
Abstract
Abstract
Background:
Fluid therapy in the perioperative period varies greatly between anesthesia providers and may have a negative impact on surgical outcomes.
Methods:
We conducted a retrospective analysis of 705 elective colorectal cases consisting of colectomies, ileocolic resections, and low anterior resections at an academic institution from January 1, 2010 to May 29, 2015, collected by our electronic medical record before implementation of Enhanced Recovery After Surgery (ERAS®) pathways.
Results:
The mean for total crystalloid administration was 2578 mL with a standard deviation (SD) that was approximately 50% of the mean value. A combination of both normal saline and lactated Ringer's solution was used in almost all cases without a clear rationale for fluid choice. Fluid administered to patients was disproportional to measured intraoperative fluid losses (estimated blood loss and urine output) by a factor of 10. The average rate of fluid given was 1050 mL/h with an SD of nearly the same amount (951 mL). There was a variability of over 67% in total crystalloid administered based on both ideal body weight and total body weight.
Conclusions:
We found that a wide variability in the amount and type of fluid therapy administered existed at our institution before implementation of a colorectal ERAS pathway or routine use of goal-directed fluid therapy (GDFT). ERAS pathways with GDFT protocols could lead to more rational and consistent fluid therapy leading to improved outcomes.
Introduction
F
The application and utility of GDFT in clinical practice is an area of continued research and debate. 11 Many of the GDFT studies in the past 15 years utilize different types of hemodynamic monitors, hemodynamic variables, and fluid protocols, making it difficult to compare studies. 12 In addition, definitions for fluid management, including terms such as “restrictive” and “liberal,” are not consistent from study to study and change over time. Still, professional societies now encourage a rational fluid plan tailored to the individual patient. 13 GDFT has also been widely adopted as part of larger perioperative strategies to reduce surgical morbidity known as Enhanced Recovery After Surgery (ERAS®) pathways.14,15
ERAS pathways in colorectal surgery are well described in the literature, but similar pathways have also been developed for many other surgeries.15–18 The goal of an ERAS pathway is to reduce perioperative morbidity and improve return to baseline functional status with reduced cost and shorter length of stay.14–16,19 Preventable readmissions following colorectal surgery lead to increased morbidity and increased healthcare costs. 20 ERAS pathways favor achieving euvolemia during the perioperative period. Fluid overload leads to increased release of atrial natriuretic peptide, which leads to destruction of the vascular endothelial glycocalyx, the barrier preventing flooding of the interstitial space with fluid. 21 Fluid overload in elective colon surgery may lead to delayed return of gastrointestinal function and increased length of stay. 22 GDFT as part of an ERAS pathway offers a more standardized approach to fluid therapy and may be a useful tool to avoid wide variation in fluid therapy among providers. 23
Our hypothesis is that before implementation of ERAS pathways at our institution, there was a wide variability in the amount of fluid therapy administered to surgical patients undergoing colorectal surgery. We test this hypothesis in a retrospective analysis of fluid administration data before the implementation of ERAS pathways.
Materials and Methods
Data source
Study data were gathered from the electronic anesthesia information management system (MetaVision, Wakefield, MA) at one academic institution (Brigham and Women's Hospital, Boston, MA) from January 1, 2010, to May 29, 2015. The study period was defined by the time frame of utilization of the electronic anesthesia record system. Institutional review board approval was obtained for analysis of the data and exempted from the consent requirement due to the deidentified nature of the data.
For every surgical case abstracted from the electronic system, data were obtained regarding the patients' age, sex, American Society of Anesthesiologists Physical Status (ASA PS) classification, height, weight, surgical service, case duration, and type of fluid administered. Ideal body weight was calculated using the Devine formula. 24 For fluid administration, the data were segmented into total quantity in milliliters of fluid of lactated Ringer's solution, 0.9% normal saline, and Normosol (Hospira, Lake Forest, IL). Blood product administration was segmented into number of units of packed red blood cells, fresh frozen plasma, and pooled platelets. In addition, data on estimated blood loss (EBL) and UO were abstracted. The primary surgical procedure was coded using the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM), and reported as mapped to text values.
Inclusion and exclusion criteria
To provide the most specific focus on elective colorectal operations, the study group was limited to colectomies, ileocolic resections, and low anterior resections performed by our colorectal surgery service. This thereby excludes all colectomies performed in the setting of trauma and critical illness as these are commonly performed at our institution by our trauma surgery service. Cases were identified by the presence of the term colectomy, ileocolic or anterior resection in the mapped text values based on the ICD-9-CM codes recorded in the electronic anesthesia information management system. Cases were excluded if data were missing for any of the fluid variables or patient variables (age, height, weight, ASA PS classification). After inclusion and exclusion criteria, a total of 705 cases were included in the analysis. Incomplete reporting of laparoscopic or open surgical approaches was noted in the data and was therefore excluded from the analysis.
Statistical analysis
Patient demographic variables are reported as mean ± 1 standard deviation (SD). Fluid data reported as both the mean ± 1 SD and median/interquartile range due to a right tail in the distribution of data. All analyses were conducted using R Studio Version 0.99.491 (Boston, MA) and R Project for Statistical Computing, v3.2.3 (Vienna, Austria).
Results
Figure 1 shows the age, body mass index (BMI), and colorectal case duration for 705 elective colorectal surgeries (colectomies, ileocolic resections, and low anterior resections) at the Brigham and Women's Hospital in Boston, MA, before the implementation of a colorectal ERAS pathway. Table 1 presents the data in numerical format. The number of male and female patients was approximately equal. The mean BMI was 27.7 with an SD of 6.5. The total body weight (TBW), ideal body weight (IBW), and anesthesia time are also shown. The majority of patients were ASA PS classification 2 (46.4%) and 3 (52.0).
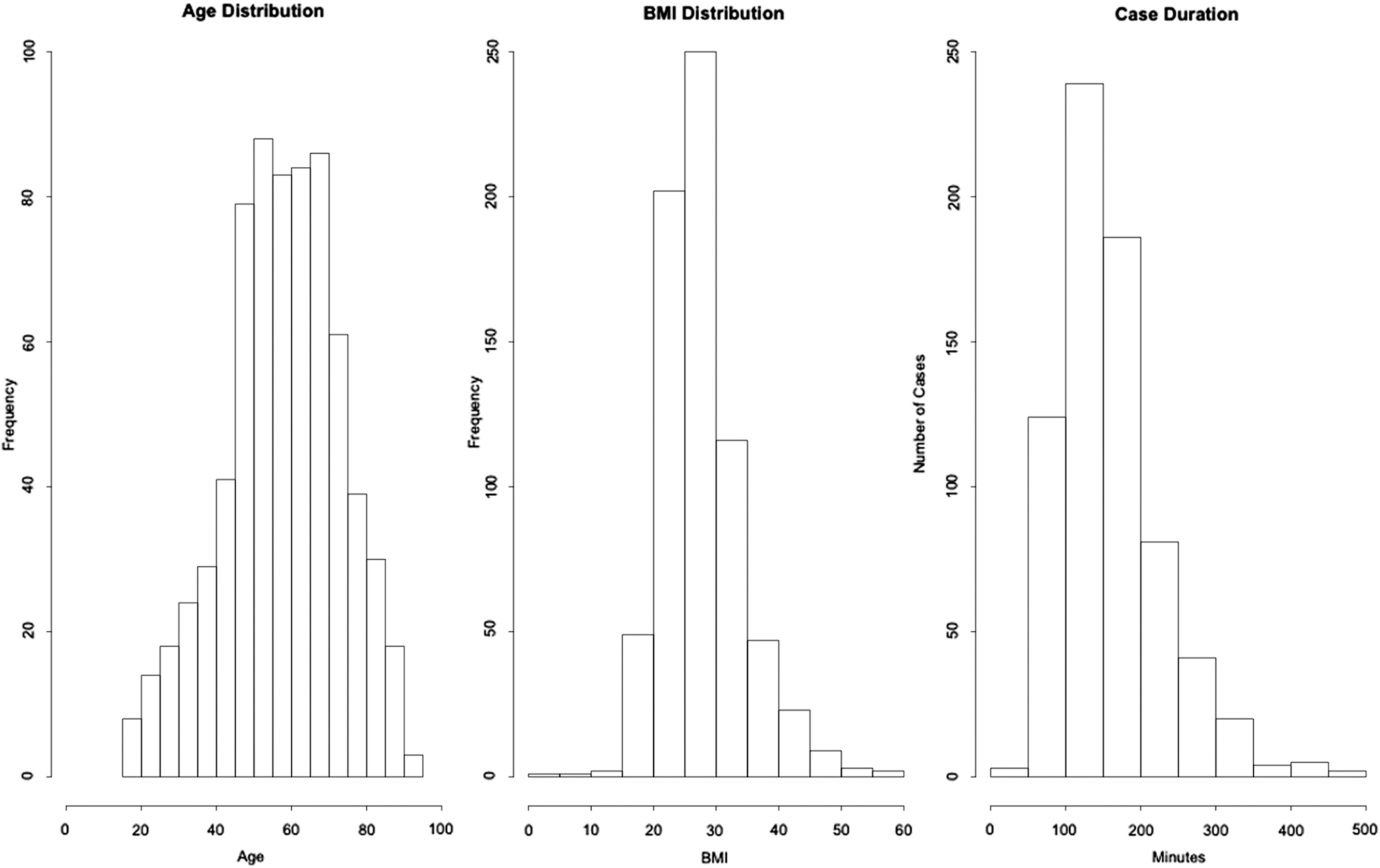
Age, BMI, and colorectal case duration for 705 elective colorectal surgeries. BMI, body mass index.
SD, standard deviation.
Table 2 shows the mean and SD of volume given for a variety of intravenous crystalloids and colloids, including lactated Ringer's, normal saline, Normosol/Plasmalyte, packed red blood cells (PRBCs), fresh frozen plasma (FFP), and platelets (Plts). The mean for total crystalloid administration was 2578 mL with an SD that was ∼50% of the mean value. For 700 out of the 705 cases studied, some amount of lactated Ringer's was infused. Normal saline was given for 625 out of 705 cases. The vast majority of patients received both normal saline and lactated Ringer's. For normal saline and lactated Ringer's, the SD was relatively large at 624 and 1488 mL, respectively. Normosol/Plasmalyte intravenous solutions were rarely used, representing only 0.4% of the cases reviewed. Less than 4% of the cases received a PRBC transfusion and less than 1% of the patients received Plts or FFP. Mean EBL and UO were relatively small (190 and 276 mL, respectively) compared to the amount of crystalloid administered, which was on the order of liters of fluid.
IQR, interquartile range; SD, standard deviation.
Table 3 shows total crystalloid administration for IBW and TBW. There was a large SD for fluid administration for both IBW and TBW. The mean cc/kg of total crystalloid given for IBW was 30.7 with an SD of 21.7. That was ∼67% variability in fluid therapy as a function of IBW. Similar results are seen for TBW with a mean cc/kg of total crystalloid of 34.3 and SD of 23.1 (70% variability on average). Patients received approximately a liter of crystalloid therapy per hour with an SD of nearly that same amount (8951 mL). The data are also presented graphically in Figure 2.
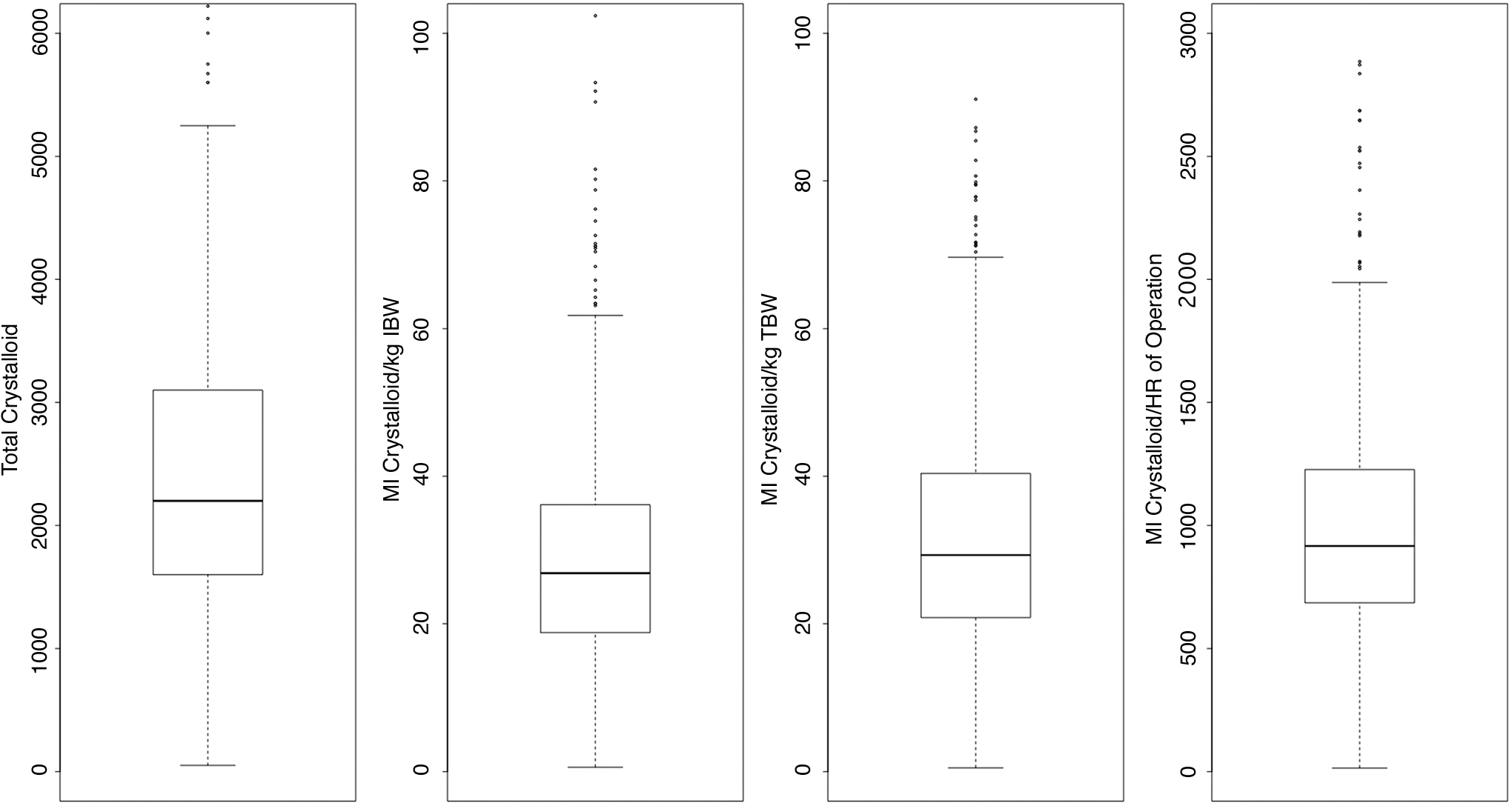
Total weight-based crystalloid administration. IBW, ideal body weight; TBW, total body weight.
SD, standard deviation.
Discussion
In our retrospective analysis of fluid administration at one academic institution, we found wide variability in fluid administration for colorectal surgery cases before implementation of an ERAS pathway. The SD for total crystalloid administration was approximately 50% of the entire mean fluid given for a case. Fluid therapy was approximately 1 L per hour with an SD that was nearly the same amount. Average fluid infused per hour was approximately the same as the SD (about 1 L of crystalloid). The variability was present when factoring for IBW and TBW. The analyzed data point to a potential area for improvement in perioperative care to reduce inconsistent fluid therapy among anesthesia providers, which can be achieved by education, feedback, consensus-building, and clinical protocols.
Based on analysis of the UO and EBL, it would seem that measurable fluid losses were not driving fluid therapy. Without specific information on individual cases, the likely impetus for fluid therapy is perceived insensible losses, replacement of fluid losses during nil per os (NPO) time before surgery, and/or bowel preparation. Both NPO and bowel preparation, a common practice in the past, are typically modified in an ERAS pathway to ameliorate the physiologic stress on patients. Patients are often encouraged to continue clear fluids per mouth up to 2 hours before surgery. Current recommendations advise against use of hyperosmolar bowel preparation in favor of iso-osmotic ones that do not cause significant preoperative dehydration requiring fluid replacement. 13
The selection of the type of crystalloid administered was likely arbitrary in our study. Almost every patient included in the study received both lactated Ringer's and normal saline. It is possible that lactated Ringer's was used because it is the default intravenous fluid hung during initial intravenous line placement in the preoperative area. The anesthesia provider may decide to switch to normal saline during the surgery. Neither fluid is physiologic. Lactated Ringer's is relatively hypotonic. Normal saline is hypertonic and large-volume infusions can lead to metabolic acidosis. 25 Although Normosol/Plasmalyte are more physiologic, only 3 patients received this fluid therapy type.
We believe the findings in our study support the use of a standardized clinical pathway, such as an ERAS pathway and GDFT to reduce the variability in fluid therapy for elective colorectal cases (colectomies, ileocolic resections, and low anterior resections). However, the efficacy of GDFT to reduce morbidity and mortality in the context of an ERAS pathway has been called into question in the literature. 26 The available research suggests that if an institution is already engaged in an ERAS pathway, the measureable positive effects of GDFT on its own may not be evident. Nonetheless, more judicious administration of intravenous fluids as well as decreased NPO and preoperative dehydration could naturally lead to less overall fluid given, less deviation in fluid therapy, and a fluid therapy plan that achieves euvolemia rather than hypovolemia or fluid overload. Fluid therapy administration practices have changed as ERAS pathways continue to develop. It may not be possible any longer to see large, statistically significant effects of more judicious fluid therapy as more providers adopt this approach. However, the potential benefits of rational fluid therapy with other ERAS pathways are numerous. 15
There are limitations to our retrospective study. Our study includes data from different surgeons, different anesthesia providers, different patient populations with comorbidities not captured in our analysis, and variation in the types of elective colorectal surgery performed that may have affected the results. However, finding ways to reduce variability in perioperative care, especially fluid management, is precisely what makes implementation of an ERAS pathway and GDFT potentially beneficial. The goal is not to treat every patient the same as each patient will present with their own unique issues and each surgery may progress differently. The objective is to develop a uniform approach to fluid management so that deviations from a “straightforward” case can be assessed in a uniform manner. With more homogeneity in fluid management in our group, trends can more easily be identified and improvements initiated with the greatest potential positive impact for our patients. The data we found in our study suggest that before a colorectal ERAS pathway and GDFT were used at our institution, we were inconsistent in our approach to fluid management.
Implementation of an ERAS pathway and GDFT is not a one-step process nor will it be the same at every institution. The unique characteristics of each institution, including patient population and surgeries performed, should be taken into account. Decisions need to be made regarding which advanced hemodynamic monitor to use (esophageal Doppler monitor, arterial contour waveform analysis, etc.), which variables to optimize (i.e., SVV, PPV), and which protocols to use (fluid versus fluid and vasopressors). The literature does not fully support one model over another at the present time. It is important to engage anesthesia providers in the process of crafting protocols to increase the likelihood of participation and investment in ongoing quality improvement.
Future direction from our study would be investigating how fluid therapy at our institution has changed after implementation of an ERAS pathway and GDFT initiatives and which hemodynamic monitoring modalities are most effective. While it is recommended that fluid therapy be guided by patient-specific criteria and not adherence to strict protocols, the large variability that is pervasive throughout the data we analyzed implies there was no uniform fluid therapy goal or assessment of fluid responsiveness occurring at our institution during the study period. A thorough perioperative fluid management plan emphasizing minimizing relative hypovolemia and fluid overload can lead to improved surgical outcomes. ERAS pathways and GDFT present an opportunity to achieve this in a systematic way.
Footnotes
Disclosure Statement
There are no conflicts of interest to report. The manuscript is not under consideration for publication elsewhere and it has never been partially published. There were no sources of financial support. ERAS