program and are requested to attend a specific hernia consultation after 4 weeks, 6 months, and each year. We evaluated subjective outcomes and physical examination. Radiological imaging only was performed if symptoms or signs of complication were present. These patients were identified from a prospective database and were retrospectively analyzed. The following aspects were evaluated: demographic data, site of the defect, diagnostic methods, operative time, postoperative complications, hospital stay, and recurrence rate.
The IPOM procedure was carried out with the patient placed in a supine position with both arms adducted. Pneumoperitoneum was obtained using Veress needle in the contralateral flank region of the hernia and by inserting a 10-mm port at the mid clavicular contralateral line. Diagnostic laparoscopy was then performed (Fig. 1). Two further 5-mm ports were placed on the contralateral hypochondrium and iliac fossa of the defect.
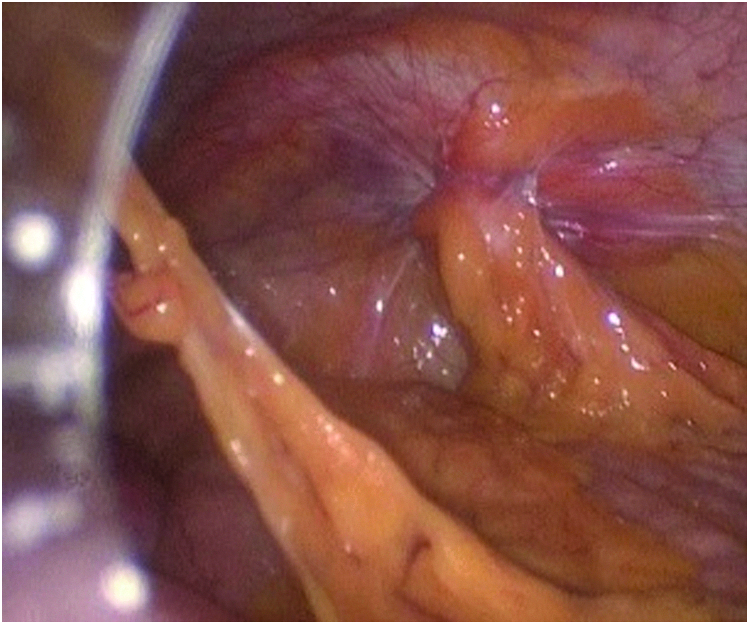
Intraoperative views of a patient presenting with right Spigelian hernia.
The hernia defect was identified and its contents reduced using sharp dissection. Primary closure of the defect was not performed. The size of the mesh was determined by the defect size and a 5 cm overlap; these marks were painted over the skin (Fig. 2). The mesh was positioned over the defect intraperitoneally, and then, with an external needle inserted through the painted marks, it was anchored to the abdominal wall (Fig. 3). Once the mesh was fully extended, it was tacked with multiple absorbable tacks. We inserted two circular lines of tacks around the defect (double crown technique) (Fig. 4). These maneuvers enabled us to better define the defect size, select the appropriate mesh size, and cover the whole defect.

Measuring of the defect and marking the 5 cm overlap on the skin.
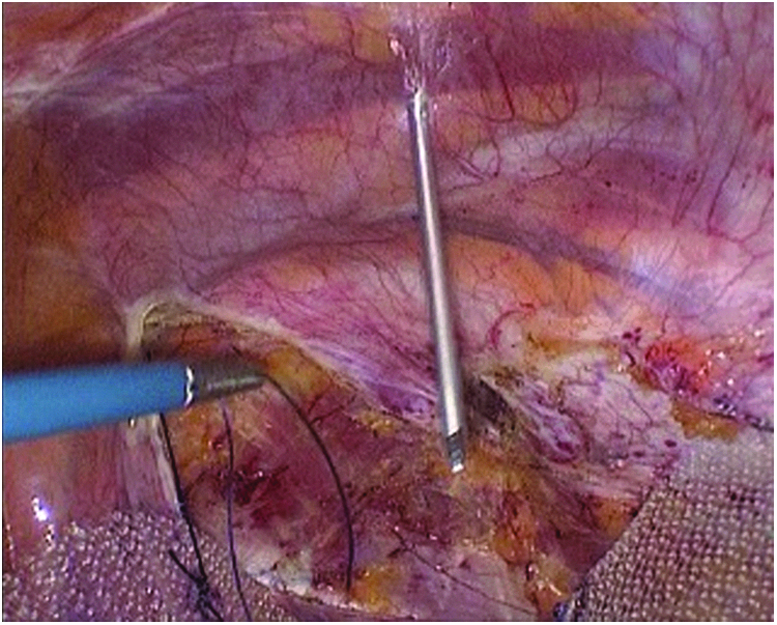
Method to extend mesh: needle introduced through the skin mark that is removed adjusting the mesh equidistant 5 cm from the defect.
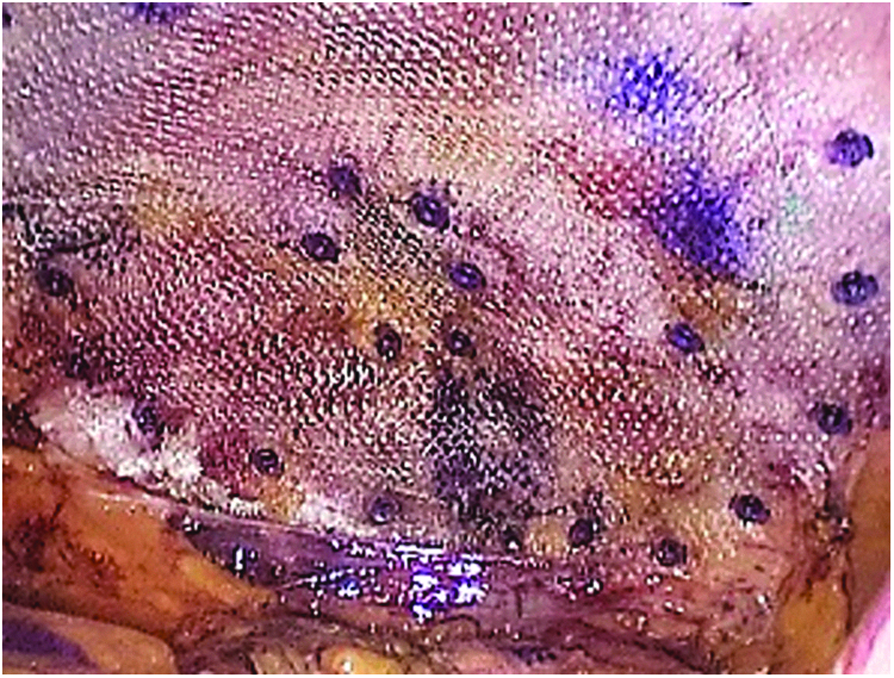
Double crown of tacks fixing the mesh.
Results
Between January 2008 and December 2015, 15 patients underwent laparoscopic SH repair by IPOM technique. The mean patient age was 57 years (range 26–78). Eight patients (53.3%) were men. With respect to hernia location, the SH was right sided in 8 patients (53.3%). No patient had bilateral SH. One patient had SH associated with a contralateral inguinal hernia. Of these, 62.5% of patients presented risk factors, such as obesity (n = 2), chronic pulmonary disease (n = 1), and previous abdominal surgery (n = 5). The median American Society of Anesthesiologists (ASA) grade was 2 (12 patients), with the majority being ASA 1 or 2. Table 1 shows main characteristics of the patients diagnosed with SH. Among the previous surgeries, a left inguinal hernia was repaired by laparoscopic TEP approach in 1 patient, 2 patients had a history of cesarean sections, one of laparoscopic cholecystectomy, and another of laparoscopic prostatectomy.
All patients were diagnosed preoperatively. Most of them (67.7%) had a hernia on examination and 5 patients presented flank pain as the main complaint. In 4 patients, computed tomography (CT) scanning of the abdomen was required to confirm diagnosis of SH or rule out other abdominal wall defects, overall in patients with previous surgery.
Surgery was carried out laparoscopically using IPOM technique and there were no conversions to an open repair. The mean operative time was 43 minutes, with the range between 30 and 70 minutes. There were no intraoperative complications. In 7 patients, the composite mesh used was a prosthetic that comprised of polypropylene (PP) and expanded polytetrafluoroethylene (ePTFE) (108 g/m2, Relimesh; Herniamesh, Chivasso, Italy) and in 8 patients, a polyvinylidene fluoride (PVDF)-coated PP mesh (108 g/m2, Dynamesh-IPOM; Dahlhausen, Cologne, Germany) was employed. The mesh was always placed to overlap widely the defect circumferentially (5 cm) and fixed only with tacks with double crown technique. There were no postoperative complications and all patients were assessed the next morning and discharged. There were no readmissions related to SH repair. At postoperative follow-up, all patients were pain free and recurrences have not been detected so far, with a median follow-up of 4 years (1–8). CT scans were not needed in the follow-up due to the lack of subjective impressions, symptoms, or physical signs of complication. No patient has developed symptoms of bowel obstruction or mesh infection and mesh explant has not been required in any patient.
Discussion
SH represents a low-incidence occurrence. Its unspecific symptoms and difficult detection by physical examination make early diagnosis difficult. Both reasons explain why the elective procedure of SH has not yet been standardized and why the elective SH repair series reports a limited number of patients. Although some reports describe 50% of cases of SH discovered incidentally at laparoscopy, 4 a comprehensive clinical history and thorough physical examination provides the diagnosis in 74% of cases, 5 similar to our series. CT has been reported to be the most reliable test to confirm the diagnosis, 6 and it was required to confirm the final diagnosis in 4 cases.
SH may remain undiagnosed until emergency surgery is required. Given the high rate of incarceration/strangulation, its diagnosis is an indication for elective surgical repair. 7 The surgical options for repair vary from the open repair to the laparoscopic hernia repair. Open procedure with primary suture repair has reported a recurrence rate of 4%, 8 whereas the mesh repair achieves a less recurrence rate (until 0% in some series). 9 Furthermore, laparoscopic surgery has consolidated its role in treating abdominal wall hernias. Some reports reflect the advantages of laparoscopic repair versus open repair. Moreno Egea et al. 10 developed a comparative, randomized study between open repair and TEP in SH repair, which revealed that the laparoscopic repair group had significantly less morbidity and shorter hospital stays.
Among the laparoscopic techniques, the same procedures developed to repair inguinal hernias have also been used in SH repair: TEP, TAPP, and IPOM. Each of the three techniques has its advantages and disadvantages. TEP is technically more demanding, it requires specific equipment, and longer operating time. However, it avoids entry into the peritoneal cavity, there is no risk of intraabdominal lesions during the procedure, and prosthesis does not contact with the bowel minimizing the development of adhesions. 11
TAPP and IPOM are intraabdominal laparoscopic approaches; both offer a precise location of the defect, access to the peritoneal cavity and to the content of the hernia, and a learning curve that is lower than in TEP technique. However, separating a flap or peritoneal pocket that covers the mesh makes usually TAPP procedure difficult in SH repairs. It requires longer surgical time and greater experience in abdominal wall surgery than IPOM, in which it is simple to extend the mesh properly and attach it. 12 In addition, both approaches offer the possibility of concomitant treatment of other abdominal wall defects, such as an inguinal hernia. In fact, 1 patient with SH also had a contralateral inguinal hernia, and the IPOM technique let us repair both pathologies.
The latter two techniques are usually related to the potential risk of intestinal lesions and a complete reperitonization is required to avoid adhesions and other complications because of the intraabdominal location of the mesh. 13 In fact, a PP mesh must only be used in TAPP when the flap that covers the mesh is a firm tissue, separated without fissures, and will allow reperitonization with safety. Otherwise, it is safer to use a composite mesh.
Nowadays, a wide range of composite meshes are available. Nearly all of them use PP, polyester (PE), and ePTFE and combine them with each other or with additional materials such as titanium, omega 3, PVDF, or hyaluronate. But, it appears that there is no ideal synthetic material, and all of them may have a disadvantage, making the choice of an optimal replacement graft difficult. 14 We show a literature review of the different mesh types employed in the laparoscopic repair of SH (Table 2).
IPOM, intraperitoneal onlay mesh; PE, polyester; PP, polypropylene; TAPP, transabdominal preperitoneal; TEP, total extraperitoneal.
Porosity is the main determinant of tissue reaction; large pores allow cellular infiltration and soft tissue integrity. Weight is another factor, and it depends on the pore size; light-weight meshes produce less foreign body reaction and are more elastic. Nevertheless, a macropore mesh may result in a disorganized neoperitonealization and therefore can cause potentially more adhesions. Theoretically, a macroporous mesh is needed against the parietal peritoneum and a micropore side against the viscera. 15 On the other hand, some reports insist currently on the importance of the mesh structure and affirm that the reticular-type structure will always induce adhesions because of an irregular mesothelization. 16 An actual controversy remains about the use of composite meshes: is it a wrong option to use a composite mesh when its visceral side is reticular, as in PVDF-coated or poliglecaprone-coated PP meshes? On the one hand, there are reports with good results in their intraperitoneal use in studies with animals, case series, and randomized studies,17–21 but some studies provide information about the risk of complications with this type of meshes.22–24
In our study, we have employed ePTFE-coated PP mesh and PVDF-coated PP mesh with no problems and no patient has developed bowel obstruction or intestinal fistula. To our knowledge, in the published series about elective laparoscopic treatment of SH, complications related to the mesh are not described with a median follow-up of 4 years, as in our patients. These studies include intraabdominal techniques and several types of intraabdominal meshes.
Among these studies, in 2014 Moreno Egea et al. 10 compared the results of the TEP approach with the IPOM approach in laparoscopic SH repair involving 16 patients. IPOM technique was carried out in 9 of them, using a titanium-PP coated mesh with an operative time of 30 minutes and without complications related to the mesh. In 2015, Kelly et al. 5 performed a review of all laparoscopic SH repair that involved 40 patients; 25 of them had an intraperitoneal repair using PP and poliglecaprone or PE with polyethylene glycol–glycerol meshes and no complications related to the mesh were described (Table 2).
Recurrence rates of SH have been similar among laparoscopic approaches, 25 and we have not reported any recurrence employing IPOM technique. The use of mesh, regardless of the size of the defect, may have influenced these results. However, we believe that the risk of recurrence depends on other factors too, such as factors associated with the patient or with a poor technique. We consider it is essential that the mesh can be well extended, overlapping the defect more than 5 cm, and without the closure of the defect to make perform a tension-free procedure. Furthermore, we attach the mesh with double crown of tacks to extend the mesh completely, avoiding contact between the parietal side and the bowel.
IPOM technique has been recommended as the “gold standard” technique in SH repair because of the technical and economic advantages. 26 From our experience, we recommend the IPOM as a safe and effective technique in SH repair. Moreover, it presents characteristics appropriate to an Outpatient and Short-Stay Surgery Unit, with less morbidity and early discharge. However, the current controversies in intraabdominal meshes must be clarified to offer the best solution to patients.
Footnotes
Disclosure Statement
No competing financial interests exist.