
Abstract
Abstract
Background:
To validate and compare the stone scoring systems (stone size [S], tract length [T], obstruction [O], number of involved calices [N], and essence or stone density [E] [S.T.O.N.E.], Guy's Stone Score [GSS], Clinical Research Office of the Endourological Society [CROES], and Seoul National University Renal Stone Complexity [S-ReSC]) used to predict postoperative stone-free status and complications after percutaneous nephrolithotomy (PCNL).
Methods:
A total of 567 patients who underwent PCNL for renal stones between January 2012 and August 2015 were included in the recent retrospective study. Sixty-one patients who had not done preoperative CT were excluded from the study. GSS, S.T.O.N.E., S-ReSC, and CROES nephrolithometry scores were calculated for each patient, and their potential association with stone-free status, operative and fluoroscopy time, and length of stay (LOS) was evaluated. Postoperative complications were graded according to the modified Clavien classification, and the correlation of scoring systems with postoperative complications was also investigated.
Results:
The mean CROES, S.T.O.N.E., GSS, and S-ReSC scores were 203.7 ± 59.8, 7.52 ± 1.8, 2.08 ± 0.9, and 3.35 ± 2.2, respectively. The overall stone-free rate was 77.9%. All scoring systems were significantly correlated with stone-free status and operation time. While GSS, S.T.O.N.E., and CROES systems were significantly correlated with complication rates (CR), S-ReSC score failed to predict CR. All scoring systems except S.T.O.N.E. were significantly correlated with LOS. CROES and S-ReSC scores were predictive of estimated blood loss (EBL), while GSS and S.T.O.N.E. failed to predict EBL.
Conclusions:
Recent study demonstrated that S.T.O.N.E., GSS, CROES, and S-ReSC scoring systems could effectively predict postoperative stone-free status. Although S-ReSC scoring system failed to predict CR, the rest three scoring systems were significantly correlated with postoperative CR.
Introduction
P
GSS categorizes PCNL complexity into four grades (grade I, II, III, IV) according to the patient's and imaging characteristics. 3 S.T.O.N.E. score is calculated using five variables, including stone size, tract length (skin-to-stone distance), degree of obstruction, number of calices involved, and stone essence (density). 4 CROES nephrolithometry nomogram was developed by Smith et al. on behalf of the CROES PCNL Study Group. 6 In this nomogram all parameters, including preoperative radiological findings, as well as patient factors, correspond to a specific score and the total score is calculated. S-ReSC scoring system was developed by Jeong et al. to predict the outcomes of PCNL that had been performed using only one access. 5 There is still a lack of agreement about the best scoring system. 7 In the recent study we aimed to compare the efficacy of the four most used scoring systems. To the best of our knowledge, the recent study is the first one in the literature comparing all the four stone scoring systems.
Materials and Methods
After obtaining internal institutional review board approval, patients undergoing PCNL between January 2012 and August 2015 were retrospectively reviewed. Patients with an available preoperative computed tomography (CT) were included in the study. Sixty-one patients who had more than one access were excluded from the study because the S-ReSC scoring system was developed for evaluation of outcomes of PCNL performed using only one access. PCNL was performed in prone position under general anesthesia. Access was obtained under fluoroscopy using an 18 gauge needle, and tract was dilated with Amplatz dilators. Stone fragmentation was accomplished using a pneumatic lithotripter (Vibrolith®; Elmed, Ankara, Turkey). At the end of the procedure, 14F nephrostomy tube was inserted, and antegrade pyelography was performed. Patient demographics (age, gender, body mass index [BMI]) and perioperative data were recorded by surgeon immediately postoperatively. Perioperative data included operation side, stone burden, location of percutaneous tracts, operative and fluoroscopy times, length of stay (LOS), estimated blood loss (EBL), and intraoperative stone-free status. Also postoperative complications were noted according to the Clavien grades.
Stone-free status was assessed on 1-month postoperative visit using kidney ureter bladder (KUB) radiograph. In our practice, KUB radiograph is used for routine evaluation of post-PCNL stone status, because of the cost. CT is reserved for only symptomatic patients, radiolucent stones, and/or suspicion of residual fragments seen on KUB radiography. Residual stone size of <4 mm on KUB or CT was described as clinically insignificant residual fragments, and these patients were considered as stone free.
The scores of each scoring system (GSS, S.T.O.N.E., S-ReSC, and CROES) were calculated using preoperative CT as described by Thomas et al., 3 Okhunov et al., 4 Jeong et al., 5 and Smith et al. 6 Association between these scores and complications, stone-free status, stone burden, operative time, EBL, and LOS was assessed. In CROES scoring system, we categorized patients into four grades (grade 1: 0–100, grade 2: 101–150, grade 3: 151–200, and grade 4: 201–350).
Statistical analysis
Categorical data were presented as numbers and percentages. Data for continuous variables are presented as mean and standard deviation. Pearson correlation coefficient was used to evaluate whether GSS, S.T.O.N.E., S-ReSC, and CROES nephrolithometry scores are associated with complications, stone-free status, stone burden, operative time, EBL, and LOS. Receiver operating characteristic (ROC) analysis was used to assess the predictive ability of each scoring system on the stone-free rates (SFR) and complications. Statistical analysis was performed using Statistical Package of Social Sciences version 21 (IBM SPSS Statistics; IBM Corp., Armonk, NY).
Results
A total of 506 cases were included in the study. The demographic and perioperative characteristics of the patients are summarized in Table 1. Thirty-four patients who had renal anomalies, including horseshoe kidney (5), bifid renal pelvis (7), renal rotational anomalies (14), and ureteropelvic junction obstruction (8), were in the study. Mean stone burden was 502.01 ± 517.5 (55–2869) mm2. All PCNLs were performed using one access. Mean operation time and fluoroscopy time were 102.06 ± 39.4 (25–300) minutes and 78.67 ± 49.7 (9–410) seconds, respectively. Residual fragments were detected in 112 (22.1%) patients.
BMI, body mass index; CROES, Clinical Research Office of the Endourological Society; GSS, Guy's Stone Score; SD, standard deviation; S-ReSC, Seoul National University Renal Stone Complexity; S.T.O.N.E., stone size (S), tract length (T), obstruction (O), number of involved calices (N), and essence or stone density (E).
The mean CROES, S.T.O.N.E., GSS, and S-ReSC scores were 203.7 ± 59.8, 7.52 ± 1.8, 2.08 ± 0.9, and 3.35 ± 2.2, respectively. The overall SFR was 77.9%.
Correlations of scoring systems with evaluated parameters are shown in Table 2. All scoring systems were significantly correlated with stone-free status and operation time. While GSS, S.T.O.N.E., and CROES were significantly correlated with complication rates (CR), S-ReSC score failed to predict CR. All scoring systems except S.T.O.N.E. were significantly correlated with LOS. CROES and S-ReSC score were predictive of EBL, while GSS and S.T.O.N.E. failed to predict EBL. The complications graded according to modified Clavien classification system are shown in Table 3 in detail. The overall CR were 32.5%.
Bold text indicates values are statistically significant.
Correlation is significant at the 0.05 level (2-tailed).
Correlation is significant at the 0.01 level (2-tailed).
EBL, estimated blood loss; LOS, length of stay.
UTI, urinary tract infection.
ROC analysis of four scoring systems to predict stone-free status is shown in Figure 1. The cutoff points calculated with Youden index for stone-free status for GSS, S.T.O.N.E., S-ReSC, and CROES were 2.5 (sensitivity 78.4%, specificity 51.8%), 7.5 (sensitivity 66.5%, specificity 58%), 3.5 (sensitivity 69.8%, specificity 69%), and 199.5 (sensitivity 69.8%, specificity 69%), respectively.
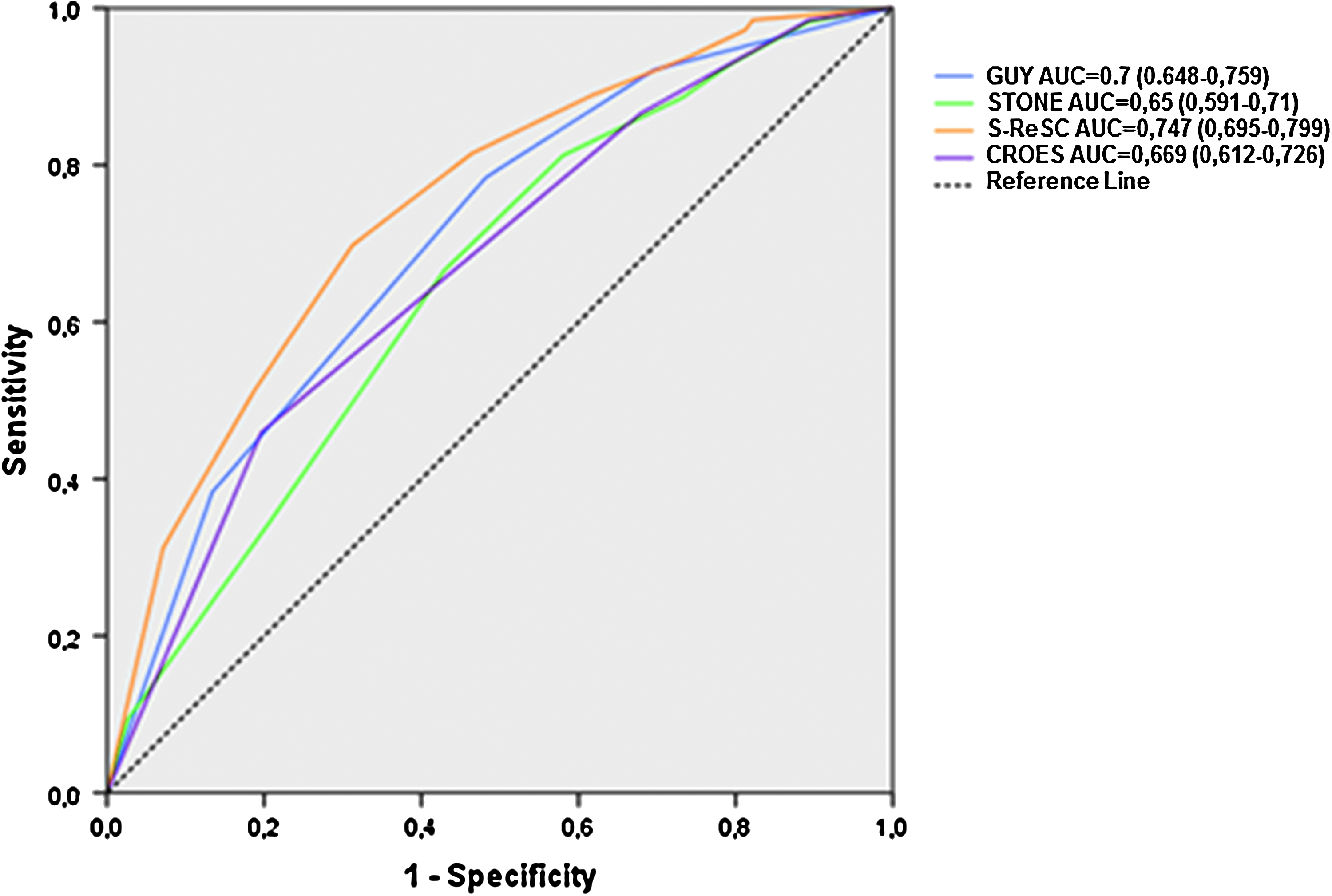
ROC curve for scoring systems in predicting stone-free status. AUC, area under the curve; CROES, Clinical Research Office of the Endourological Society; GUY, Guy's scoring system; ROC, receiver operating characteristic; S-ReSC, Seoul National University Renal Stone Complexity; STONE, stone size (S), tract length (T), obstruction (O), number of involved calices (N), and essence or stone density (E).
The ROC analysis of four scoring systems for predicting complications is shown in Figure 2. The cutoff points calculated using Youden index for predicting complications for GSS, S.T.O.N.E., and CROES were 2.5 (sensitivity 75.7%, specificity 37.5%), 9.5 (sensitivity 89%, specificity 23.7%), and 174.5 (sensitivity 86.2%, specificity 26.3%), respectively. A cutoff value was not calculated for the S-ReSC scoring system, since the S-ReSC could not predict the postoperative complications significantly.
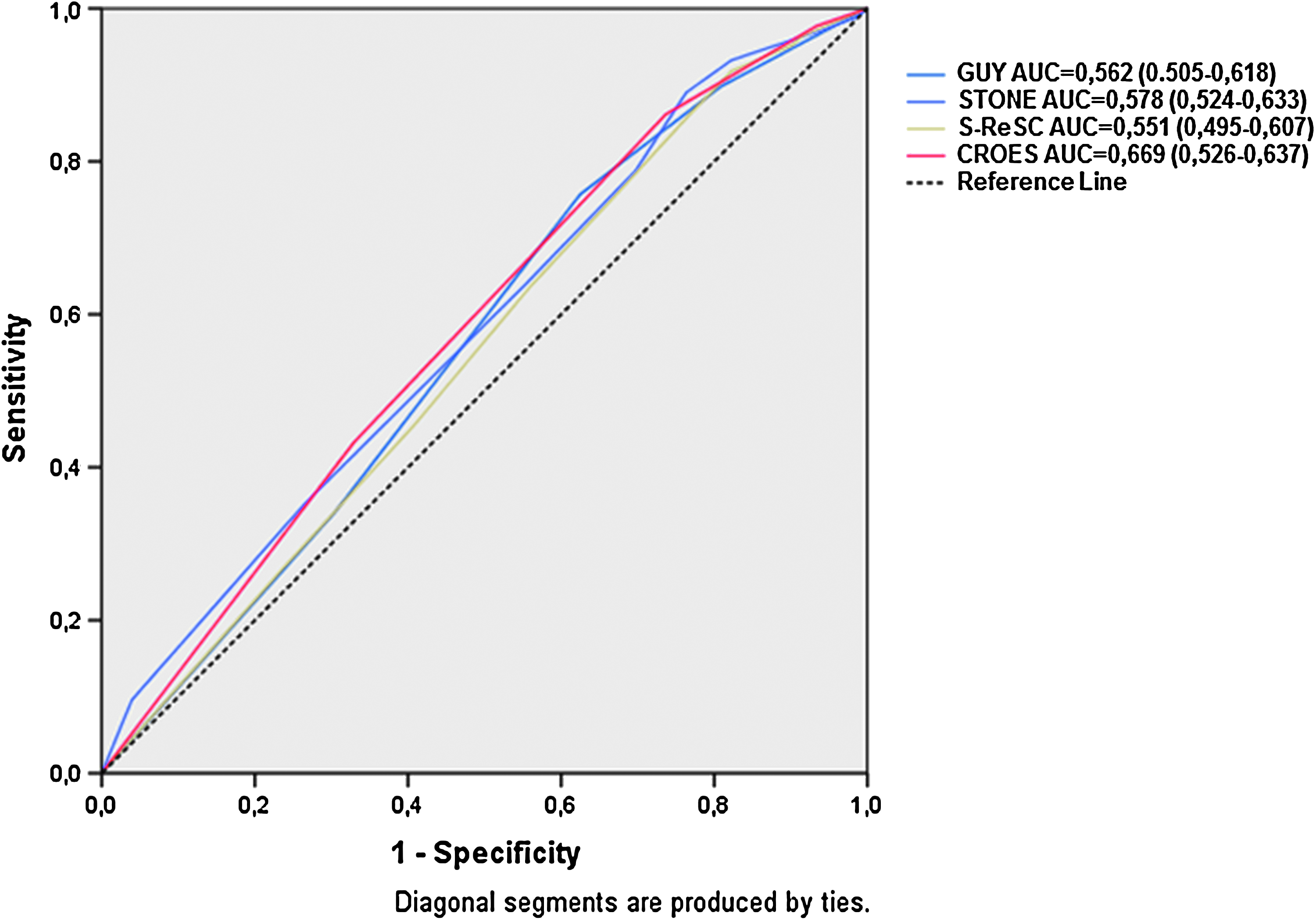
ROC curve for scoring systems in predicting complications.
Discussion
Preoperative imaging methods have critical importance to decide for the accurate diagnosis and optimum surgical management in patients with renal stones. 8 Multiplanar imaging has been the preferred one to detect the stone complexity, including stone size, location, pelvicaliceal anatomy, and association with adjacent organs.9,10 Postoperative stone-free status can be predicted with preoperative imaging methods.11–13 In the recent years, several scoring systems have been developed to standardize the terminology regarding stone complexity and for preoperative counseling of the patients.3–6
There are a total of 11 variables in four scoring systems, but only 2 of these variables are in common. The other nine variables (tract length, stone size, staghorn status, renal pelvic obstruction, stone density, case volume per year, number of stones, treatment history, renal anatomy, and spina bifida or spinal injury) are included separately in each scoring system. But only GSS includes abnormal renal anatomy into scoring systems. S.T.O.N.E. nephrolithometry, S-ReSC scoring system, and the CROES nomogram do not consider renal anomalies. However, results of large-scale studies demonstrated that abnormal renal anatomy is not associated with inferior surgical outcomes.14,15 We concluded renal anatomy does not affect directly PCNL results.
Ideal scoring system should be repeatable, easily used in daily practice, include the findings of imaging methods, and predict postoperative SFR and CR. 3 There is no universally accepted scoring system yet. We think that it is essential to compare the existing scoring systems and find out deficient parts to improve the ideal scoring system. In the present study, we investigated the potential role of GSS, S.T.O.N.E., S-ReSC, and CROES scoring systems to predict postoperative SFR and CR.
Previous studies revealed significant correlation between SFR, CR, and GSS.3,15–22 Kumsar et al. showed significant association among Clavien score, operation time, and GSS. 23 However the authors revealed no correlation between SFR and GSS. In a previous study, the authors advocated that although GSS is highly effective in predicting stone-free status, it is inefficient to predict CR. 24
Labadie et al. showed that GSS is significantly associated with hospitalization time and blood loss. 18 In another study, Vicentini et al. evaluated 155 PCNL cases and their findings revealed that GSS is significantly associated with blood transfusion rates and operation time. 17 In the current study, we found positive correlation between GSS and SFR, CR, operation time, hospitalization time, and stone burden, respectively.
In a previous study, the authors revealed a significant relationship between S.T.O.N.E. nephrolithometry score and SFR and bleeding. 18 In this study, an area under curve value of 0.67 was measured for S.T.O.N.E. nephrolithometry score, but a possible correlation between the scoring system and operation time was not examined. Noureldin et al. compared GSS and S.T.O.N.E. nephrolithometry scoring systems. 19 The authors mentioned that both scoring systems are effective in predicting SFR, blood loss, operation time, and hospitalization time. In a different study, the authors aimed to validate S.T.O.N.E. scoring system. 25 In this study, although S.T.O.N.E. score was found to be effective in predicting SFR, it wasn't significantly associated with CR. Farhan et al. found significant association between S.T.O.N.E. score and SFR and operation time, respectively. 26 However no significant association was detected between S.T.O.N.E. score and CR. Similarly, Akhavein et al. advocated that although S.T.O.N.E. scoring system was highly effective to predict postoperative SFR, it was not sufficient to predict CR. 27 In contrast Kumsar et al. found significant association between S.T.O.N.E. score and Clavien complication scores besides SFR. 23 In the recent study, a positive correlation was found between S.T.O.N.E. score and SFR, CR, operation time, stone burden, age, and BMI.
Labadie et al. revealed a significant relationship between CROES nomogram and postoperative SFR after PCNL. 18 Similarly previous validation studies showed that CROES nomogram is an effective and reliable scoring system to predict SFR.18,28
In a recent study, Bozkurt et al. investigated the results of 437 patients who underwent PCNL and compared GSS and CROES scoring systems. 29 In this study, both scoring systems were significantly associated with SFR, blood loss, operation time, and CR. In a previous study, the authors revealed that S.T.O.N.E. scoring system had a predictive role to show postoperative SFRs in patients with staghorn stones, while GSS and CROES systems were not effective. In the present study, we found positive correlation between CROES score and SFR, CR, operation time, hospitalization time, bleeding rate, and stone burden.
S-ReSC is a scoring system which was developed to predict postoperative SFR following PCNL. S-ReSC scoring system mainly uses the complex localization of the stone in the renal collecting system as the most important factor to predict SFR. However this system is not solely dependent on the distribution of the stone in the collecting system since this is closely related with the size and number of the stones. In the original study, cutoff value for S-ReSC score to predict stone-free status was calculated as 0.86. 5 In a different study, Choo et al. investigated the outcomes of 327 PCNL operations which were performed in 2 clinics by 4 different surgeons and their findings revealed a significant correlation between S-ReSC scoring system and SFR. 30 In this study, the cutoff value for S-ReSC score to predict SFR was measured as 0.773.
Although previous studies showed that S-ReSC scoring system was effective in predicting SFR after PCNL, to the best of our knowledge none of the studies investigated the potential role of S-ReSC system to predict postoperative complications.5,30 In the current study, we found positive correlation between S-ReSC score and SFR, operation time, hospitalization time, bleeding rate, and stone burden, respectively. However there was no significant association between the S-ReSC scoring system and postoperative CR.
The main limitations of the present study are its retrospective design which could possibly cause some bias, and all of the patients were not evaluated postoperatively with CT as a standard imaging method, and a residual stone size of <4 mm was accepted as stone free. Patients were evaluated with plain KUB radiography for financial constraints. And postoperative X-rays were analyzed by the same radiologist. However, to the best of our knowledge, the recent study is the first one in the literature comparing all the four stone scoring systems.
Conclusions
Our findings revealed that GSS, S.T.O.N.E., S-ReSC, and CROES scoring systems can be effectively and reliably used to predict SFR after PCNL. We think that scoring systems can be potentially used to standardize the postoperative outcomes of different studies and these systems can guide the clinician to predict postoperative PCNL outcomes.
None of the scoring systems is superior to other in predicting postoperative SFR. However, GSS can be more easily used in clinical practice. All scoring systems except S-ReSC were effective to predict postoperative complications.
Footnotes
Disclosure Statement
No competing financial interests exist.