
Abstract
Abstract
Background:
Laparoscopic liver resection (LLR) for lesions adjacent to major vessels was still associated with difficulty and challenge. This study aimed to compare outcomes after LLR and open liver resection (OLR) of lesions adjacent to major vessels.
Materials and Methods:
A retrospective analysis of patients with hepatic tumors close to main or second branches of Glisson's tree, to the major hepatic vein, or to the inferior vena cava within 1 cm between January 2015 and January 2017 was performed based on the propensity score matching (PSM) method. Perioperative and oncological outcomes were then evaluated.
Results:
A total of 64 patients underwent LLR and 86 patients had OLR. After 1:1 PSM, well-matched 40 patients in each group were obtained. The operative time (240 versus 210 minutes, P = .012) in the LLR group was significantly longer than that in the OLR group, whereas blood loss (200 versus 400 mL, P = .003) was less in the laparoscopic group. The median hospital stay for LLR (6 versus 8 days, P = .032) was shorter than for the open procedure. No statistical differences was noted according to overall postoperative complications, but the OLR group tended to be vulnerable to more severe complications. For patients with hepatocellular carcinoma, the comparable oncological results in terms of 2-year overall survival (P = .898) and disease-free survival (P = .992) were observed.
Conclusions:
LLR for tumors adjacent to major vessels appears to be feasible and safe in selected patients. LLR is associated with less blood loss, shorter hospital stay, and similar oncological outcomes compared with OLR.
Introduction
L
By 2014, the second International Consensus Conference for Laparoscopic Liver Resection recommended that laparoscopic minor liver resections should be considered a standard practice in surgery, whereas laparoscopic major liver resection is only confirmed to be an innovative procedure that was still burdened with some unknown risks. 5 In the meantime, the difficulty scoring system for LLR was introduced and elaborated by a combination of the extent of liver resection, tumor location, tumor size, liver function, and proximity to major vessels. 6 Resections for major extent, posterior-superior segments, large lesions as well as lesions close to major vascular were associated with a high score and a steep learning curve, hence limiting the wide dissemination of laparoscopic techniques.
Over the past few years, the indications for laparoscopic hepatectomy have gradually expanded as the rapid development of laparoscopic devices and surgical experience. Accordingly, many centers have attempted to carry out more challenging laparoscopic procedures with reported favorable both short- and long-term outcomes of LLRs for major resections, posterior-superior segment resections, large or giant lesion resections, and background of liver cirrhosis.7–14 However, for lesions adjacent to the main and second branches of Glisson's tree, to the major hepatic vein, or to the inferior vena cava, laparoscopic procedures are associated with more risk and currently published data regarding these special cases are scarce, making the LLR for lesions proximate to major vessels remaining an unsolved problem.15,16
Therefore, this study was introduced and aimed to analyze the surgical and oncological outcomes of LLR for lesions adjacent to major vessels compared with conventional OLR.
Materials and Methods
Study design
From January 2015 to January 2017, all patients with hepatic tumor lesions adjacent to major vessels who received curative liver resection in West China Hospital were retrospectively enrolled from a prospectively collected database. Inclusion criteria were as follows: (1) male or female patients aged 18–75 years, (2) Child–Pugh class A or B liver function, (3) tumor close to the main or second branches of Glisson's tree, to the major hepatic vein, or to the inferior vena cava within 1 cm, and resection with preservation of such vessels, (4) a 15-min indocyanine green retention rate ≤10% for patients with liver cirrhosis, and (5) Eastern Cooperative Oncology Group (ECOG) score 0 or 1. 17 The exclusion criteria were (1) repeat liver resections, (2) hepatic resection combined with other abdominal organ resections except for gallbladder, (3) presentation of extrahepatic metastases for malignant lesions, and (4) severe dysfunction of the heart, lung, kidney, or other organs.
Patients were divided into LLR and OLR groups according to the different surgical procedure received. Preoperative evaluations were essential for both groups and included liver function test, tumor maker test, routine blood test, coagulation function test, as well as the three-phase-enhanced computed tomography, or magnetic resonance imaging scans. This study was approved by the Committee of Ethics in West China Hospital of Sichuan University.
Surgical procedure
The types of liver resection were defined based on the Brisbane 2000 classification. 18 The detail of the laparoscopic procedure has been described previously.19,20 In general, all patients under intravenous general anesthesia were placed in the left lateral decubitus position with operator standing on the right side and assistant surgeon and scopist on the left side of the patient. A Veress needle was then inserted to establish pneumoperitoneum and the intraabdominal pressure was maintained at 13 mmHg. A 12-mm periumbilical port was used for the 30° rigid laparoscope whereas the other four upper abdominal ports (two 12-mm and two 5-mm trocars) were applied for main operation. After full mobilization of the liver, laparoscopic ultrasonography was performed to confirm lesions' position with major vasculature and guide transection line (Fig. 1A). Superficial parenchyma dissection was done by harmonic scalpel (Ethicon Endo-Surgery), whereas deeper tissue was accomplished by a combination of harmonic scalpel, laparoscopic cavitron ultrasonic surgical aspirator (CUSA; Valleylab, Inc.), and Ligasure (ValleyLab, Inc.) (Fig. 1B). To control surgical blood loss, the intermittent Pringle maneuver was applied with a clamp time of 15 minutes and then 5 minutes unclamped (Fig. 1C). Small vessels were controlled by Hem-o-lock clips or titanium clips, whereas the main hepatic veins or Glisson pedicles were all secured by the laparoscopic linear stapler (Fig. 1D). After surgery, the resected liver was then placed into a specimen bag and removed from an enlarged port in the upper abdomen or the suprapubic transverse incision (Fig. 1E, F). Peritoneal drainage tubes were routinely applied on the cut surface.
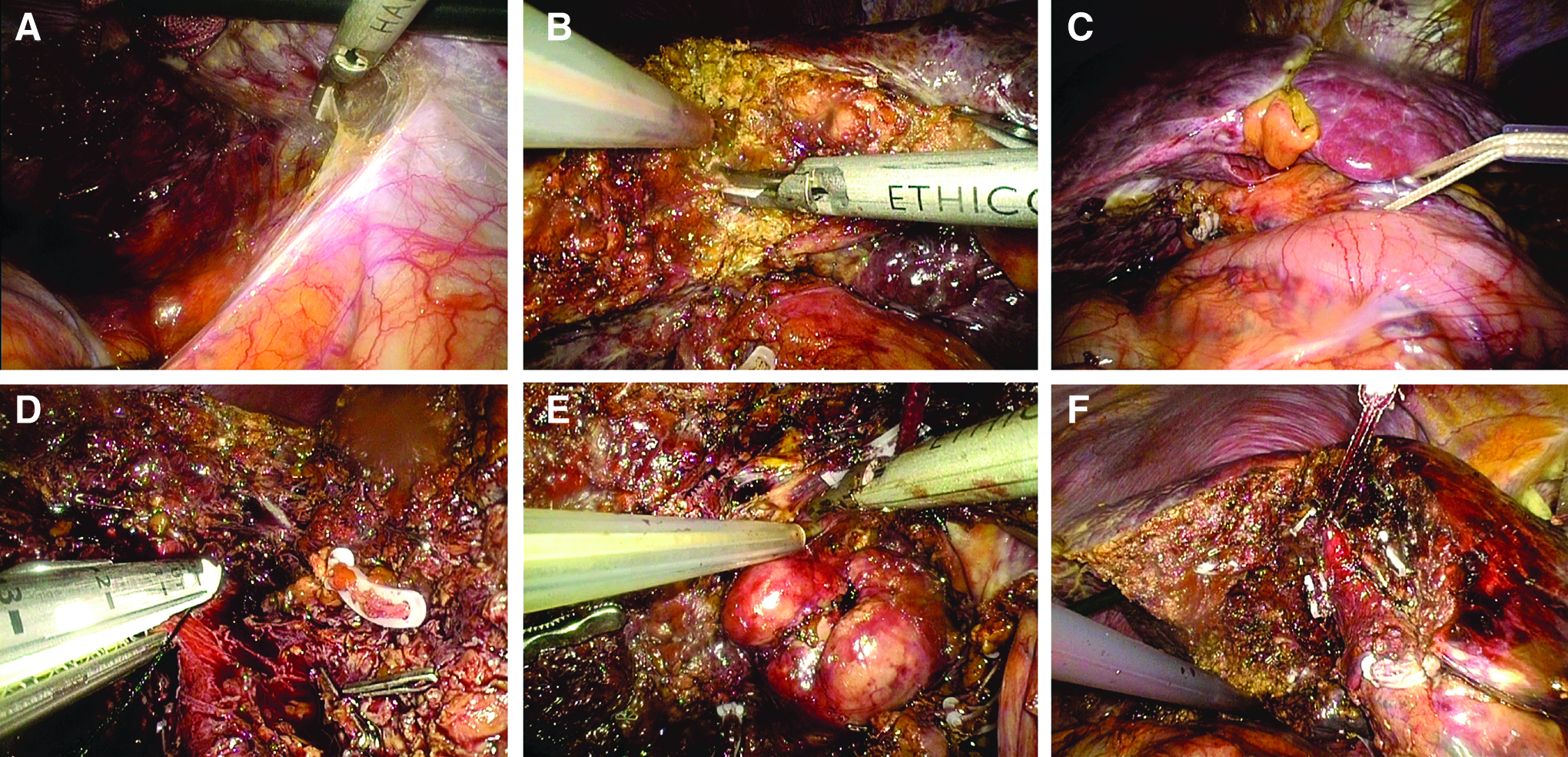
Surgical procedure.
For open procedure, a right subcostal incision was performed with the patients placed in supine position. The surgical strategy was similar to LLR with the clamp crushing and CUSA as the main methods for parenchymal dissection. Pringle maneuver was usually applied and the central venous pressure was maintained <5 mm Hg during liver resection.
Postoperative care and clinical outcomes
Postoperative evaluations of patients who received liver resection included routine blood test, liver function test, as well as coagulation function test on postoperative days 1, 3, 5, and 7. After it was confirmed that there was no abdominal fluid collection by an ultrasound imaging, the peritoneal drainage tubes were then removed.
Postoperative complications were classified by the Clavien–Dindo grade with the major complication defined as Clavien–Dindo ≥3 and then compared according to the comprehensive complication index (CCI).21,22 Liver failure was determined by the “50–50 criteria” on postoperative day 5. 23 Postoperative hemorrhage was defined according to the drop in hemoglobin level >3 g/dL postoperatively compared with the postoperative baseline level and/or any postoperative transfusion of packed red blood cells for a falling hemoglobin. 24 Ascites was identified by the postoperative daily drainage >10 mL per kilogram of body weight. 25
Statistical analysis
To overcome patients' selection bias from a retrospective nature, the propensity score matching (PSM) method was applied through the one-to-one nearest-neighbor matching strategy without replacement using a 0.2 caliper. The factors enrolled into the PSM model were as follows: age, body mass index (BMI), preoperative liver function, American Society of Anesthesiologists (ASA) classification, indications for resection, previously abdominal operation history, comorbidities, lesion size, and location.
Continuous data were expressed as median with range and analyzed based on Mann–Whitney U test and Wilcoxon rank test before and after PSM, whereas categorical variables were expressed as number with percentage and compared using Chi-square test and McNemar's test before and after PSM. Overall survival (OS) and disease-free survival (DFS) were compared by the Kaplan–Meier method and analyzed based on the log-rank test. Two-tailed P < .050 was considered statistically significant. All analyses were performed with SPSS version 22.0 (IBM SPSS, Inc., Chicago, IL).
Results
Baseline characteristics
A total of 150 patients meeting the inclusion and exclusion criteria were enrolled in this study. Of which 64 were in the LLR group and 86 were in the OLR group. Baseline characteristics of all patients are shown in Table 1. Before PSM, the ASA grade (P = .027), types of tumor (P = .036), and lesion size (4.8 versus 6.0 cm, P < .001) were significantly different between the 2 groups. After finishing the PSM, both LLR and OLR groups have 40 patients left but the baseline demographics were well balanced.
ASA, American Society of Anesthesiologists; BMI, body mass index; COPD, chronic obstructive pulmonary disease; CRLM, colorectal liver metastasis; HCC, hepatocellular carcinoma; ICC, intrahepatic cholangiocarcinoma; LLR, laparoscopic liver resection; NCRLM, noncolorectal liver metastasis; OLR, open liver resection.
Surgical characteristics
The extent of resections of LLR and OLR groups included tumorectomy (n = 6 versus n = 8), segmentectomy (n = 2 versus n = 7), left lateral sectionectomy (n = 3 versus n = 3), left hepatectomy (n = 8 versus n = 4), right anterior sectionectomy (n = 2 versus n = 5), right posterior sectionectomy (n = 9 versus n = 4), and right hepatectomy (n = 10 versus n = 9), respectively. The major vessels involved in LLR and OLR groups included right hepatic vein (n = 13 versus n = 11), middle hepatic vein (n = 13 versus n = 13), left hepatic vein (n = 3 versus n = 3), right anterior portal pedicle (n = 3 versus n = 5), right posterior portal pedicle (n = 2 versus n = 2), right portal pedicle (n = 3 versus n = 5), and left portal pedicle (n = 3 versus n = 1), respectively.
The operative time (240 versus 210 minutes, P = .012) in the LLR group was significantly longer than that in OLR group. However, blood loss (200 versus 400 mL, P = .003) was less in the LLR group than in the OLR group. No statistically significant differences were noted in terms of Pringle time (40 versus 30 minutes, P = .138), transfusion requirement (5.0 versus 15.0%, P = .289), and surgical margin (3.2 versus 2.9 mm, P = .711), respectively. The conversion was encountered in 1 case due to the severe adhesion in laparoscopy (Table 2).
Postoperative outcomes
The postoperative outcomes are shown in Table 3. The median postoperative hospital stay (6 versus 8 days, P = .032) was shorter in the LLR group. The overall complication rates (17.5 versus 22.5%, P = .500) in terms of liver failure, postoperative hemorrhage, ascites, pneumonia, pleural effusion, and wound infection were comparable between LLR and OLR groups. However, major complications were observed only in the OLR group and included 2 patients with refractory ascites treated by abdominal paracentesis and 1 patient suffering from hemorrhage received relaparotomy to stop bleeding. When calculated by CCI (0 versus 0, P = .046), statistically significant difference in postoperative morbidity was noted.
Oncological outcomes
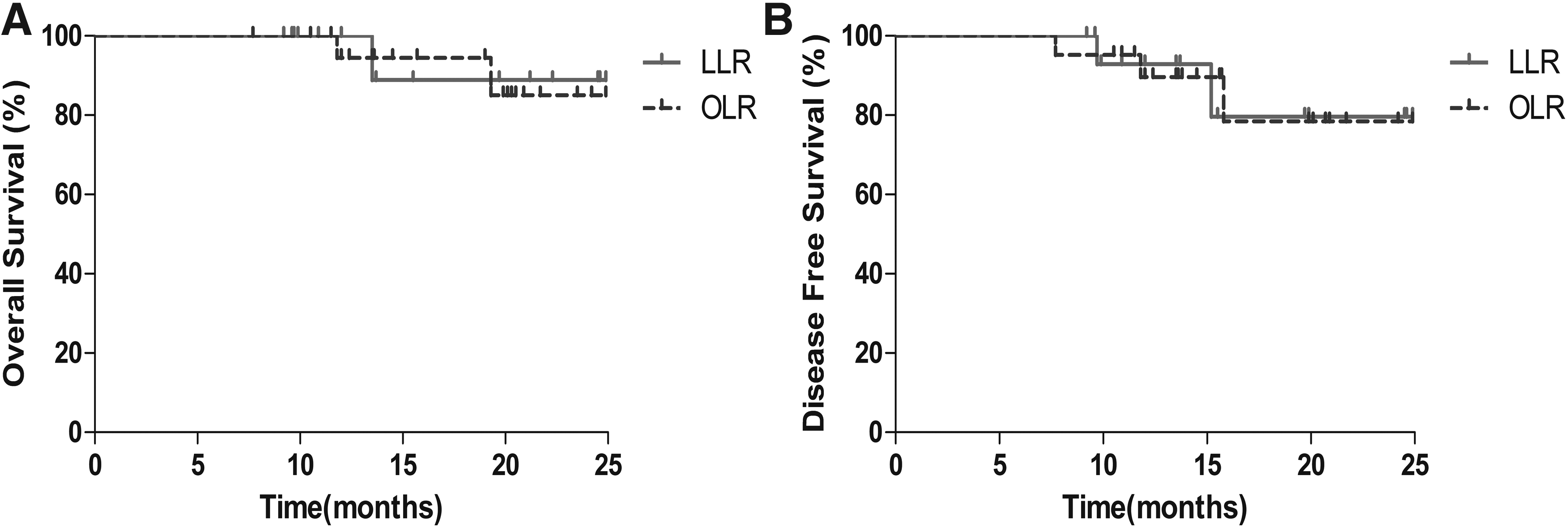
For hepatocellular carcinoma (HCC) patients enrolled in both groups, the oncological outcomes regarding OS (P = .898) and DFS (P = .992) were comparable with the median follow-up time of 13.8 (7.7–24.9) months. The 1- and 2-year OS rates were 100.0% and 88.9%, respectively, in the LLR group, and 94.4% and 85.0%, respectively, in the OLR group (Fig. 2A). The 1- and 2-year DFS rates were 92.9% and 79.6%, respectively, in the LLR group, and 89.6% and 78.4%, respectively, in the OLR group (Fig. 2B).
Discussion
Although surgical devices and experience of laparoscopy have gradually improved, LLR for lesions proximate to major vessels, which is associated with high grade score in the difficulty scoring system, remains technically challenging and data focusing on this special cohort of patients are limited in current literature.15,16 In this study, comparison between LLR and OLR for hepatic tumors close to major vessels was introduced and the superior perioperative outcome and comparable oncological outcomes of LLR were observed.
The baseline characteristics of the original 2 groups showed significant differences in terms of ASA grade, types of tumor, and tumor size, which were considered as obvious factors that would influence surgeons' preferences for different surgical procedures. Analysis based on such baseline data will no doubt be misjudged. Therefore, the PSM method was applied based on the aforementioned factors to overcome patients' selection bias arising from lack of randomization. Moreover, for other factors including age, BMI, preoperative liver function, previously abdominal operation history, comorbidities, and tumor location, even though the statistically significant differences between 2 groups were not noted, they were also selected as matching factors for their potential influences on surgical procedure selection. Based on the well-matched 2 groups, the surgical and oncological outcomes of LLRs were then evaluated.
In this study, less blood loss and less proportion of intraoperative transfusion in the LLR group were observed. In general, for tumors adjacent to major hepatic veins or portal pedicles, the massive bleeding from injured vascular can be sometimes uncontrollable and lead to high conversion rates in laparoscopic surgery. 26 However, there was only 1 case of conversion of the LLR group that was caused by severe adhesion of the previously open cholecystectomy history. Usually, the full mobilization of the liver from retroperitoneum before parenchyma transection was applied in our center. Under the magnified view of laparoscopy, mobilization could be performed easier with energy devices, which may often require larger subcostal incisions in conventional OLRs. On occasion of hepatic veins injury, the full mobilized liver could be advantageous and help surgeons lift up the liver to reduce bleeding and earn time for reparation. In the mean time, maintaining a relatively low central venous pressure and the intimate cooperation between operator and assistants for effective suturing are of great importance to get vascular control. In addition, the use of Pringle maneuver can be advantageous to minimize bleeding from portal branches and help contribute a relatively clean surgical field for parenchyma dissection. Moreover, choosing the appropriate energy devices could facilitate the whole operation. Usually, we adopt CUSA and harmonic scalpel as the main tools for dissection, but for patients with cirrhotic background, Ligasure will be more often preferred. What is more, the special caudal-to-cranial vision of LLR facilitates the application of liver-hanging maneuver by using a laparoscopic Goldfinger dissector, which also serves as an effective way to decrease rates of hepatic veins or vena cava injury. Besides meticulous dissection of liver parenchyma by laparoscopic energy devices, laparoscopic ultrasonography did play a crucial role in LLR for its confirmation of lesions' position with major vessels and then guiding resection along such vulnerable vasculars.
In line with previously published data, longer operative duration in the LLR group was noted.13,27 For this relatively new surgical technique, a certain learning curve is existing, especially for more difficult cases of tumor proximate to major vessels, and will no doubt influence the surgeon's operative proficiency. In addition, the more precise manipulation during laparoscopic procedure and the routine use of Pringle maneuver may still be responsible for the prolonged surgical time.
With respect to postoperative morbidity, the LLR group shows outcomes comparable with those of the OLR group. When judging from the severity of postoperative complications encountered, the laparoscopic group yielded a better endpoint. Even though it failed to reach a statistically significant difference, LLR tended to be superior in postoperative pulmonary complications. In accordance with reported literature, laparoscopy decreases respiratory infection as well as symptomatic pleural effusion rates in patients undergoing liver resections. 28 Instead of a huge subcostal incision, LLR simply placed four or five trocars in the upper quadrant of the abdomen, which significantly decreased the destruction of respiratory muscles, thus contributing to a relatively fast postoperative rehabilitation. Moreover, patients who underwent laparoscopic surgery suffered less postoperative pain and got quicker out-of-bed activity, which also favors the recovery course. As a result, the median hospital stay in the LLR group was less than that of the OLR group, indicating the obvious advantages of laparoscopy.
For HCC patients enrolled in this study, the oncological outcomes were similar between the 2 groups. As it has been reported that intraoperative massive bleeding and transfusion requirement have a negative impact on postoperative recurrence, the laparoscopic procedure seems more beneficial.29,30 Considering the special tumor lesions that were close to major vascular structures, surgical margin can be sometimes of greater concern. For such instances, the use of laparoscopic ultrasonography could be more beneficial to overcome the lack of tactile sensation in laparoscopic surgery. Not just for the initial application of marking transection line, it should be also available during the whole operation whenever necessary to confirm lesions' position with major vasculature and thereby guiding transection. In this cohort of cases, all patients with HCC were pathologically confirmed for R0 resection and no local or port-site recurrence was observed during the 2-year follow-up. This may suggest that the laparoscopic technique for tumor proximate to major vessels could provide oncological results comparable with those of open procedure and in the same time yield a better cosmetic effect.
There are some limitations in this study. As a retrospective study, lack of randomization is the main shortcoming. Even though a randomized controlled trial could provide the most favorable evidence for clinical research, it is sometimes of great difficulty to carry out as the laparoscopic procedure is associated with a direct benefit of cosmetic presentation for patients and an obvious different cost of hospitalization compared with open surgery. To overcome this, the PSM method was applied according to several factors known may have an impact on patients' selection, and analysis based on the well-matched groups could then decrease the bias as much as possible. Moreover, the relatively small sample size and short follow-up time in patients with malignant lesions may still serve as an undeniable limitation. Further randomized controlled studies with larger sample size and single kind of tumor are warranted.
In conclusion, this study showed that LLR was associated with less blood loss, shorter hospital stay, lower severity of postoperative complications, and oncological outcomes comparable with those of OLR. LLR for tumors adjacent to major vessels appears to be feasible and safe in selected patients.
Footnotes
Disclosure Statement
No competing financial interests exist.