
Abstract
Abstract
Background:
Anastomotic leakage is a determining factor of morbidity and mortality after an esophagectomy. An adequate blood supply of the gastric conduit is vital to prevent this complication. We aimed to determine the feasibility and usefulness of indocyanine green (ICG) fluorescence imaging to evaluate the gastric conduit perfusion during an esophagectomy.
Methods:
Patients with distal esophageal cancer or esophagogastric junction cancer scheduled for esophagectomy were enrolled in this study. After pulling up the gastric conduit into the chest and before performing the anastomosis, 5 mg of ICG was injected as a bolus. Visual assessment of the blood supply of the gastric conduit was compared with the ICG fluorescence imaging pattern of perfusion.
Results:
Five patients were included in this study. Hybrid Ivor Lewis esophagectomy (laparoscopic abdomen and right thoracotomy) was performed in all cases. In all patients, visual assessment of the perfusion of the stomach determined that the conduit was well perfused. In two patients (40%), ICG fluorescence showed an inadequate blood supply of the conduit's tip. Resection of the devitalized portion of the conduit was performed in these two patients. No anastomotic leaks were recorded, and all patients had an uneventful postoperative course.
Conclusions:
Visual assessment of the gastric conduit may underestimate perfusion and inadequate blood supply. ICG fluorescence imaging is a promising tool to determine the gastric conduit perfusion during an esophagectomy. Prospective studies with larger series are warranted to confirm the usefulness of ICG fluorescence imaging during an esophagectomy.
Introduction
A
After esophagectomy, a gastric conduit is most frequently used for reconstruction. Poor blood supply at the tip of the gastric conduit is one of the most important factors contributing to anastomotic leakage, along with tension. Traditionally, perfusion and viability of the conduit have been determined subjectively by surgeons, based on color of the conduit, bleeding, and a palpable right gastroepiploic artery. Thus, an objective method for effective evaluation of blood supply is warranted. As indocyanine green (ICG)-enhanced fluorescence imaging provides a real-time video image of the distributive pattern of vascularity, it is simple to use, it is not linked to complications, and it seems to be an ideal tool to visualize the perfusion of the gastric conduit during an esophagectomy. 8
We aimed to determine the feasibility and usefulness of ICG fluorescence imaging to evaluate the gastric conduit perfusion during an esophagectomy.
Materials and Methods
A consecutive series of patients with distal and esophagogastric junction esophageal cancer scheduled for esophagectomy were included in this study. Preoperative work-up included barium swallow, endoscopy, endoscopic ultrasound, and positron emission tomography in all patients. Patients underwent induction chemotherapy and radiation followed by surgery or upfront surgery as indicated by the stage of their tumor.
All patients included in the study were consented, and the study was approved by the Institutional Review Board of the University of North Carolina.
Hybrid Ivor Lewis esophagectomy technique and ICG protocol
The aim of the initial laparoscopic portion was to dissect the abdominal esophagus, esophageal hiatus, and create the gastric conduit. The patient was placed in a supine, steep reverse Trendelenburg position and intubated with a double lumen endotracheal tube. Five abdominal ports were typically utilized. A 10 mm port was placed about 20 cm distal to the xiphoid process. Four subsequent 5–12 mm ports were placed under direct visualization in the right and left upper quadrant. The first step was the mobilization of the greater curvature by the division of the gastrocolic omentum while preserving the gastroepiploic arcade, and by the division of the short gastric vessels. The gastrohepatic ligament was then divided preserving the right gastric artery, and the hiatus and distal esophagus were dissected. The left gastric artery and the coronary vein were then isolated and divided at their origin with a vascular stapler. A Penrose was placed around the esophagus and advanced into the mediastinum.
Once the abdominal part of the operation was completed, the patient was placed in a left lateral decubitus position. A muscle preserving right thoracotomy was performed in the fifth intercostal space. The right lung was deflated and retracted anteriorly. The azygos vein was divided. The esophagus was dissected from the vertebral body and the pericardium. The stomach was then pulled into the chest and divided with linear staplers to build the gastric conduit.
Immediately after resecting the specimen, and before reconstruction, 5 mg of ICG (ICG-Pulsion®; Pulsion Medical Systems, Munich, Germany) was injected intravenously as a bolus. Ten milliliters of normal saline was then injected. A video camera was then connected to an ICG laparoscope with a high-end full HD camera system (IMAGE1 STORZ professional image enhancement system), and equipped with a special filter for optimal reproduction during ICG-enhanced fluorescence and standard white light imaging. As ambient illumination interferes with the fluorescence detection sensitivity of the video camera, all the operating room lights were turned off for the ICG detection.
Visual assessment of the perfusion of the gastric conduit was assessed with the ICG fluorescence-imaging pattern of perfusion. Subsequently, an intrathoracic esophagogastric stapled side-to-side anastomosis was performed at the level of the azygos vein.
Postoperative follow-up
All patients were prospectively followed by the two surgeons involved in the study (F.S. and M.G.P.).
The postoperative care protocol included removal of the nasogastric tube on postoperative day (POD) 2, start with liquids on POD 4 and soft diet on POD 5, and subsequent discharge depending on pain control and oral intake.
Results
Five consecutive patients were included in this study. A hybrid Ivor Lewis esophagectomy was performed in all cases.
In all patients visual assessment determined that the gastric conduit was well perfused. However, in two patients (40%), ICG fluorescence showed an inadequate blood supply of the conduit's tip (Fig. 1). Resection of the devitalized portion of the conduit was performed in these two patients.
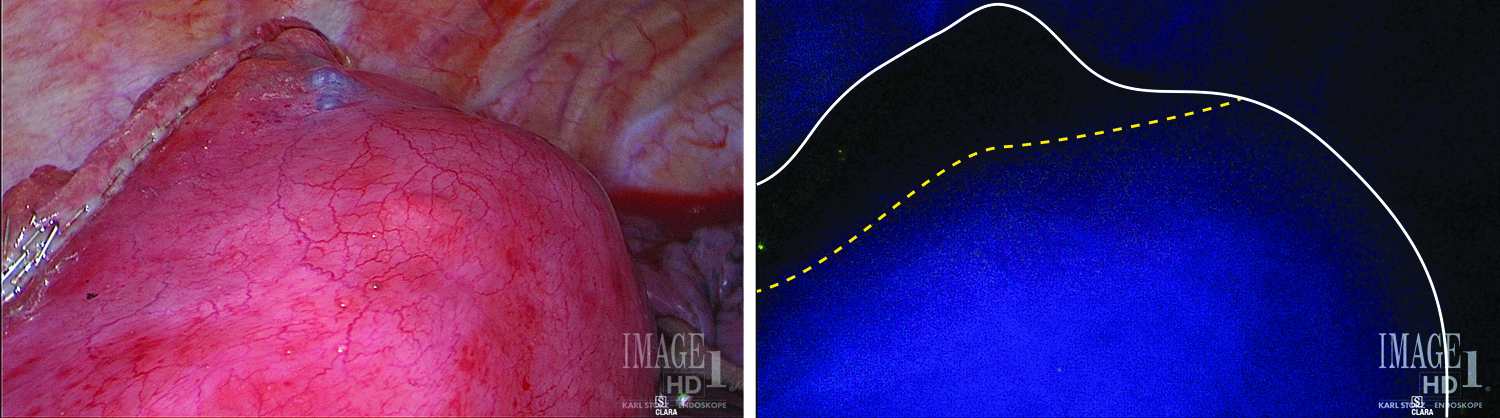
Assessment of gastric conduit's perfusion with standard white light imaging and with ICG fluorescence imaging. Conduit's tip presumably well perfused with standard white light but inadequately perfused with ICG imaging assessment. ICG, indocyanine green.
The intraoperative and postoperative course of all patients was uneventful, and no anastomotic leaks were recorded. The mean length of hospital stay was 8.8 days.7–11
The characteristics of the patients enrolled in the study are shown in Table 1.
Adeno, adenocarcinoma; F, female; HIL, hybrid Ivor Lewis; M, male; pN, pathological nodal metastasis; pT, pathological tumor depth of invasion.
Discussion
We performed a pilot study to determine the feasibility and usefulness of ICG fluorescence imaging to evaluate the gastric conduit perfusion during an esophagectomy. We found this imaging technology to be a promising tool to determine the blood supply of the gastric conduit.
Although several factors have an influence on the development of anastomotic leakage, blood perfusion is thought to be one of the most important causes. Currently, there is no universally accepted method to assess the perfusion of gastrointestinal anastomoses. Surgeons usually check the viability of the stomach by gross inspection of the intestinal color, pulsations of the vessels, and bleeding from the cut edge. A previous study, however, showed that surgeons' clinical risk assessment had a low predictive value for anastomotic leakage in gastrointestinal surgery. 9 The authors evaluated the accuracy of the surgeons' estimation of risk for anastomotic leakage of colorectal anastomoses above or under 15 cm from the anal verge. For an accurate risk assessment of leakage, sensitivity was 38% for high anastomoses and 62% for low anastomosis, and specificity was 46% and 52%, respectively. 9
ICG fluorescence imaging is a relatively new technique to assess the perfusion of gastric conduit intraoperatively.10,11 The ICG dye can be injected intravenously with practically no adverse effects. 12 The technique is based on the fluorescence effect of ICG when exposed to light at near infrared wavelength. Fluorescence is detected using specific scopes and cameras, and then transmitted to a video screen, thus enabling the observer to visualize areas of anatomical interest where the dye has accumulated. Specifically, the fact that the right gastroepiploic artery supplies most of the constructed gastric conduit during an esophagectomy makes it of paramount importance that the entire stomach is well perfused. Without successful strategies for increasing the blood supply of the conduit, assessment of its perfusion may be helpful in construction of the conduit and choice of anastomotic site.
Shimada et al. 13 evaluated the usefulness of blood supply visualization by ICG fluorescence for reconstruction during esophagectomy. The authors reported that this technique could detect organ blood flow before reconstruction and assist in evaluating the appropriate anastomotic sites. However, the incidence of anastomotic leakage was not reduced. 13 This finding suggests that microvessels detected by ICG fluorescence may not always provide enough blood for a viable anastomosis. On the contrary, Campbell et al. 14 reported that after the introduction of intraoperative vascular evaluation of the gastric conduit with ICG fluorescence imaging, the rate of anastomotic leakage decreased from 20% to 0%. Similarly, Koyanagi et al. 15 showed that intraoperative evaluation of blood flow speed by ICG fluorescence in the gastric conduit wall was a useful tool to predict the risk of anastomotic leakage.
It is worth mentioning that timing is very important. Once the ICG is injected on the patient, there are few seconds to identify the vascularization pattern with the highest possible resolution. Thus, it is of paramount importance to have the conduit in the correct position and the camera ready to be switched to the ICG-imaging system. Even though rare, allergic reactions to ICG have been documented and may represent a limitation for this technique.
In our small series, ICG was easily detected intraoperatively and the pattern of perfusion of the gastric conduit was identified in all patients. None of our patients experienced allergic reactions or any other adverse events related to the dye. While visual assessment determined that the conduit's tip was well perfused in all patients, in two patients (40%), ICG fluorescence showed an inadequate blood supply of the conduit's tip. This was an interesting finding, considering that it drove us to resect the devitalized portion of the conduit in those two patients. It is impossible to know what could have happened if those “ICG devitalized” tips were used for the esophagogastric anastomosis. Nevertheless, it is promising that no anastomotic leaks were recorded assessing the perfusion with ICG fluorescence.
Unfortunately, the assessment of fluorescence intensity remains somehow subjective with this technology. Protyniak et al. 16 attempted to quantify the light intensity by intraoperative pixel brightness analysis. However, they failed to determine a cutoff value, which is needed to minimize the interobservatory differences. Future imaging and software enhancements are warranted to achieve an objective method of fluorescence quantification.
Conclusion
Visual assessment of the gastric conduit may underestimate inadequate blood supply. ICG fluorescence imaging is a promising tool to determine the gastric conduit perfusion during an esophagectomy. Prospective studies with a larger number of patients are warranted to confirm the usefulness of ICG fluorescence imaging during an esophagectomy.
Footnotes
Disclosure Statement
No competing financial interests exist.