
Abstract
Abstract
Background:
A debate is still surrounding the use of laparoscopic surgery for advanced gastric cancer (AGC) related to doubts about the requirements to satisfy oncologic criteria. The aim of this study is to analyze the oncological results, the intraoperative complications, and the short- and medium-term morbidity and mortality in patients with AGC who underwent subtotal laparoscopic gastrectomy (SLG) or total laparoscopic gastrectomy (TLG) with extended lymphadenectomy.
Materials and Methods:
We reviewed medical records of patients who underwent radical gastrectomy for AGC started laparoscopically with the intent of curative surgery, between July 2007 and October 2015. We recruited 74 patients and studied demographics, American Society of Anesthesiologists (ASA) score, pTNM stage, histologic pattern of the tumor, duration of surgery, conversion rate, estimated blood loss, number of resected lymph nodes, type of gastrointestinal reconstruction, postoperative complication, mortality rate, length of stay, time to canalization and resumption of food intake, and overall and disease-free survival rate.
Results:
We performed 74 interventions, with a conversion rate of 14.9% (11/74). Sixty-three were performed totally as laparoscopic: 43 (68.25%) SLGs and 20 (31.75%) TLGs, all with an extended lymphadenectomy (D2 or more). Operative time was 150 ± 34 minutes (range 75–225 minutes), the mean number of resected lymph nodes 21.4 ± 6.2, global morbidity rate 25.39%, rate of reoperation 9.52%, and perioperative mortality at 30 days 0%. We performed an average follow-up of 48.7 months (range 18–60), and we observed 5-year overall and disease-free survival, respectively, of 48.6% and 42.7%.
Conclusions:
LG with extended lymphadenectomy for AGC is a feasible procedure with good results in terms of postoperative course, complications, and mortality. Thanks to the use of extremely precise and safe technologies the extended lymphadenectomy can be performed laparoscopically. The laparoscopic approach, when performed by experienced surgeons, ensures a correct oncological treatment in combination with the benefits of the laparoscopic technique.
Introduction
T
A radical gastrectomy with an extended lymphadenectomy is the only curative therapy that ensures good results in terms of survival for M0 advanced gastric cancer (AGC). 4 The first report of a laparoscopic gastrectomy (LG) for early gastric cancer (EGC) was published by Kitano et al. 5 Actually LG for the treatment of gastric cancer is accepted for EGC. Compared to the open approach laparoscopic technique is related to lower postoperative pain, faster return to the normal activities, reduction in length of hospital stay, lower rate of wound infection, and better esthetic results.6–9 In the KLASS trial, 1416 patients were randomized to the laparoscopic approach and the open approach, resulting in a significantly lower incidence of postoperative morbidity in the laparoscopic group (13.0% versus 19.9%, P = .001), while the intraoperative complications and mortality rates were comparable. 10
For the treatment of AGC, in which the extended lymphadenectomy is mandatory, the laparoscopic approach is still object of discussion due to its supposed technical difficulty and the lack of long-term results. In particular, it is debated if it is possible to perform a complete and safe lymph node dissection. The first reported LG with D2-extended lymph node dissection for the treatment of AGC was performed by Uyama in 2000. 11 Although there is increasing interest on this technique, randomized trials comparing the open technique with the laparoscopic one are lacking.6–8,12–14 The oncologic results appear to be comparable, as demonstrated in a recent retrospective study in which 1874 patients, 816 treated with open technique and 1058 treated with laparoscopic technique, were analyzed. No statistically significant differences were reported in terms of disease-free survival at 5 years, the results were stratified according to the stage of the disease (stage IB: 96.7% for laparoscopic versus 95.6% for open, stage IIB: 83.8% versus 78.6%, stage IIIA: 80.2% versus 73.7%, stage IIIB: 35.5% versus 49.0%, and stage IIIC: 42.9% versus 37.6%). 15
We started performing LG in selected patients with EGC in 2007. After an initial learning curve period we started performing this procedure in patients with AGC; the use of ultrasonic (Ultracision; Ethicon) or radiofrequency (Medtronic, MD) devices allowed to perform a correct lymphadenectomy.16–19 This study aims to analyze the oncological results, the intraoperative complications, and the short- and medium-term morbidity and mortality in patients with AGC who underwent subtotal laparoscopic gastrectomy (SLG) or total laparoscopic gastrectomy (TLG) with extended lymphadenectomy. The primary outcomes considered were the postoperative morbidity rate and the oncological results.
Materials and Methods
The clinical data from patients who underwent radical gastrectomy for AGC (≥T2) by a laparoscopic approach with the intent of curative surgery were retrospectively reviewed. From July 2007 to October 2015, 74 treated patients were recruited.
We analyzed demographics, the surgical risk (American Society of Anesthesiologists [ASA] score), 20 pTNM stage (according to the seventh edition of TNM staging system of gastric cancer), 21 histologic pattern of the tumor (according to Lauren's classification), 22 duration of surgery, rate of conversion, estimated blood loss, number of resected lymph nodes, type of gastrointestinal reconstruction, postoperative complication, mortality rate, length of stay, time to bowel opening and resumption of food intake, and overall and disease-free survival rate.
The variables considered were collected in an electronic database and expressed as mean, standard deviation, or percentage. The statistical analysis was performed with XLSTAT® software. The survival rate and the disease-free survival rate were expressed with the Kaplan–Meier curve. The Cox regression model was used for the analysis of predictors for complications and prognostic factors for survival. The P value considered for the statistical significance was .05.
The preoperative workup for each patient suitable of surgical treatment contemplated blood tests (blood count, coagulation panel, electrolytes, kidney and liver function, oncological markers); electrocardiogram and chest X-ray; upper-GI endoscopy with biopsy; thoracoabdominal CT scan with IV contrast; and anesthesiological evaluation for assessment of the surgical risk.
The selection criteria for the SLG were as follows: tumors involving the antrum, the pylorus, or gastric body; free margin of resection >5 cm; and appropriate vascular supply of the gastric remnant. The resection involves 2/3; of the viscus. The caudal section is performed at the duodenum below the pylorus. The cranial section is performed along a virtual anatomic line that goes from the right diaphragmatic pillar to the Van Goethem point. The reconstruction is performed with the Roux-en-Y or Omega anastomosis. A TLG was performed in patients with neoplasm localized at the fundus, the cardias, or at the body without a free margin of resection >5 cm; histological diagnosis of diffuse gastric cancer. The procedure contemplates the complete asportation of the stomach. The cranial section is performed at the subdiaphragmatic esophagus. The reconstruction is performed following the Orringer technique, and the gastrojejunal anastomosis is performed before stomach resection, exercising a slight traction, to facilitate the esophageal exposition allowing lesser anastomotic tension.
The patient is positioned in the supine position and in anti Trendelenburg position inclined at a 20° angle, with opened legs, with the left arm abducted and connected to the blood pressure cuff, the pulse oximeter, and the venous access. The surgeon stands between the patient's legs, the first assistant surgeon on his right and the second assistant surgeon, holding the camera while sitting, is positioned to the left of the first operator. The nurse at the instrumentary table is positioned between the surgeon and the first assistant. The videolaparoscopic equipment is placed behind the right shoulder of the patient, including the monitor, the insufflator, the camera control, the light source, and the irrigation–aspiration pump. The electrosurgical and dissection systems are placed on the right side of the bed (Fig. 1).

Left: position of the patient, the surgical team, and instrumentary. Right: position of the trocars, the fifth trocar in the left flank (5 mm) is positioned only for performing total gastrectomy.
Four trocars are used for the subtotal gastrectomy with the addition of a 5 mm trocar in the left flank for the total gastrectomy for the traction of the stomach (Fig. 1).
Results
From April 2007 to October 2015, 74 patients with histological definitive diagnosis of AGC approached with laparoscopic technique were retrospectively analyzed. The conversion rate was 14.9% (11/74). The reasons for the conversion were as follows: the need of associated multiple organ resections (pancreatosplenectomy and/or colonic resection) to ensure oncological radicality in 9 cases, in 2 cases the presence of massive adhesions. These 11 cases were therefore excluded from the study. Sixty-three patients were enrolled, 34 men and 29 women. The mean age was 70 ± 9.73 years (range 48–87); the average BMI was 27 ± 3 kg/m2 (range 21–31).
Table 1 shows the procedure performed: TLG or SLG according to the localization of the tumor. A SLG was performed in 43 (68.25%) patients and a TLG in 20 cases (31.75%).
No patients underwent neoadjuvant treatment, according to our oncologic protocol for AGC. Forty-seven (74.6%) patients received preoperative transfusion for anemia due to bleeding from the tumor, and 26 patients (41.3%) had dysphagia.
Considering the ASA classification of surgical risk, ASA 1 was found in 5 patients (7.9%), ASA 2 in 35 (55.6%) patients, and ASA 3 in 23 (36.5%) patients. Twenty-five (39.7%) patients presented with intraperitoneal adhesions at the intraoperative exploration as a consequence of previous surgeries.
The mean operative time was 150 ± 34 minutes (range 75–225 minutes). For the TLG the mean operative time was 155 ± 34 minutes (range 95–210 minutes), and for the SLG was 147 ± 34 minutes (range 75–225 minutes). An ultrasonic dissector device (Ultracision; Ethicon) was used in 42 procedures and a radiofrequency 5 mm dissector in 21 procedures (Medtronic), without evidences in hemostatic performance.
An extended lymphadenectomy was performed in all the operations, D3 in the first 23 cases and a D2 in the remaining cases, with a mean number of dissected lymph nodes of 21.4 ± 6.2 lymph nodes (range 8–40). A dissection with a total number of removed lymph nodes ≥16 was performed in 56/63 patients (88.89%).
During the SLG the Roux-en-Y reconstruction was performed in 31/43 (72.1%) cases and the Omega loop anastomosis in 12/43 (27.9%). In all the patients who underwent a TLG the reconstruction was performed with an esophagogastric anastomosis following the Orringer techniques with a transmesocolic loop.
The mean estimated blood loss was 204 ± 129 mL (range 50–500 mL).
All patients, according to our protocol, kept fasting until the fifth postoperative day, when upper gastrointestinal X-ray with oral contrast is performed to evaluate the anastomosis. Patients resumed oral food intake at a mean of 5.7 ± 1.9 days. The mean time for bowel opening was 3.0 ± 1.0 days. The mean time to discharge was 14.2 ± 16.0 days (range 7–116).
The postoperative morbidity rate was 25.39% (16/63 patients): 4 anemias requiring blood transfusion (6.35%), 3 bronchopneumonias (4.76%), 5 duodenal stump leaks (DSL) (7.94%), 3 anastomotic leakages (AL) of the gastroenteroanastomosis (4.76%), and 1 hemoperitoneum (1.59%). The rate of reoperation was 9.52% (6/63): 3 for duodenal stump leak, 2 for AL, and 1 for hemoperitoneum. The Table 2 summarizes the postoperative complications according to the classification of Clavien-Dindo (CD) 23 with the associated management.
Reference 23 .
CD, Clavien-Dindo.
The multivariate analysis using the Cox regression model did not show a correlation (P > .05) between the variable analyzed in the Table 3 and the occurrence of complications.
CI, confidence interval; OR, odds ratio; Y/N, yes/no.
The occurrence of DSL and AL was analyzed with the ASA score and patients age, respectively. ASA score for DSL group: ASA ≥2 3/23 (13.04%) versus ASA ≤2 2/40 (5%) (odds ratio [OR]: 2.8, P = .34). ASA score for AL group: ASA ≥2 3/23 (13.04%) versus ASA ≤2 0/40 (0%) (OR: 13.8, P = .04).
Mean age for DSL group was 75 ± 6.68 years versus 70 ± 9.86 years in no DSL group (P = .23). Mean age for AL group was 83 ± 0.46 years versus 70 ± 9.55 years in no AL group (P = .02).
No postoperative mortality was observed. The histologic pattern of the tumor was intestinal in 33 (52.38%) patients and diffuse in 30 (47.62%) patients, according to Lauren's classification. 21 The pTNM is reported in Table 4. The stage of the tumor was as follows: IB in 18 (28.57%), IIA in 13 (20.63%), IIB in 8 (12.70%), IIIA in 9 (14.29%), IIIB in 5 (7.93%), IIIC in 2 (3.17%), and IV in 8 (12.70%) patients.
Reference 20 .
The target for the postoperative follow-up was 60 months. Thirty-four patients completed the follow-up (53.9%). The mean postoperative follow-up time was 48.7 months (range 18–60 months). Patients who underwent adjuvant chemotherapy were 45/63 (71.43%).
At the end of the follow-up period 28/63 deaths have been reported, with an overall survival rate of 55.6%. Figure 2 shows the overall survival of the population and Figure 3 the overall survival according to each stage.
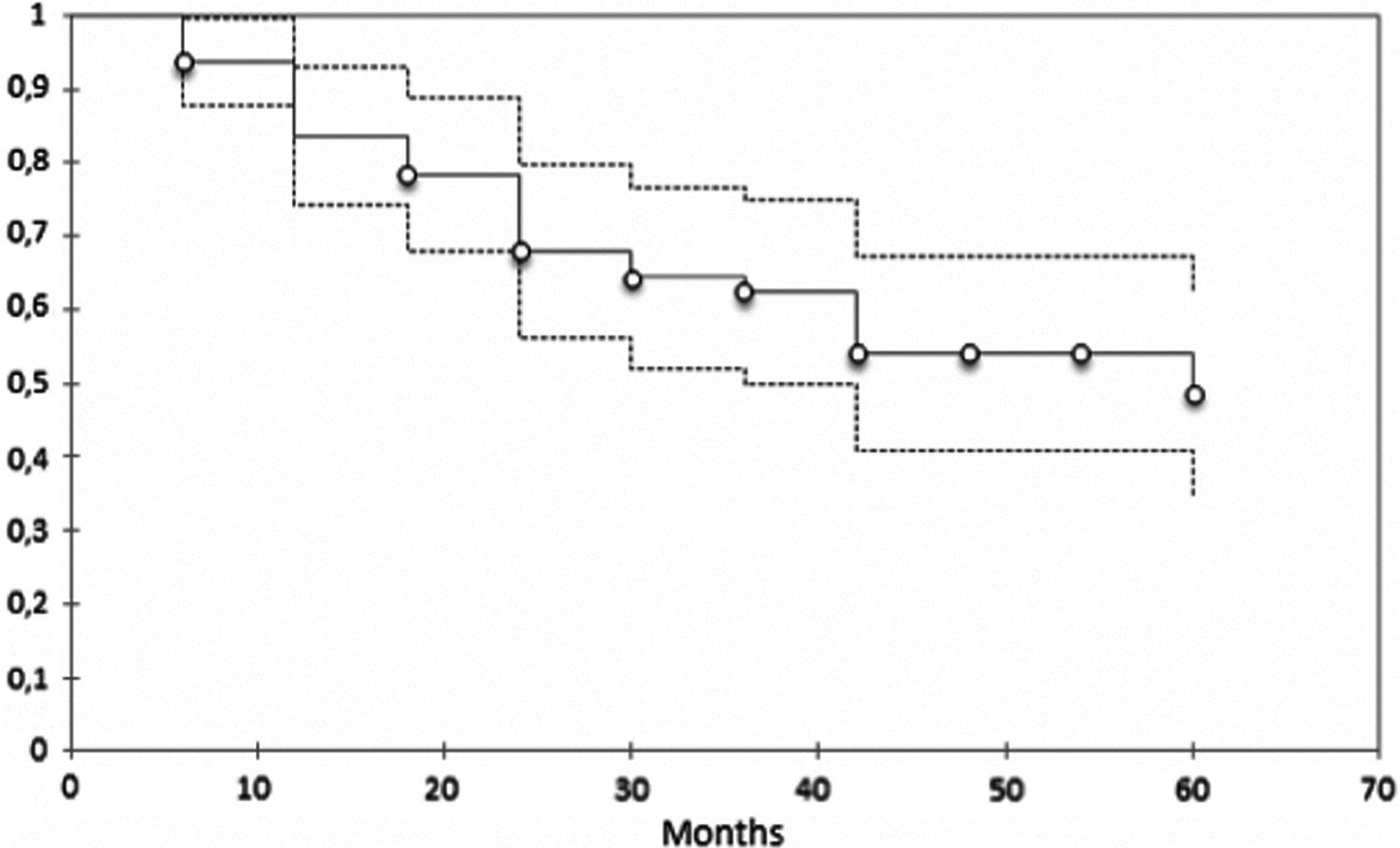
Overall survival of the population. The superior dotted line represents the upper limit of 95% confidence interval for the overall survival of the population. The middle line represents the overall survival of the population. The inferior dotted line represents the lower limit of 95% confidence interval for the overall survival of the population.

Overall survival according to each stage.
The overall survival rate at 12 months was 83.4%, at 24 months 67.9%, at 36 months 62.4%, at 48 months 54.0%, and at 60 months 48.6%.
Considering the overall survival according to the stage of the tumor: stage I had 94.1% at 12 months, 88.2% at 36 months, and 80.2% at 60 months; stage II 85.2% at 12 months, 57.7% at 36 months, and 51.9% at 60 months; and stage III 80.4% at 12 months, 60.3% at 36 months, and 20.1% at 60 months. Considering stage IV the mean survival was 19.5 months ±4.7 (95% confidence interval [CI]: 10.3–28.7 months).
Figure 4 shows that no statistically significant difference (P = .223) was seen in terms of overall survival in the subset of patients with a mean number of removed lymph nodes <16; this probably was due to the fact that in 88.89% (56/63) of patients the number of removed lymph nodes was ≥16.
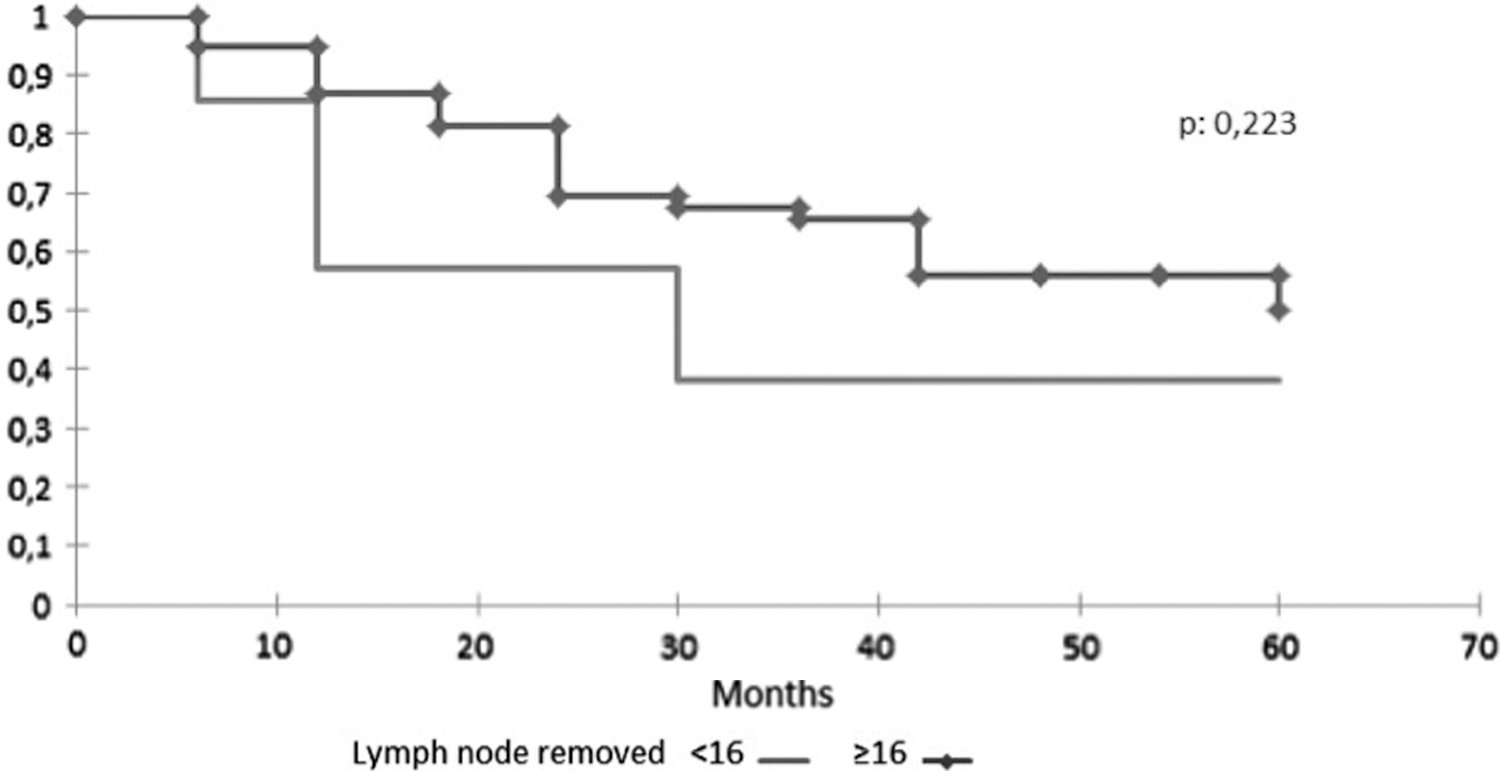
The overall survival in the two subgroups of patients, number of removed lymph node <16 or ≥16.
In Figure 5, which shows the results in terms of disease-free survival, compared to tumor recurrence (liver metastasis, local recurrence, lymph node, and peritoneal carcinomatosis) there was an average disease-free survival of 31.4 ± 1.8 months. The disease-free survival rates were 75.1% at 12 months, 66.4% at 24 months, 60.4% at 36 months, 50.7% at 48 months, and 42.7% at 60 months.

Disease-free survival of the population. The superior dotted line represents the upper limit of 95% confidence interval for the disease-free survival of the population. The middle line represents the disease-free survival of the population. The inferior dotted line represents the lower limit of 95% confidence interval for the disease-free survival of the population.
Discussion
Laparoscopic surgery for gastric cancer has rapidly developed according to the early benefits guaranteed by this minimally invasive technique. The treatment of EGC with the laparoscopic approach is now accepted,10,24 while the treatment of the AGC remains controversial, due to supposed technical difficulty in performing an adequate lymphadenectomy. Retrospective studies on EGC have also shown that there are no differences in terms of survival in patients operated with the laparoscopic approach compared to the open technique. Although the long-term results of the KLASS study are still to be published, EGC's laparoscopic treatment is now accepted. Regarding the treatment of AGC few data are available; however, both randomized and retrospective studies have shown that the number of lymph nodes removed and the disease-free survival do not differ significantly from the open technique.13,15,25
Huscher et al. reported the management of EGC and AGC with a total laparoscopic approach. They reported acceptable outcomes regarding the surgical resection, morbidity, and mortality in a cohort of 100 patients. 26
Seventy-four patients with AGC treated with laparoscopic approach were analyzed. The demographics of the population are comparable with the case studies in literature.27–31
The conversion rate, not always reported in other studies, was 14.9% (11/74). Adhesions due to previous surgery were present in 44.6% (33/74) of the patients at the intraoperative exploration. The reason for conversion was as follows: adhesions in 2 cases and multiorgan resection to ensure oncological radicality in 9 cases.
All the studies in literature confirm that the most important prognostic factor is the negativity of the margin of resection, R0.32,33 In fact, the 5-year survival in patients with gastric cancer T4 R0 ranges from 23% to 46%, while the survival rate drops in case of R1 resections, ranging from 0% to 17%. 34 In our series we have been able to perform a R0 resection in all cases. This technique did not increase the perioperative morbidity for the patients included in the study: using the Cox regression model, this variable was not significantly related to the incidence of postoperative complications, confirming the results of a recent multicenter Italian observational study. 35 Although other studies reported a higher percentage of complications, multiorgan resection plus gastrectomy was performed without improved survival. 36
The surgical procedures lasted an average of 150 ± 34 minutes, 155 ± 34 for TLG and 147 ± 34 minutes for the SLG. These data are at the lower limits of the ranges reported in the literature.12–14,37 This is probably due to the fact that almost all of the reported procedures were performed by a single operator, with a solid experience in the field of minimally invasive surgery.
An extended lymphadenectomy was performed in all the procedures. The D3 lymphadenectomy was carried out in the first 23 cases. This practice was then abandoned, not due to a highest risk of complications (P = .344), but following a recent randomized controlled trial in which was demonstrated no therapeutic advantages derived from the prophylactic lymphadenectomy of the para-aortic lymph nodes.38,39 In the analyzed population, the number of removed lymph nodes <16 or ≥16 was not significantly related to the overall survival of the patients (P = .233); this evidence may be due to the fact that in the majority of cases (88.9%) the number exceeded the standard of 16 lymph nodes.
DSL (7.94%) and AL (4.76%) rates resulted to be higher than other series reported in literature (1%–6.3%).40–42 Analyzing our patients series we found that the risk for DSL and AL is higher for patients with ASA score ≥2. DSL group: ASA ≥2 3/23 (13.04%) versus ASA ≤2 2/40 (5.26%) (OR: 2.8, P = .34). AL group: ASA ≥2 3/23 (13.04%) versus ASA ≤2 0/40 (0%) (OR: 13.8, P = .04). As reported in other studies, 43 we also noted that the occurrence of DSL and AL is higher for older patients: DSL group was 75 ± 6.68 years versus 70 ± 9.86 years (P = .22), and AL group was 83 ± 0.46 versus 70 ± 9.55 (P = .02).
Our results concerning the survival rate are partial, due to the fact that the oncological follow-up is still ongoing. At the time of the study the average time was 48.7 months. At the target follow-up of 60 months we reported an overall survival rate of 48.6%. These data were expressed with the Kaplan–Meier curve. Few data have been reported in literature regarding the medium term follow-up.
In our study, 12.8% of patients (8/63) belonged to stage IV. In these patients the decision to operate was due to bleeding from the tumor in 100% of the patients associated to dysphagia with endoscopic stenosis in 62.5% (5/8). A recent systematic review and meta-analysis on more than 3000 patients 44 showed that a gastrectomy performed in M1 patients with AGC significantly increases the median survival compared to those not treated (mean survival of 14.96 months versus 7.07). In our study, stage IV patients had a median survival of 19.5 months ±4.7 (95% CI: 10.3–28.7 months). The morbidity of this subpopulation is in line with the global population in our study; the average hospital stay was 11.7 days (range 6–20), with improved quality of life and a rapid onset of postoperative therapy.
In conclusion in the western world more than two thirds of patients with gastric cancer have a diagnosis at an advanced stage. Currently, laparoscopic surgery has been accepted for the treatment of EGC. This study, similar to others in literature,45,46 aims to assess the feasibility of laparoscopic surgery for advanced stages. We showed good results in terms of postoperative course, complications, and mortality. Laparoscopic surgery, when performed in minimally invasive surgery units, guarantees the respect of the surgical oncological criteria if compared to the open technique. This study, following many similar analysis from Asian authors, assessed the feasibility of the laparoscopic D2 lymphadenectomy. The use of ultrasonic or radiofrequency devices allows to perform a laparoscopic complete extended lymphadenectomy. The overall survival and disease-free interval reported are consistent with those reported in literature. Hence, the laparoscopic approach, when performed by experienced surgeons, ensures a correct oncological treatment in combination with the benefits of the laparoscopic technique.
Footnotes
Disclosure Statement
No competing financial interests exist.