
Abstract
Abstract
Background:
To report our experience with solo-surgeon, single-port laparoscopic anterior resection (solo SPAR) for sigmoid colon cancer.
Materials and Methods:
Data from sigmoid colon cancer patients who underwent anterior resections (ARs) using the single-port, solo surgery technique (n = 31) or the conventional single-port laparoscopic technique (n = 45), between January 2011 and July 2016, were retrospectively analyzed. In the solo surgeries, making the transumbilical incision into the peritoneal cavity was facilitated through the use of a self-retaining retractor system. After establishing a single port through the umbilicus, an adjustable mechanical camera holder replaced the human scope assistant. Patient and tumor characteristics and operative, pathologic, and postoperative outcomes were compared.
Results:
The operative times and estimated blood losses were similar for the patients in both treatment groups. In addition, most of the postoperative variables were comparable between the two groups, including postoperative complications and hospital stays. In the solo SPAR group, comparable lymph nodes were attained, and sufficient proximal and distal cut margins were obtained. The difference in the proximal cut margin significantly favored the solo SPAR, compared with the conventional AR group (P = .000).
Conclusion:
This study shows that solo SPAR, using a passive camera system, is safe and feasible for use in sigmoid colon cancer surgery, if performed by an experienced laparoscopic surgeon. In addition to reducing the need for a surgical assistant, the oncologic requirements, including adequate margins and sufficient lymph node harvesting, could be fulfilled. Further evaluations, including prospective randomized studies, are warranted.
Introduction
S
Efforts to reduce the number of required surgical personnel have also been considered for open surgery. These efforts have included the development of numerous instruments for providing traction, such as the Iron Intern (Automated Medical Products, New York, NY) and Omni-Tract (Minnesota Scientific, St. Paul, MN). After the introduction of laparoscopic surgery, a variety of camera-holding systems and simple traction instruments were developed to replace the scope assistant. The camera-holding systems have been developed in both active and passive forms and have been studied in phantom experiments and in clinical settings. Many reports suggest that the passive camera holders are comparable to human assistants and provide a cost efficient method for controlling the camera and holding instruments.1–3
Because the laparoscope replaces the direct vision of the surgeon, the role of camera assistant is particularly important during laparoscopic surgery. Any discordance between the surgeon and the scope assistant leads to surgeon stress and operative risks. 4 This might be one of the reasons for the development of various surgeon-controlled camera-holding systems.
In Korea there has been a surgical manpower shortage due to a long period of reduced applications for admission to general surgery residency programs. At our institution, SPLS has been performed in a variety of surgical settings since 2009; only the surgeon and the camera assistant participate in these SPLSs. Therefore, we planned solo-surgeon SPLS procedures, using a passive camera holder instead of the camera assistant, and have reported the safety and feasibility of this approach for appendectomies. 5
In the present study we investigated the feasibility and applicability of a single surgeon, assisted by a passive camera holder, performing single-port colonic resections. We also compared the results to those obtained during conventional SPLS. Specifically, both techniques were used to perform anterior resections (ARs) for sigmoid colon cancer, and the short-term outcomes and oncologic result were compared.
Patients and Methods
Between December 2013 and July 2016, 31 consecutive patients underwent solo-surgeon, single-port laparoscopic anterior resection (solo SPAR), with the assistance of a passive camera holder, at Daejeon St. Mary Hospital (affiliated with The Catholic University of Korea). They were retrospectively compared with those who underwent conventional SPLS AR, assisted by a human scope assistant (n = 45), between January 2011 and November 2013. All patients who were eligible for conventional laparoscopic procedures met the inclusion criteria. The exclusion criteria included advanced local disease, severe medical illness, or an emergent condition, such as a bowel obstruction or perforation. Patients who underwent a concurrent operation, such as cholecystectomy or hysterectomy, were excluded from the investigation.
The study was approved by the Ethics Committee of Daejeon St. Mary's Hospital, the Catholic University of Korea (Institutional Review Board code: DC17RISI0008). All surgeries were performed by 1 expert surgeon who was well experienced in performing SPLS. The protocol for colon SPLS has been standardized, as reported previously.6,7 A surgical assistant was included only during the anastomosis procedure for transanal application of circular staples (EEA; Ethicon, Somerville, NJ) and the open part of single-incision closures. During the open part of the procedure, the initial process, from the umbilical skin incision to the application of the single-port device, was performed by one surgeon using a self-retaining retractor (Lone Star 3307G; Cooper Surgical, Trumbull, CT), which replaced the assistant during fascial exposure (Fig. 1). In addition to the total operation time, this period between incision and port application and the setup time for installing the mechanical camera holder were tracked.

Utilization of a Lone Star retractor (3307G; Cooper Surgical, Trumbull, CT) for fascia exposure and access to peritoneal cavity.
Patient characteristics (age, sex, body mass index [BMI], American Society of Anesthesiologists [ASA] score, comorbidities, and previous abdominal surgeries), surgery-related parameters (operative time, blood loss, conversion to multiport or open surgery, postoperative length of stay, time to first flatus, time to first feeding, and perioperative complications), and pathologic parameters (tumor stage and number of harvested lymph nodes) were assessed and compared between groups. An intravenous analgesic (Pethidine HCl [25 mg] or Tramadol [50 mg]) was used for postoperative pain control; the number of patients requiring postoperative analgesia and the dosing frequencies were also recorded and compared. Complications were defined as the presence of any adverse event that developed perioperatively or within 30 days after the procedure. Small bowel obstruction was defined as the need for nasogastric tube insertion due to an inability to tolerate a solid diet in conjunction with concomitant radiologic findings suggestive of mechanical obstruction of small intestine. Urinary retention was defined as the need for reinsertion of a urinary catheter to allow urine passage, after the initial urinary catheter was removed. Pleural effusion was defined as the need for catheter drainage of fluid collected due to respiratory symptoms, such as dyspnea. Pancreatitis was defined as an absolute increase in serum amylase levels to ≥500 mg/dL and the use of drug therapy and bowel rest.
Solo SPAR procedure
The patient was placed in the lithotomy position with the right arm wrapped around the trunk. The operator stood on the right side of the patient. A vertical incision, 2–3 cm in length, was made at the umbilicus. A self-retaining retractor, as previously reported for use in SPLS appendectomies, 5 was used for fascial exposure and assessing the peritoneal cavity. The peritoneal cavity was accessed using the open method, assisted by the retractor. After entering the peritoneum, we inserted a commercial single port (OCTO port; Dalim), which had a 12-mm and two 5-mm trocars. After placing the port, pneumoperitoneum was established by insufflating the abdominal cavity to a pressure of 12 mmHg. At this time, the surgeon mounted an adjustable mechanical camera holder (Endoworld® LAP53 Holding Systems; Karl Storz, Tuttlingen, Germany) by anchoring it to the operating table rail. A passive camera holder consists of three bars connected with lockable joints. A rigid, 30° 10-mm laparoscope was attached to the camera holder and inserted through the 12-mm trocar. After the patient was adjusted into the Trendelenburg position, with the right side tilted down, the laparoscope (anchored to the tip of scope holder) was adjusted to provide the best surgical view; the scope holder's joint was locked to provide stable surgical vision (Fig. 2A). Thereafter, the surgical procedure, similar to conventional single-port laparoscopic AR except for the use of the camera holder, was performed. Our passive camera holder system allows scope repositioning, using either hand, by adjusting the center of the ball joint (Fig. 2B). The sigmoid colon was mobilized from the medial to the lateral side, and the dissection was extended superiorly to the level of the inferior mesenteric vessels. A high ligation was then performed using a 5-mm Hem-o-lok (Hem-o-lok Ligating Clips; Teleflex, Wayne, PA). To obtain the proper distal margins and handling, the upper rectum was mobilized and transected using a linear stapler (a 60-mm long, reticulating endoscopic GIA stapler; Covidien, Dublin, Ireland). The proximal colon was ligated, using nylon tape at 2-cm intervals, about 10 cm proximal to the cancer. The colon was transected, using the LigaSure sealing system (Covidien), between the two nylon ligations and placed into a specimen retrieval bag (LapBag; Sejong Medical, Paju, Korea); the specimen was extracted through the umbilical incision site. The ligated proximal colon stump was also extracorporealized through the umbilical incision site and prepared for anastomosis, that is, the tape was removed and an anvil was inserted into the remaining proximal colon. After returning the stump to the peritoneal cavity, an end-to-end anastomosis (EEA) was made using a circular stapler (EEA 28 or 31 mm; Ethicon) transanally. The anastomosis and intra-abdominal conditions were checked, and the operation was completed. Only the circular anastomosis and wound closure were performed with surgical assistance.

Intraoperative view of surgeon.
Statistical analysis
Prospectively collected data were retrieved from our electronic medical record system, and a retrospective analysis was performed. The data are presented as the numbers of patients and percentages, or as mean and standard deviation. Continuous data were analyzed using the Mann–Whitney and independent t-tests. Moreover, Fisher's exact test or χ2 test was used to compare categorical data; a two-sided P value <.05 was considered statistically significant. All data analyses were performed using SPSS, version 17, software (SPSS, Chicago, IL).
Results
Between January 2011 and July 2016, 102 patients with sigmoid colon cancer underwent single-port laparoscopic AR, with the assistance of either a human scope assistant or a mechanical camera holder. However, 26 patients were excluded because they underwent combined surgical procedures; therefore, 76 patients were evaluated (solo SPAR, 31; conventional SPLS AR, 45). The patient baseline characteristics are shown in Table 1. Both groups were balanced with respect to baseline characteristics, including age, sex, BMI, ASA grade, tumor site, and history of previous laparotomies.
Values are expressed as mean ± standard deviation unless otherwise specified.
ASA, American Society of Anesthesiologists; BMI, body mass index; CEA, carcinoembryonic antigen; solo SPAR, solo-surgeon single-port laparoscopic anterior resection; SPLS AR, single-port laparoscopic surgery anterior resection.
The surgical outcomes and postoperative courses are summarized in Table 2. There was no significant difference in the mean operative times between the solo SPAR (187 minutes) and conventional SPLS AR (192.7 minutes, P = .832) groups. The mean incision to port application time using the self-retaining retractor, without surgical assistance, and the mean setup time for installing the mechanical camera holder during solo SPAR group were 4 minutes and 50 seconds, respectively; this did not make a significant difference in the total operation time between the two groups. Even though the mean blood loss in the solo SPAR group (125.2 mL) was higher than in the conventional SPLS AR group (173.3 mL, P = .058), it did not reach statistical significance; 2 patients in the solo SPAR group did require blood transfusions. We also analyzed the solo SPAR operative times using a moving average method for the 31 patients. The results of this learning curve analysis indicated that the operative time stabilized after the first 10 consecutive patients (Fig. 3).
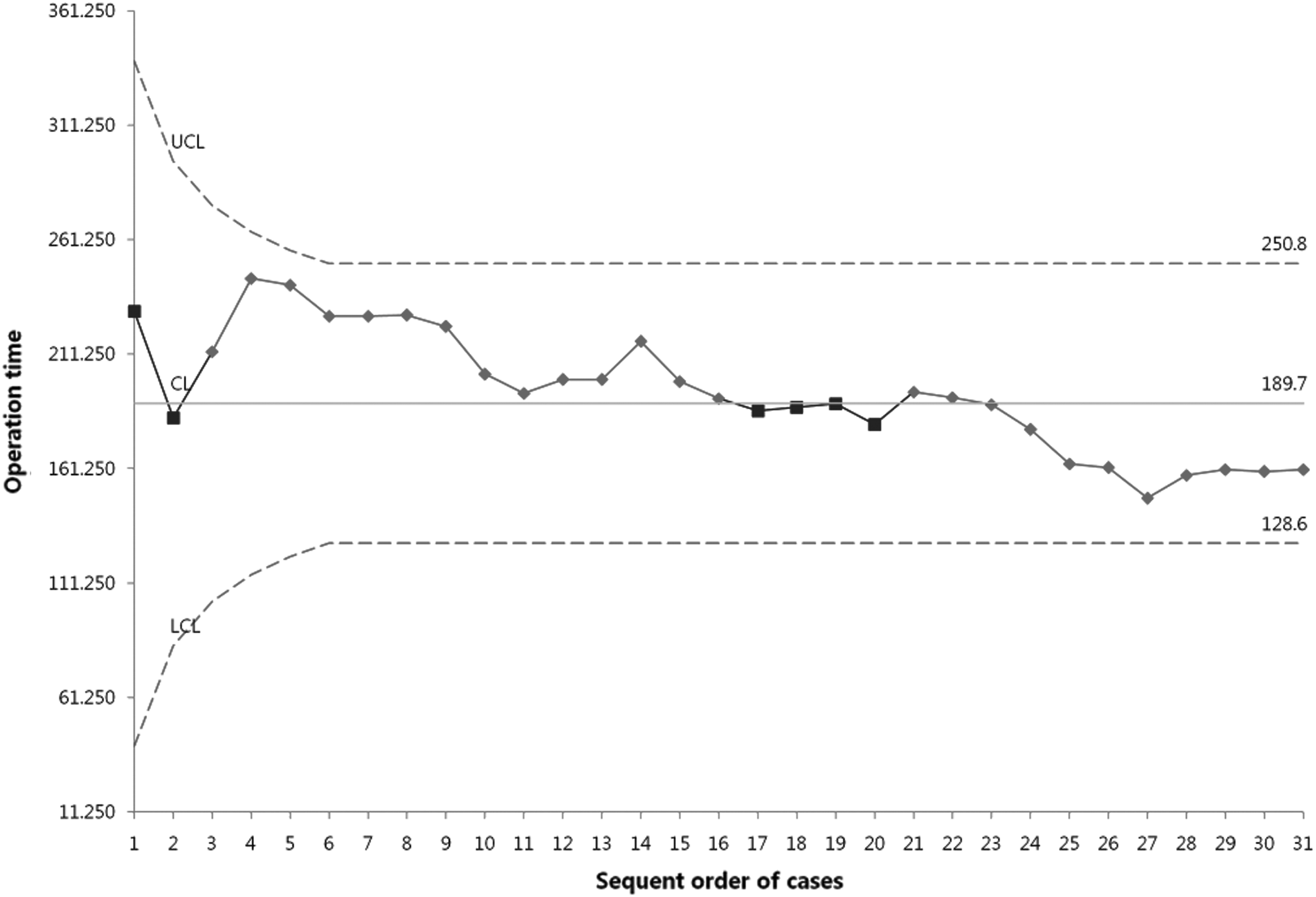
Learning curve analysis of solo surgeon single-port laparoscopic anterior resection using moving average method.
Values are expressed as mean ± standard deviation unless otherwise specified.
No other significant differences, including conversion to open or conventional laparoscopic surgery and intra- and postoperative morbidities, were found between the two groups. In the conventional SPLS AR group, the intraoperative complications comprised a single case of vascular injury. Postoperative anastomotic site leakage also occurred in 2 patients in the group. One patient, with minor leakage, was treated conservatively and discharged. The second required two reoperations, including single-port laparoscopic primary closure, with peritoneal lavage, and reanastomosis with loop ileostomy on postoperative days 4 and 13, respectively. He was discharged on day 42 after the second reoperation. In the solo SPAR group, there were two readmissions due to 1 patient developing an incisional hernia at the single-incision site. This was treated with single-port herniorrhaphy and dual phase onlay mesh, in months 11 and 14 after solo surgery. In the conventional SPLS AR group, one reoperation was required due to an anastomosis site stricture that developed 3 months after the first SPLS. Each group had 1 patient who required conversion to open colectomy. The reasons for conversion were a large tumor mass in the solo SPAR patient and severe dense adhesions in the conventional SPLS AR patient. There were no cases of conversion to human-assisted SPLS AR in the solo SPAR group. During the postoperative recovery period, the requirement for intravenous analgesics and the recovery times (time to passage of flatus, taking a soft diet, or postoperative hospital stay) were comparable between the two groups.
The pathologic outcomes are shown in Table 3. There were no significant differences between the groups in terms of pathologic data, including tumor cell differentiation, tumor depth, lymph node metastasis, and largest tumor diameter. Moreover, compared with the conventional SPLS AR surgery, solo-SPAR allowed comparable numbers of lymph nodes to be recovered (19.0 ± 8.9) and sufficient proximal and distal cut margins to be secured (proximal cut margin, 12.2 ± 3.3 cm; distal cut margin, 7.0 ± 3.2 cm). Unexpectedly, the solo SPAR group had significantly longer proximal cut margins (12.2 cm) than did the conventional SPLS AR group (8.2 cm, P = .000).
Values are expressed as mean ± standard deviation unless otherwise specified.
Discussion
Since laparoscopic surgery was introduced, it has shown advantages with respect to postoperative pain, recovery times, and possibly improved immune function.8–10 The small size of laparoscopic surgery incisions has resulted in not only less pain but also in fewer wound infections, less incisional herniation, fewer peritoneal adhesions, and better cosmesis. Laparoscopic surgery has also allowed operations to be performed with fewer personnel. Over time, the evolution of the technologies and techniques used in laparoscopic surgery has further minimized the damage to the abdominal wall and reduced the number of personnel required for surgery. As part of this evolutionary process, SPLS was introduced and various types of cameras and instrument holders were developed. SPLS is now performed in a variety of surgical fields. For colorectal disease, Bucher et al. and Remzi et al. reported the first successful SPLS in 2008.11,12 Recently, SPLS for colorectal cancer has been reported, including comparative studies with conventional laparoscopic treatment.13–15 Several review studies have also demonstrated comparable outcomes between single-port colectomies and conventional laparoscopic surgeries.16,17
In most laparoscopic surgeries, 1 or 2 additional assistants are needed, in addition to the assistant responsible for the camera. However, in SPLS, most procedures are commonly performed by the surgeon with the help of a camera assistant. The role of the camera assistant is to focus the camera around the surgical site and to maintain a steady field of view. This role can easily be replaced when using a camera-holding system. In addition, once the camera's field of view is set, there is an added advantage in that the mechanical device provides a constant and stable field of view, as long as no further manipulations are performed. We thought that if an appropriate camera holder system was applied to SPLS, an acceptable solo-surgeon surgery would be possible. Various camera and instrument holders have been described in the literature.1,3,18–21 Direct camera control and viewpoint adjustment can be realized by a passive camera holder that is manually controlled by the surgeon or by an active camera holder that is driven by motors and controlled with a user interface. 2 The passive camera holders appear to function as well as or better than the active devices.1,18
The present study was designed to compare the safety and efficacy of solo SPAR, using a passive camera holder, with conventional SPLS AR in patients with sigmoid colon cancer. Our data revealed that the short-term outcomes of solo SPAR were comparable to those obtained following conventional SPLS AR. There were no significant differences between the two groups in terms of operating time, estimated blood loss, postoperative complications, conversion rates, or blood loss. With respect to operative times, we assumed that the solo SPAR procedure might be longer due to the time needed by the surgeon to install the mechanical camera holder and to reposition the camera. However, a comparison of the operative times did not reveal any differences relative to the conventional SPLS AR procedure. Similar results for solo-surgeon surgeries involving laparoscopic colectomies have also been reported. 22 In a comparison of laparoscopic colectomies, with and without the aid of an active camera holder, Merola et al. demonstrated that the use of a robotic camera holder did not alter the length of the operative procedure. 23 In a comparative study investigating the clinical use of passive holders, Choi et al. compared patient outcomes after acute cholecystitis between a group treated with solo laparoscopic cholecystectomies using a passive scope holder and a group treated with conventional laparoscopic cholecystectomies with a scopist and showed no significant difference in the operative time, length of hospital stay, or morbidity. 24
To our knowledge, this is the first study investigating solo-surgeon surgery for single-port laparoscopic colectomies using a passive camera holder. As mentioned, the results were very similar to those obtained during conventional laparoscopic colectomies obtained at our institution. We can offer some suggestions regarding the operative time. The setup time for installing the passive holder was short (mean, 50 seconds), and the process was simple. Few repositionings of the camera holder were required during the surgical procedure, and the time required for those repositionings was short. In a literature review regarding the clinical value of camera and instrument holders in minimally invasive surgery, Jaspers et al. concluded that camera positioning, by the surgeon, is intuitive and efficient, leading to few repositionings. The surgeon's repositioning of the camera appears to involve a similar number of actions and a similar amount of time as when the surgeon has a human assistant. 2
In this series, solo SPAR was successful in all patients, except 1 who required conversion to laparotomy due to the large tumor size. Otherwise, no intraoperative and only seven minor postoperative complications occurred in the solo SPAR group. The postoperative complication rate was 22.6%, which is comparable to conventional SPLS AR. However, two incisional hernias occurred as late complications in the solo SPAR group and were treated with single posthernia repair surgeries. However, there were no incisional hernias in the conventional SPLS AR group. We could not find any association between the solo surgery and incisional hernia occurrence. When the wound is closed, the closure involves a human assistant, as it does during conventional SPLS AR. Thus, this complication is considered to be related to the SPLS.
In this study, we also compared the pathologic specimens obtained during the solo SPAR and conventional SPLS AR surgeries in an attempt to evaluate the adequacy of the specimens. The numbers of lymph nodes harvested and the margins and lengths of the resected specimens were adequate, and the results showed similar outcomes to conventional SPLS AR.
The current study also revealed several other considerations associated with solo SPAR. As expected, solo SPAR offered a more stable view of the surgical field because the surgeon was controlling the camera manipulations, unlike in conventional SPLS AR where an assistant is manipulating the camera. Thus, only the desired movements were occurring. Another benefit was that solo SPAR allowed the surgeon a high degree of freedom of movement. The passive camera holder consisted of a thin linear rod that replaced the camera assistant who typically shares the limited bedside space with the surgeon. This provided additional clearance around the patient. The camera holder is also easy to adjust and does not lead to prolonged operating times. In addition, rapid learning curves for the use of robotic camera-holding systems have been previously reported and are similar to those observed in our study. 25 Conversely, concerns that requiring the surgeon to reposition the camera would result in increased operating times were alleviated by the present results. ARs are surgical procedures that are mainly limited to a single abdominal quadrant. We previously reported the feasibility of solo surgeries involving a single abdominal quadrant, that is, solo SPLS appendectomy. 26 However, in cases where the surgical field extends into other quadrants, such as irrigating the Morrison pouch or looking for missing intraperitoneal surgical gauze, having the surgeon responsible for relocating the camera holder along the table rail or handling all maneuvers across the other quadrant was time consuming and intricate. Another concern for solo surgery is the management of unexpected situations that may arise during the surgery. In this series, there were no uncontrollable situations, such as major bleeding. However, the availability of additional prepared staff is mandatory in case an emergency situation arises.
We acknowledge that this study has several limitations, including the small sample size, lack of long-term oncologic outcomes, and the retrospective review of prospectively collected data. Furthermore, a selection bias for surgical candidates and the proficiency of the SPLS operator could be other limitations of the study. Nevertheless, in this study, solo SPAR was performed in consecutive patients with sigmoid colon cancer, and the patient distribution was well balanced with the conventional SPLS AR group. To our knowledge, this is the first report of solo-surgeon, single-port colectomies involving the use of a camera holder. Thus, the present study could be useful data to experienced single-port surgeons who are planning to use a camera-holding system.
In conclusion, in this comparative analysis of solo SPAR, using a passive camera holder, and conventional SPLS AR, we examined surgical outcomes, oncologic safety, and the learning curve of the solo procedure. We conclude that solo, assisted by a passive camera holder, may be a safe and feasible surgical technique when performed by a surgeon well-experienced with conventional SPLS; a relatively short learning period is required. However, the technique and the type of camera holder used warrant further investigation, including more extensive, prospective comparative studies.
Footnotes
Disclosure Statement
No competing financial interests exist.