
Abstract
Abstract
Background:
Single-incision laparoscopic surgery (SILS) is a feasible and safe procedure for colorectal cancer. However, SILS has some technical limitations such as collision between instruments and inadequate countertraction. We present a hybrid single-incision laparoscopic surgery (hybrid SILS) technique for colon cancer that involves use of one additional 5 mm trocar.
Methods:
Hybrid SILS for colon cancer was attempted in 70 consecutive patients by a single surgeon between August 2014 and July 2016 at Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine. Using prospectively collected data, an observational study was performed on an intention-to-treat basis.
Results:
Hybrid SILS was technically completed in 66 patients, with a failure rate of 5.7% (4/70). One patient was converted to open surgery for para-aortic lymph node dissection. Another was converted to open surgery due to severe peritoneal adhesion. An additional trocar was inserted for adhesiolysis in the other two cases. Median lengths of proximal and distal margins were 12.8 cm (interquartile range [IQR], 10.0–18.6), and 8.2 cm (IQR, 5.5–18.3), respectively. Median total number of lymph nodes harvested was 24 (IQR, 18–33). Overall rate of postoperative morbidity was 12.9%, but there were no Clavien-Dindo grade III or IV complications. There was no postoperative mortality or reoperation. Median postoperative hospital stay was 6 days (IQR, 5–7).
Conclusions:
Hybrid SILS using one additional 5 mm trocar is a safe and effective minimally invasive surgical technique for colon cancer. Experienced laparoscopic surgeons can perform hybrid SILS without a learning curve based on the formulaic surgical techniques presented in this article.
Introduction
S
SILS has some technical limitations, namely collision between laparoscopic instruments and the camera scope due to crowding in a small single incision, typically through the umbilicus. Inadequate countertraction due to conflict between instruments can also make it difficult to dissect the tissue in an anatomically accurate manner.
Reduced port laparoscopic surgery (RPLS) is a surgical technique that uses fewer and or smaller trocars than those used in CMLS. RPLS includes SILS and SILS plus one additional port. RPLS using one additional port can retain the advantages of minimally invasive surgery while minimizing the limitations of SILS in colorectal surgery.6,7 SILS plus one additional port has been used to prevent conversion to CMLS or open surgery, but few of these studies have reported formulaic surgical techniques.8,9 Insertion of an additional 5 mm trocar at the beginning of surgery into the right lower quadrant for right or left colectomy and anterior resection is a new concept. If necessary, an additional 5 mm trocar site could be used for a drain.
In this study, we present our surgical technique, which we call hybrid single-incision laparoscopic surgery (hybrid SILS), which has the following criteria: (1) transumbilical single incision; (2) only one additional trocar; and (3) trocar no larger than 5 mm.
Materials and Methods
This study involved 91 consecutive colon cancer surgeries performed by a single surgeon between August 2014 and July 2016 at Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine, Seoul, Korea. Rectal cancer surgery was excluded from this study, but low anterior resections performed for rectosigmoid junction cancer to resect distally 5 cm or more beyond tumor were included in this study. The study was approved by the Ethics Committee at our institution (KBSMC 2016-01-007). All surgeries included in this study were performed by an experienced surgeon who had completed over 400 cases of laparoscopic colorectal cancer surgery. During the study period, open surgery was performed in 21 patients (23.1%); 5 because of combined surgery, 12 because of an emergency operation performed for perforation or obstruction, and 4 due to a tumor larger than 10 cm or direct invasion. Altogether, 70 patients (76.9%) underwent hybrid SILS for colon cancer during the study period. Using prospectively collected data, an observational study was performed on an intention-to-treat basis.
Surgical procedure
After general anesthesia, all patients were placed in the modified lithotomy position. Hybrid SILS was performed with a platform using a hand-made glove port. This platform was made using one nonpowdered surgical glove (6.5″ size), two 12 mm trocars, and a commercially available wound protector (Alexis wound protector/retractor, small; Applied Medical, Rancho Santa Margarita, CA) (Fig. 1). A right-hand glove was used for left colectomy or anterior resection, and a left-hand glove was used for right colectomy.
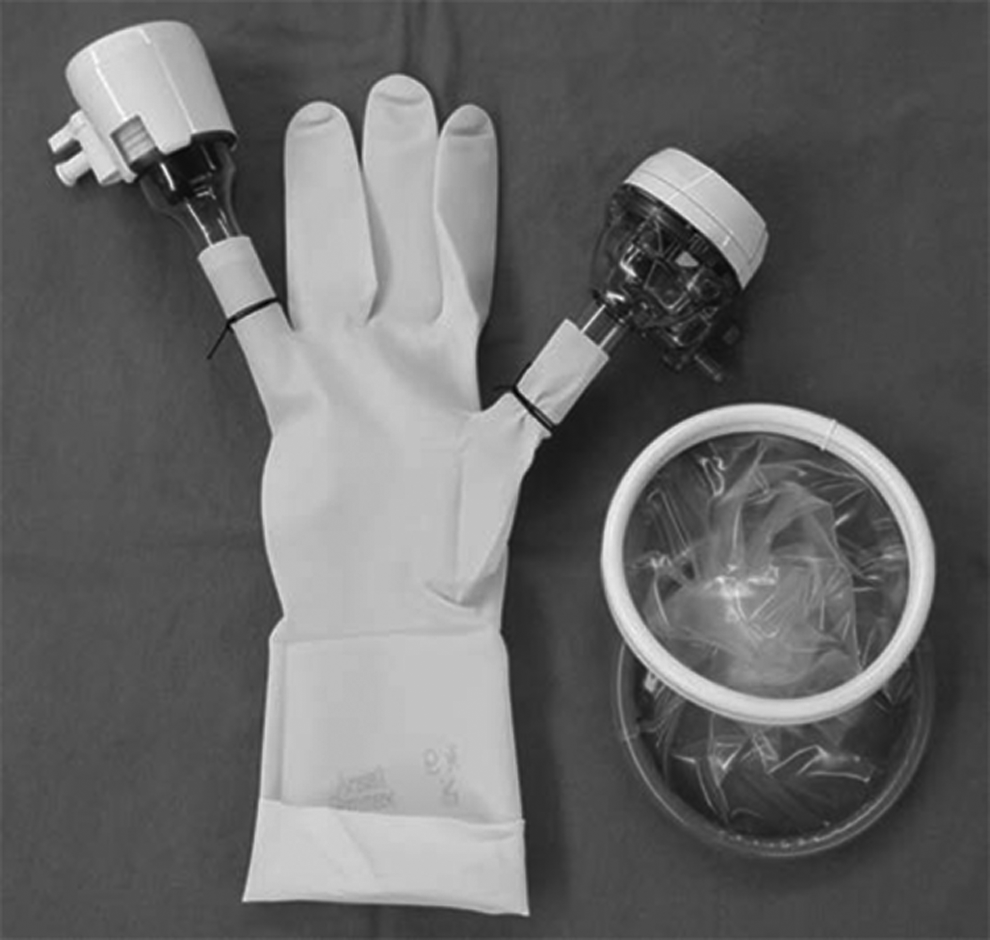
The hand-made glove port consists of one nonpowdered surgical glove (6.5″ size), two 12 mm trocars, and a commercially available wound protector.
First, a 3–4 cm longitudinal transumbilical incision was created, reflecting the patient's body shape and tumor size. After the wound protector was inserted into the incision, a hand-made glove port was connected to the wound protector, and they were rolled up together. In cases of left colectomy or anterior resection, the platform using a right-hand glove was aligned to the axis directed to the right anterior superior iliac spine. For right colectomy, the platform using the left-hand glove was aligned to the axis directed to the left anterior superior iliac spine (Fig. 2). These alignments were performed to minimize collisions between laparoscopic instruments and the camera scope. An additional 5 mm trocar was inserted into the right lower quadrant in all cases of right or left colectomy and anterior resection (Fig. 2). In all cases, a 10 mm flexible type scope and standard laparoscopic straight instruments were used.
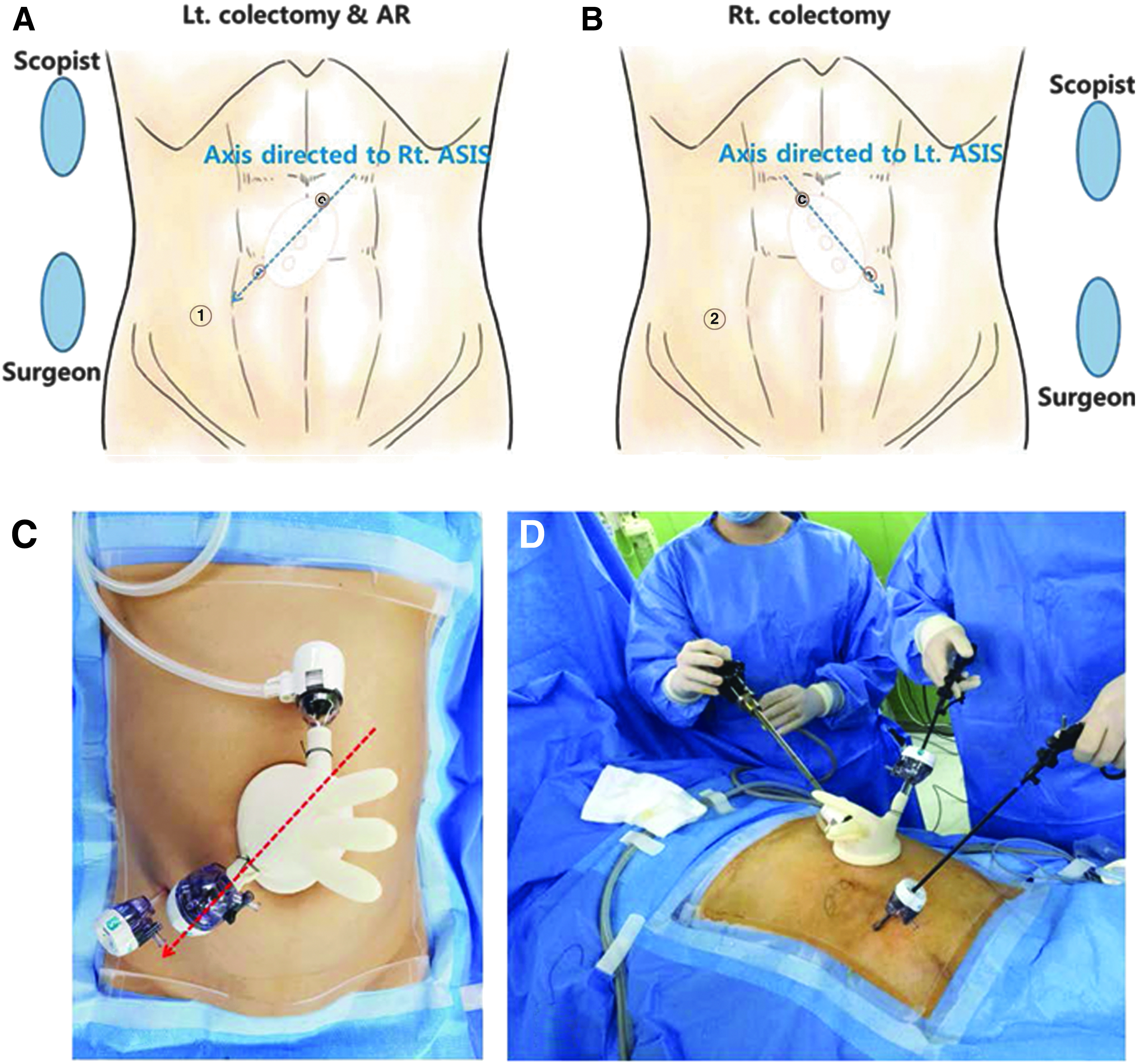
When setting up hybrid single-incision laparoscopic surgery (hybrid SILS), alignment of the glove port is important to reduce collisions. Left colectomy and anterior resection using a right-hand glove
Colectomy and anterior resection were performed according to the surgical strategy of complete mesocolic excision (CME) and D3 lymph node dissection for T1–T4 or resectable metastatic colon cancer (Fig. 3). In some cases, D2 resection was performed for T1 cancer confirmed after colonoscopic resection.

Ileocolic vessels at their origins
Right colectomy
Right hemicolectomy was started using an inferior approach, with peritoneal dissection between the mesoileum and the retroperitoneum with the patient in the Trendelenburg position with the right tilted upward. After continuous dissection from bottom to top through the anatomical plane along the Toldt's fascia, ileocolic vessels, right colic vessels, and the right branches of the middle colic vessels were ligated at their origins. The origins of the middle colic vessels were ligated in cases of extended right hemicolectomy. CME was completed, and the patient was then positioned in the reverse Trendelenburg position for takedown of the hepatic flexure and transverse colon from the parietal peritoneum. After right hemicolectomy, extracorporeal end-to-side anastomosis was performed using circular and linear staplers.
Left colectomy and anterior resection
The patient was placed in the Trendelenburg position with the left tilted upward. Using conventional laparoscopic techniques, the origin of the inferior mesenteric artery (IMA) was exposed, skeletonized, and then ligated. Medial to lateral dissection was continued from medial to lateral through the anatomical plane along the Toldt's fascia. The inferior mesenteric vein was also ligated at the origin, below the inferior border of the pancreas, in case splenic flexure mobilization had to be performed. In distal sigmoid or rectosigmoid junction cancer cases, distal resection was performed at least 5 cm beyond the tumor. Anastomosis was performed intracorporeally using a conventional double-stapling technique. In some cases, the root of the left colic artery was ligated after IMA lymph node dissection in the splenic flexure or proximal descending cancer, followed by anastomosis on a case-by-case basis.
Perioperative management
Patients scheduled to undergo left colectomy or anterior resection preoperatively received standard mechanical bowel preparation with 4 L polyethylene glycol (Colyte F; Taejoon Pharm, Inc., Seoul, Korea). Right colectomy was performed after minimal bowel preparation using 250 mL Magcorol solution (Taejoon Pharm, Inc., Seoul, Korea). A urinary catheter was inserted in the operation room following general anesthesia. All anesthetic procedures were performed in a routine manner. Intravenous patient-controlled analgesia was postoperatively used for pain relief according to patient preference. After full recovery from general anesthesia, all patients were allowed a clear fluid diet. On the first postoperative day, patients received a liquid diet, which was then advanced as tolerated. The urinary catheter was removed at 6 am on the first postoperative day, after which all patients were encouraged to ambulate. Patients were discharged from hospital to home after they were tolerable in regular diet and experienced normal bowel movement.
Result
Patient characteristics
In total, 70 patients with a mean age of 66.8 ± 12.1 years were analyzed. Clinical data, including gender, body mass index, American Society of Anesthesiologists (ASA) score, history of previous major abdominal surgery, and tumor location, are show in Table 1. Intention-to-treat analysis was performed. Categorical data are presented as percentage and quantitative data as mean ± standard deviation or median value with interquartile range (IQR).
Values are presented as n (%) and mean value ± standard deviation.
ASA, American Society of Anesthesiologists.
Perioperative outcomes
The most common type of surgery was anterior resection (32, 45.7%). Hybrid SILS failed for technical reasons in 4 patients (5.7%). One patient was converted to open surgery for para-aortic lymph node dissection after confirmation of para-aortic lymph node metastases by intraoperative frozen sectioning. Severe peritoneal adhesion resulted in conversion of hybrid SILS to open surgery in one case and necessitated the use of additional trocars in two cases. Intraoperative blood loss was less than 50 mL in 80.0% of cases and more than 100 mL in just 5.7% of cases. No transfusions were required during the surgeries. Mean operation time was 152.0 ± 37.0 minutes (Table 2).
Values are presented as n (%), mean value ± standard deviation, or median value (interquartile range).
Mean tumor size was 4.0 ± 2.5 cm. Median lengths of proximal and distal margins were 12.8 cm (IQR, 10.0–18.6) and 8.2 cm (IQR, 5.5–18.3), respectively. Total number of lymph nodes harvested was median 24 (IQR, 18–33) and mean 27.1 ± 13.9. Pathologic stage was evenly distributed (Table 3).
Values are presented as n (%), mean value ± standard deviation, or median value (interquartile range).
The 7th edition of the American Joint Committee on Cancer Manual.
Overall rate of postoperative morbidity was 12.9%. No Clavien–Dindo grade III or IV complications were observed. There was no surgical site infection, postoperative mortality, or reoperation within 30 days after surgery. There was no incisional hernia during the study period. During the follow-up period, 22 months after surgery, an incisional hernia occurred in a 75-year-old male patient who had suffered from chronic kidney disease. Median postoperative hospital stay was 6 days (IQR, 5–7) (Table 4).
Values are presented as n (%) and median value (interquartile range).
Discussion
SILS is frequently compared with CMLS and has been found to be feasible to perform, with several advantages compared with CMLS.1,3,4,8–11 Reduction in hospital stay and less blood loss are commonly reported advantages of SILS over CMLS.10,11 However, most reports have recommended performing larger, multicentered, randomized controlled trials (RCTs) to confirm the benefits of SILS and to clarify risks and disadvantages of SILS.3,4,10,11 SILS obviously has more technical limitations than CMLS such as collision between laparoscopic instruments and the camera scope due to crowding in a small single incision. In addition to these technical limitations, the safety and advantages of SILS might be overestimated, because SILS is generally performed by experienced laparoscopic surgeons. Furthermore, the possible advantages of SILS might be due to bias in patient selection criteria and reporting by SILS enthusiasts. 12 RCTs of single-incision laparoscopic colectomy (SILC) did not find SILC to be superior to CMLS.13,14 However, a RCT that enrolled only a selected group of patients with small tumors and good operative risk showed that SILC was associated with less postoperative pain and shorter hospital stay than CMLS. 15
We conceived of hybrid SILS to overcome the technical limitations of SILS. In the present case series, a platform with a glove and two 12 mm trocars was used. The feasibility of a glove port for abdominal surgery, mainly cholecystectomy, was first demonstrated in 2010. 16 A glove port can minimize conflicts between the camera scope and instruments compared with other commercially available SILS platforms. A 6.5″ surgical glove is sufficiently flexible to separate the trocars for full movement with the camera scope or laparoscopic instruments inserted. Furthermore, only two trocars are inserted into the SILS platform in hybrid SILS, minimizing crowding in the small single incision. These features allow a shift from RPLS using three ports to hybrid SILS. Based on our experience, hybrid SILS is technically very similar to RPLS using three ports. Experienced laparoscopic surgeons who can perform colon cancer surgery using only three ports can shift to hybrid SILS without a learning curve.
In our hospital, CME with D3 lymph node dissection is routinely performed in most curative colectomy and anterior resections. D2 resection is performed only for pathologically confirmed T1 cancer. Although there is limited evidence that CME with D3 lymph node dissection leads to longer disease-free survival than D2 or less dissection, CME is associated with a larger number of lymph nodes harvested, an important quality marker of oncologic outcome. 17 Hybrid SILS could provide a safe laparoscopic surgical field to complete CME with D3 lymph node dissection. In this study, median total number of lymph nodes harvested was 24 (IQR, 18–33); fewer than 12 lymph nodes were harvested in only two patients, both of whom had undergone D2 resection for T1 cancer. With regard to the surgical strategy of CME and D3 lymph node dissection for colon cancer, well designed prospective RCTs are needed to conclude whether this strategy affords better long-term oncologic outcomes than other strategies. Under these circumferences, hybrid SILS could maximize the possible benefits of SILS by minimizing technical limitations.
We excluded patients who underwent low anterior resection using the hybrid SILS technique for rectal cancer. Low anterior resections performed for rectosigmoid junction cancer to resect distally 5 cm or more beyond tumor were included in this study, since upper or midrectum could be vertically transected through an umbilical single incision without excessive efforts and complications. However, when using SILS for rectal cancer, it is technically difficult to vertically transect the distal rectum through the umbilical single incision, even when using an articulating linear stapler. In particular, a narrow pelvis and/or lower rectal cancer necessitate replacement of the 5 mm trocar in the right lower quadrant to a 12 mm trocar for insertion of a linear stapler. This is a violation of the criteria for hybrid SILS. The next challenge is how to vertically transect the distal rectum through an umbilical single incision without excessive efforts and complications. Advancements in laparoscopic staplers or changes in surgical techniques would make it feasible to perform distal rectal transection using SILS.2,18
Hybrid SILS is one of the RPLS with insertion of an additional 5 mm trocar during SILS. In previous reports of SILS plus one additional port, the additional port appeared to have been inserted during SILS to prevent conversion into CMLS or open surgery.8,9 However, insertion of an additional 5 mm trocar at the beginning of surgery into the right lower quadrant for right or left colectomy and anterior resection is a new concept. If necessary, an additional 5 mm trocar site could be used for a drain. Among the studies of SILS, a few have mentioned use of a postoperative drain in SILS.1,2,8,9,14,19 Drains are usually inserted through the umbilical single incision site in SILS, but in cases using an additional trocar, the drain was inserted in the additional trocar site. 9 In a Korean multicenter study of SILS, a drain was inserted in 65.4% of cases, and the most frequent site was the umbilical incision. 1 If the decision is made to leave a drain, the right lower quadrant, an additional 5 mm trocar site, might be a proper site for the drain in cases of right colectomy or anterior resection, which were the great part of colon cancer surgery. Insertion of a drain into the additional trocar site in RPLS (SILS plus one) indicates that an umbilical incision is not the correct route for a drain.8,9 Further studies would be needed to define the necessity and route of surgical site drains in SILS/RPLS.
Median postoperative hospital stay was 6 days (IQR, 5–7) in this study. Korean patients are usually discharged from hospital to home after they are tolerable in regular diet and experience normal bowel movement, since all people living legally in Korea are automatically enrolled in the national health insurance and total medical cost in the hospital is low. Therefore, total hospital stay in Korea would be longer than in other countries.
In conclusion, one additional 5 mm trocar makes it easy to perform colon cancer surgery safely and effectively. Furthermore, this trocar site can be reused as the site for a postoperative drain (Fig. 4). Using the formulaic surgical technique presented in this study, experienced laparoscopic surgeons can perform hybrid SILS for colon cancer without a learning curve.

Immediate postoperative wound and drain
Footnotes
Disclosure Statement
No competing financial interests exist.